Abstract
Background:
Brain natriuretic peptide (BNP) and N-terminal proBNP (NT-proBNP) are prognostic biomarkers. Although these 2 peptides differ with regard to biological characteristics, there are few reports on the differences between BNP and NT-proBNP with regard to cardiovascular events or according to sex.
Methods and Results:
Between 2005 and 2012, this study analyzed 3,610 of 4,310 Japanese outpatients (mean age, 65 years; men, n=1,664; women, n=1,947) with a history of at least one cardiovascular event who were recruited to the Japan Morning Surge-Home Blood Pressure Study. During an average 4-year follow-up, there were 129 cardiovascular events. Both median BNP (21.1 pg/mL; IQR, 10.9–40.6 pg/mL vs. 16.2 pg/mL, IQR, 7.2–36.2 pg/mL, P<0.001) and median NT-proBNP (54.7 pg/mL; IQR, 30.2–102.6 pg/mL vs. 44.9 pg/mL, IQR, 20.7–92.6 pg/mL, P<0.001) were significantly higher in women than in men. A 1-SD increment in log-transformed BNP (hazard ratio [HR], 2.18; 95% CI: 1.53–3.10) and NT-proBNP (HR, 2.39; 95% CI: 1.73–3.31) was associated with a significant increase in cardiovascular events in women; in men, only NT-proBNP showed this association. There was an interaction between log-transformed BNP (P=0.007) or NT-proBNP (P=0.001) and cardiovascular events according to sex.
Conclusions:
Both BNP and NT-proBNP predicted cardiovascular outcomes in a large Japanese clinical population. BNP and NT-proBNP were significantly stronger predictors in women than in men.
Serum levels of natriuretic peptide hormones, in particular brain natriuretic peptide (BNP) and N-terminal pro-BNP (NT-proBNP), are useful biomarkers for ruling out heart failure,1–3
as well as strong prognostic markers for cardiovascular events in not only heart failure and hypertensive populations but also the general population.4–6
BNP, in contrast to NT-proBNP, is biologically active when released into the circulation.7,8
In some studies comparing the utility of BNP and NT-proBNP for heart failure screening and prognostic value for cardiovascular events, no practical difference was observed.3,9
The value of those studies, however, was limited by their evaluation of selected patients. One study involved a small sample of patients with suspected heart failure,3
and another study was performed in a stable and symptomatic heart failure population.9
In addition, both BNP and NT-proBNP are higher in women than in men.10–12
Although the effects of BNP or NT-proBNP on prognosis have been reported according to sex in heart failure populations, the results are conflicting.13,14
This may explain why data were unable to discriminate between BNP and NT-proBNP in heterogeneous heart failure populations, yielding inconsistent results.
The aim of this study was therefore to investigate differences between BNP and NT-proBNP with regard to cardiovascular events and extend the search for this difference to sex, in a large clinical population with cardiovascular risk factors.
Methods
Subjects
We used baseline data from the Japan Morning Surge-Home Blood Pressure (J-HOP) Study. The protocol of the J-HOP study has been published (Supplementary File 1).15
Briefly, the J-HOP study is a prospective observational study (University Hospital Medical Information Network Clinical Trials Registry, UMIN000000894) evaluating the use of home blood pressure (BP) measurements to predict cardiovascular events between January 2005 and May 2012 in 4,310 Japanese ambulatory patients who had a history of and/or risk factors for cardiovascular disease (CVD) as follows: hypertension, dyslipidemia, diabetes, glucose intolerance, metabolic syndrome, chronic kidney disease (CKD), history of CVD, atrial fibrillation, current smoking, chronic obstructive pulmonary disease, or sleep apnea syndrome. All participants provided written informed consent for their data to be used, and the Institutional Review Board of Jichi Medical School approved the study.
Of the 4,310 patients enrolled in the J-HOP study, we excluded 691 lacking data for both BNP and NT-proBNP. A final total of 3,619 patients was included in the present analysis. Diabetes was defined as fasting glucose ≥126 mg/dL and/or a casual glucose ≥200 mg/dL or treatment for diabetes. Dyslipidemia was defined as total cholesterol ≥240 mg/dL or treatment for dyslipidemia. CKD was defined as the presence of proteinuria or estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m2. Past history of CVD was defined as diagnosed angina pectoris, myocardial infarction (MI), or stroke. The average of 3 office BP measurements carried out in a sitting position at 2 clinic visits were taken by a physician or nurse using an upper arm cuff and an oscillometric BP device (HEM-5001; Omron Healthcare, Kyoto, Japan), and used in the present study.
Natriuretic Peptides
Fasting morning blood and spot urine samples were collected at study enrollment. Plasma BNP was measured with a chemiluminescent enzyme assay (MI02 Shionogi BNP; Shionogi, Osaka, Japan). NT-proBNP was measured with an automated Cobas analyzer using an electrochemiluminescent immunoassay (Roche Diagnostics, Japan).
Outcome Measurement
The primary outcome was the first occurrence of a cardiovascular event during the study period, including fatal and non-fatal stroke and fatal and non-fatal coronary artery disease, defined as acute MI, angina pectoris requiring percutaneous coronary intervention, and sudden death ≤24 h after abrupt onset of symptoms. If events occurred on ≥2 occasions, the first occurrence was included in the analysis (Supplementary File 1).
Statistical Analysis
Data are expressed as mean±SD, median (IQR), or percentage. The distribution of BNP and NT-proBNP was highly skewed and was log-transformed before the statistical analysis. Continuous variables were compared using Student’s t-test, and categorical variables were compared using the chi-squared test. Univariate associations were assessed using Pearson’s correlation. Cumulative incidences of cardiovascular events in quartiles of BNP and NT-proBNP in the entire group and according to gender were plotted as Kaplan-Meier curves, and the differences were assessed with the log-rank test. The hazard ratio (HR) and 95% CI of cardiovascular events in quartiles of BNP and NT-proBNP in the entire group and according to gender were calculated using unadjusted and adjusted Cox regression analyses after adjustments for traditional cardiovascular risk factors, that is, age, gender, body mass index (BMI), smoking, pre-existing CVD, total cholesterol, high-density lipoprotein cholesterol (HDL-C), diabetes, use of an antihypertensive drug or statin, eGFR, and clinic-measured systolic blood pressure (SBP). The proportionality assumption for the Cox analysis was confirmed graphically and via the inclusion of a time×BP interaction. In the group stratified by sex, Cox regression analysis was performed with adjustment for similar covariates except for gender. To evaluate the association of elevated BNP and NT-proBNP with cardiovascular events, we used log-transformed BNP and NT-proBNP per 1 SD as a continuous variable in a Cox regression analysis that included similar covariates in the entire group and according to gender. Moreover, we used Cox proportional hazard regression to calculate adjusted HR, using dichotomized BNP (35 pg/mL as threshold) and NT-proBNP (125 pg/mL as threshold), which are recommended by the European Society of Cardiology for subjects with suspected heart failure.16
All statistical analysis was performed with Stata version 15.0 (StataCorp, College Station, TX, USA). P<0.05 was considered statistically significant for all tests.
Results
Baseline Characteristics
There were no significant differences in baseline characteristics between participants included in the current study and those who were not included (Table S1). The participant demographic and clinical characteristics according to gender are given in
Table 1. The proportion of women was 53.9%. Women were older than men. The prevalence of cardiovascular risk factors was higher in men than in women. Average BNP and NT-proBNP ere significantly higher in women than in men. There was a significant association between log-transformed BNP and log-transformed NT-proBNP in both groups (men, r=0.790, P<0.001; women, r=0.838, P<0.001).
Table 1.
Subject Baseline Characteristics vs. Sex
| |
Women
(n=1,951) |
Men
(n=1,668) |
P-value |
| Age (years) |
65.7±10.2 |
64.3±11.0 |
<0.001 |
| BMI (kg/m2) |
24.3±3.8 |
24.2±3.1 |
0.818 |
| Current smoker |
3.6 |
22.0 |
<0.001 |
| Daily drinker |
7.6 |
51.3 |
<0.001 |
| Antihypertensive medication |
77.2 |
81.5 |
0.001 |
| Diabetes |
22.2 |
27.2 |
<0.001 |
| Statin use |
28.2 |
18.8 |
<0.001 |
| Pre-existing CVD |
8.3 |
18.2 |
<0.001 |
| TC (mg/dL) |
208.6±31.6 |
195.7±32.3 |
<0.001 |
| HDL-C (mg/dL) |
60.6±14.8 |
54.5±14.9 |
<0.001 |
| Office SBP (mmHg) |
141.6±16.7 |
141.4±15.6 |
0.771 |
| Office DBP (mmHg) |
80.9±10.1 |
82.6±10.2 |
<0.001 |
| BNP (pg/mL) |
21.1 (10.9–40.6) |
16.2 (7.2–36.2) |
<0.001 |
| NT-proBNP (pg/mL) |
54.7 (30.2–102.6) |
44.9 (20.7–92.6) |
<0.001 |
Data given as mean±SD, median (95% CI) or %. BMI, body mass index; BNP, brain natriuretic peptide; CI, confidence interval; CVD, cardiovascular disease; DBP, diastolic blood pressure; HDL-C, high-density lipoprotein cholesterol; NT-proBNP, N-terminal-pro-brain natriuretic peptide; SBP, systolic blood pressure; TC, total cholesterol.
During a mean follow-up of 4.0±2.1 years (14,490 person-years), 129 cardiovascular events were observed. In the entire group, the incidence of cardiovascular events increased with increasing BNP and NT-proBNP quartiles, on Kaplan-Meier curve analysis (Figure 1). On unadjusted Cox regression analysis, the top quartile of BNP was a risk factor for cardiovascular events compared with the lowest quartile in men (HR, 2.88; 95% CI: 1.49–5.56; P=0.002) and in women (HR, 3.82; 95% CI: 1.66–8.80; P=0.002) and the top quartile of NT-proBNP was a risk factor for cardiovascular events compared with the lowest quartile in men (HR, 3.56; 95% CI: 1.83–6.96; P<0.001) and in women (HR, 6.28; 95% CI: 2.19–18.04; P=0.001). On multivariable Cox regression analysis after adjustment for age, sex, BMI, smoking, diabetes, total cholesterol and HDL-C, use of an antihypertensive drug or statin, past history of CVD, eGFR, and clinic-measured SBP, the top quartile of BNP was associated with a higher risk of cardiovascular events (Table 2). This association was similar for the quartiles of NT-proBNP. A 1-SD increment in log-transformed BNP was associated with a significant increase in cardiovascular events (HR, 1.34; 95% CI: 1.10–1.63, P=0.004). The association between a 1-SD increment in NT-proBNP and cardiovascular events was also similar (HR, 1.49; 95% CI: 1.24–1.79, P<0.001).
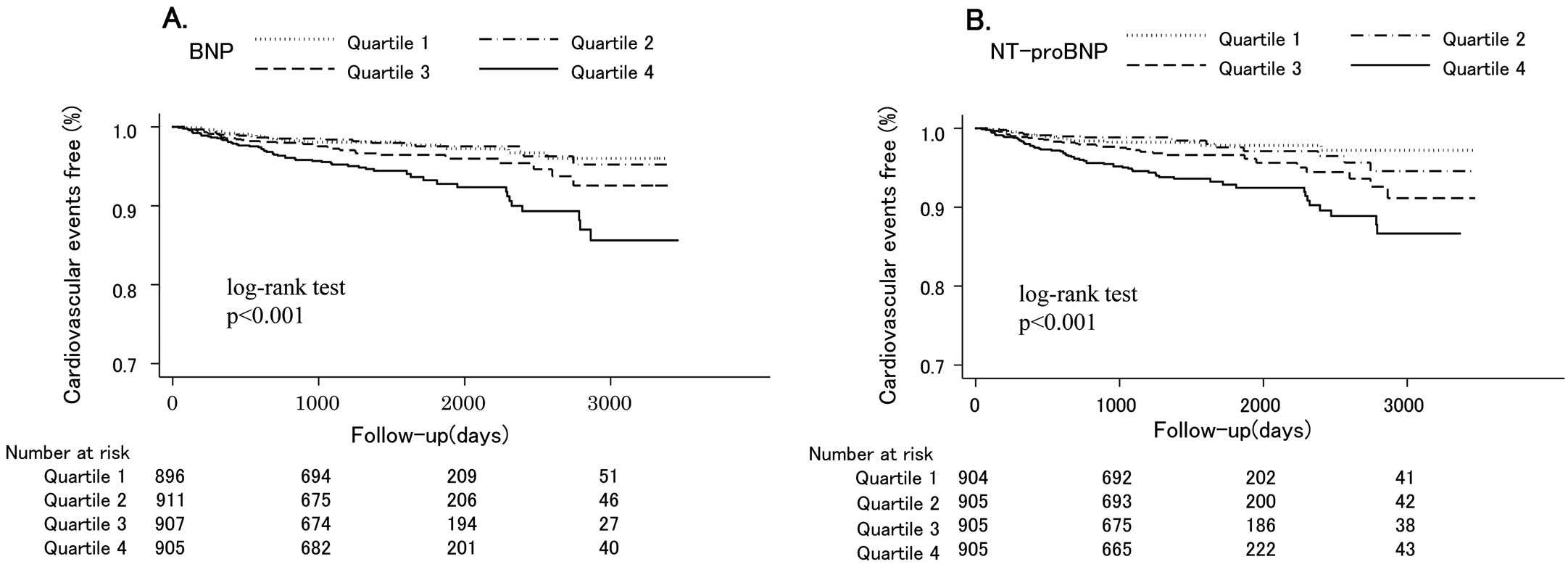
Table 2.
Risk of Cardiovascular Events vs. BNP and NT-proBNP Quartile (n=3,619)
| |
BNP |
NT-proBNP |
Range
(pg/mL) |
No. events/
Total no. subjects |
HR
(95% CI) |
Range
(pg/mL) |
No. events/
No. subjects |
HR
(95% CI) |
| Quartile 1 |
≤9.2 |
20/896 |
Re. |
<25.52 |
17/904 |
Ref. |
| Quartile 2 |
9.3–18.7 |
20/911 |
1.01 (0.54–1.91) |
25.54–50.35 |
18/905 |
0.96 (0.49–1.89) |
| Quartile 3 |
18.8–38.5 |
32/907 |
1.39 (0.77–2.52) |
50.47–97.34 |
33/905 |
1.71 (0.93–3.16) |
| Quartile 4 |
≥38.6 |
57/905 |
1.90 (1.07–3.36)* |
>97.37 |
61/905 |
2.48 (1.36–4.49)** |
*P<0.05, **P<0.01 vs. Reference. HR are adjusted for age, sex, BMI, smoking, pre-existing CVD, TC, HDL-C, diabetes, use of an antihypertensive drug or statin, estimated glomerular filtration rate, and clinic-measured SBP. BNP, brain natriuretic peptide; HR, hazard ratio; NT-proBNP, N-terminal-pro-brain natriuretic peptide. Other abbreviations as in Table 1.
In women, increased BNP and NT-proBNP quartiles were associated with cardiovascular events on Kaplan-Meier curve analysis (Figure 2). These associations were observed in men. On multivariable Cox regression analysis after adjustment for age, BMI, smoking, diabetes, total cholesterol and HDL-C, use of an antihypertensive drug or statin, past history of CVD, eGFR, and clinic-measured SBP, the top quartiles for both BNP and NT-proBNP were associated with a higher risk of cardiovascular events in women, whereas only NT-proBNP had this association in men (Table 3). A 1-SD increment in log-transformed BNP and NT-proBNP was associated with a significant increase in cardiovascular events in women, whereas only NT-proBNP had this association in men. There was an interaction between log-transformed BNP or NT-proBNP and cardiovascular events according to sex (Table 4). On further analysis, both BNP and NT-proBNP were associated with cardiovascular events, irrespective of sex (Table S2). Although the HR of BNP and NT-proBNP was high in women compared with men, the interaction between NT-proBNP and cardiovascular events according to sex was marginal.

Table 3.
Risk of Cardiovascular Events vs. BNP and NT-proBNP Quartiles and Sex
| |
BNP |
NT-proBNP |
Range
(pg/mL) |
No. events/
Total no. subjects |
HR
(95% CI) |
Range
(pg/mL) |
No. events/
Total no. subjects |
HR
(95% CI) |
| Men |
| Quartile 1 |
≤7.2 |
12/417 |
Ref. |
<20.67 |
11/417 |
Ref. |
| Quartile 2 |
7.3–16.1 |
15/413 |
0.97 (0.44–2.10) |
20.72–44.86 |
13/417 |
1.03 (0.45–2.34) |
| Quartile 3 |
16.2–36.1 |
21/421 |
1.22 (0.58–2.59) |
44.90–92.36 |
19/417 |
1.25 (0.57–2.72) |
| Quartile 4 |
≥36.2 |
34/417 |
1.49 (0.72–3.10) |
>92.64 |
39/417 |
2.25 (1.06–4.75)* |
| Women |
| Quartile 1 |
≤10.8 |
7/483 |
Ref. |
<30.15 |
4/487 |
Ref. |
| Quartile 2 |
10.9–21.0 |
3/491 |
0.45 (011–1.78) |
30.19–54.68 |
7/488 |
1.33 (0.38–4.69) |
| Quartile 3 |
21.1–40.5 |
11/488 |
1.22 (0.44–3.37) |
54.70–102.5 |
11/488 |
2.29 (0.69–7.61) |
| Quartile 4 |
≥40.6 |
26/489 |
2.85 (1.11–7.32)* |
>102.6 |
25/488 |
4.22 (1.33–13.37)* |
*P<0.05 vs. Reference. HR are adjusted for age, BMI, smoking, pre-existing CVD, TC, HDL-C, diabetes, use of an antihypertensive drug or statin, estimated glomerular filtration rate, and clinic-measured SBP. Abbreviations as in Tables 1,2.
Table 4.
Prognostic Power for Cardiovascular Events
| |
HR |
95% CI |
P for interaction |
| Log BNP (per 1 SD increase) |
| Men |
1.15 |
0.91–1.46 |
0.007 |
| Women |
2.18 |
1.53–3.10** |
| Log NT-proBNP (per 1 SD increase) |
| Men |
1.29 |
1.04–1.60* |
0.001 |
| Women |
2.39 |
1.73–3.31** |
*P<0.05, **P<0.01. HR are adjusted for age, BMI, smoking, pre-existing CVD, TC, HDL-C, diabetes, use of an antihypertensive drug or statin, estimated glomerular filtration rate, and clinic-measured SBP. Abbreviations as in Tables 1,2.
Discussion
In the present study, both BNP and NT-proBNP were significantly higher in women than in men in a large Japanese population of individuals with a history of and/or risk factors for CVD. This is consistent with previous studies.10–12
Both BNP and NT-proBNP were independently associated with cardiovascular events, irrespective of sex. Interestingly, the association between BNP or NT-proBNP and cardiovascular events in women was significantly stronger than in men.
Both BNP and NT-proBNP have been used for heart failure screening and as prognostic biomarkers in general and clinical populations.4–6
These natriuretic peptides are produced by the cleavage of precursor proBNP, and exhibit differences in biological characteristics, such as bioactivity, half-life, and involvement in metabolic processes.7,8
Although several reports have compared the clinical utility of BNP and NT-proBNP, there was no significant difference in diagnostic accuracy for screening of symptomatic heart failure in a small population,3
in prognostic power for all-cause mortality and morbidity, or in hospitalization for heart failure in a stable and symptomatic heart failure population.9
The present results have confirmed previous reports that both BNP and NT-proBNP provide prognostic power for cardiovascular events in a large clinical population with cardiovascular risk factors.
In the present study a significant interaction was noted between male and female sex according to the prognostic power of BNP and NT-proBNP for cardiovascular events. In addition, the HR of the top quartile compared with that for the lowest quartile for BNP and NT-proBNP (Table 3), and the HR for a 1-SD increment in log-transformed BNP and NT-proBNP (Table 4) was approximately 2-fold higher in women than in men. Although sex differences in the effect of BNP or NT-proBNP for cardiovascular events have been unclear, the present findings support the previous studies. Kara et al compared the prognostic value of BNP and NT-proBNP for cardiovascular events in 3,589 individuals in the general population.17
Although they found that both higher BNP and higher NT-proBNP were associated with cardiovascular events in men, only BNP had this association in women.17
Ballo et al reported that in a population with hypertension and/or type 2 diabetes, NT-proBNP above the sex-specific 80th percentile was associated with a 3.6-fold higher risk of cardiac events in women and a 2.9-fold higher risk in men, compared with that below the 80th percentile; moreover, there was an interaction for risk between men and women.18
In contrast, sex differences in the association of BNP or NT-proBNP with cardiovascular events in patients with heart failure or suspected heart failure are controversial. Christ et al reported that in patients with acute dyspnea, abnormal BNP (>500 pg/mL) was associated with a 5.1-fold and a 1.8-fold increased risk of cardiac events in men and women, respectively, compared with the risk of BNP ≤500 pg/mL; there was also a significant interaction for this association between men and women,13
whereas in a large registry of admitted heart failure patients the ability of BNP to predict in-hospital mortality was similar between men and women.14
Thus, the prognostic value of BNP and NT-proBNP may be greater for women than men in the population without clinical heart failure. In contrast, when cardiovascular risk is high, the differential prognostic value of BNP and NT-proBNP according to sex might be weakened.
Although this study was not conducted to determine the pathological mechanism accounting for the differential effect of natriuretic peptide for cardiovascular outcomes according to sex, a previous study may have partially explained this phenomenon. Chen et al investigated age-related cardiac remodeling and functional changes according to sex differences in a large, healthy population.19
In that study, women had a steeper slope for echocardiographic increase in left ventricular mass with aging compared with men, and the results were strongly associated with NT-proBNP.19
Increased left ventricular mass is a powerful predictor of cardiovascular events,20
thus explaining the present results showing superior prognostic power for BNP and NT-proBNP in women than in men, given that the present patients were relatively older. Moreover, endogenous sex hormones in postmenopausal women might have affected the association between natriuretic peptide and cardiovascular outcomes in women. In the present study, the average age of the female subjects was 65 years. Creatsa et al reported that, in postmenopausal women, a higher free androgen index, as one of the markers of circulating androgen, was associated with subclinical organ damage,21
in the same way that carotid artery intima-media thickness and pulse wave velocity are markers of cardiovascular risk.22,23
Glisic et al reported that a higher free androgen index was associated with lower NT-proBNP in postmenopausal women.24
From these two previous studies, we can thus speculate that higher androgen may decrease natriuretic peptide, whereas it may increase cardiovascular risk in postmenopausal women. As a result, even if the absolute circulating natriuretic peptide level is similar between a man and a woman, the woman might be at higher risk of cardiovascular events than the man.
In this study, both BNP and NT-proBNP were higher in women than in men. This is consistent with previous reports. Several studies have reported that both BNP and NT-proBNP are significantly higher in women than in men in the general population, regardless of age or health status.10–12,25
The physiologic basis for these sex differences in natriuretic peptide is unclear, although a stimulatory effect of female sex hormones on natriuretic peptide gene expression has been proposed.26,27
A prior population-based cohort study reported that BNP was 21% higher in women on hormone replacement therapy (HRT) than in those not on HRT.10
This suggests that BNP production may be sensitive to estrogen regulation and production.
In the present study, on unadjusted Cox regression analysis the top quartile of BNP was a risk factor for cardiovascular events compared with the lowest quartile in men, but this association disappeared after adjustment for covariates. A higher prevalence of smoking, past history of CVD and use of antihypertensive medication was also noted in men compared with women. Therefore, the weak association between BNP and cardiovascular events in men might be attributed to the different characteristics between men and women in this study. This should be confirmed in another population.
This study had several limitations. Some patients had high BNP or NT-proBNP. Although participants with symptoms of heart failure were not enrolled in the J-HOP study, we cannot completely exclude the possibility that the present cohort included patients with compensated heart failure. Given that this was an observational study, we had no information on drug treatment effects on natriuretic peptide levels during follow-up. In addition, there was a lack of data on sex hormones or menopause status, despite the possible relationship between estrogen level and the prognostic value of NT-proBNP.
Conclusions
Based on a large Japanese population with cardiovascular risk factors, both increased BNP and NT-proBNP were associated with cardiovascular events, and BNP and NT-proBNP were significantly stronger predictors in women than in men.
Acknowledgments
We gratefully acknowledge the numerous study investigators, fellows, nurses, and research coordinators at each of the study sites, who have participated in the J-HOP study. The physicians who participated in this study and the participating centers are listed in
Appendix S1. We also gratefully acknowledge Ms Kimiyo Saito for coordination and data management, and Ms Ayako Okura for editorial assistance.
Disclosures
K. Kario has received research grants from Teijin Pharma Limited, Novartis Pharma K.K., Takeda Pharmaceutical Co., Ltd., Omron Healthcare Co., Ltd., Fukuda Denshi, and honoraria from Mochida Pharmaceutical Co., Ltd., Takeda Pharmaceutical Co., Ltd., Daiichi Sankyo Co., Ltd., and Sumitomo Dainippon Pharma Co., Ltd. K. The other authors declare no conflicts of interest.
Grant
This study was financially supported, in part, by a grant from the 21st Century Center of Excellence Project run by Japan’s Ministry of Education, Culture, Sports, Science and Technology; a grant from the Foundation for Development of the Community (Tochigi); a grant from Omron Healthcare Co., Ltd, a Grant-in-Aid for Scientific Research (B) (21390247) from The Ministry of Education, Culture, Sports, Science and Technology (MEXT) of Japan, 2009 to 2013; and funds from the MEXT-Supported Program for the Strategic Research Foundation at Private Universities, 2011 to 2015 Cooperative Basic and Clinical Research on Circadian Medicine (S1101022) to K. Kario Funding sponsors had no role in forming the study design or conducting the study; collection, management, analysis, or interpretation of the data; preparation of the article; or decision to submit the article for publication.
Supplementary Files
Supplementary File 1
Supplementary Methods
Appendix S1. Participants and Participating Centers
Table S1.
Subject baseline characteristics vs. J-HOP inclusion status
Table S2.
Prognostic power for cardiovascular events vs. sex
Please find supplementary file(s);
http://dx.doi.org/10.1253/circj.CJ-18-0375
References
- 1.
Maisel AS, Krishnaswamy P, Nowak RM, McCord J, Hollander JE, Duc P, et al. Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure. N Engl J Med 2002; 347: 161–167.
- 2.
Zaphiriou A, Robb S, Murray-Thomas T, Mendez G, Fox K, McDonagh T, et al. The diagnostic accuracy of plasma BNP and NTproBNP in patients referred from primary care with suspected heart failure: Results of the UK natriuretic peptide study. Eur J Heart Fail 2005; 7: 537–541.
- 3.
Mueller T, Gegenhuber A, Poelz W, Haltmayer M. Head-to-head comparison of the diagnostic utility of BNP and NT-proBNP in symptomatic and asymptomatic structural heart disease. Clin Chim Acta 2004; 341: 41–48.
- 4.
Neeland IJ, Drazner MH, Berry JD, Ayers CR, deFilippi C, Seliger SL, et al. Biomarkers of chronic cardiac injury and hemodynamic stress identify a malignant phenotype of left ventricular hypertrophy in the general population. J Am Coll Cardiol 2013; 61: 187–195.
- 5.
Paget V, Legedz L, Gaudebout N, Girerd N, Bricca G, Milon H, et al. N-terminal pro-brain natriuretic peptide: A powerful predictor of mortality in hypertension. Hypertension 2011; 57: 702–709.
- 6.
Nakamura M, Tanaka F, Takahashi T, Makita S, Ishisone T, Onodera M, et al. Sex-specific threshold levels of plasma B-type natriuretic peptide for prediction of cardiovascular event risk in a Japanese population initially free of cardiovascular disease. Am J Cardiol 2011; 108: 1564–1569.
- 7.
de Lemos JA, McGuire DK, Drazner MH. B-type natriuretic peptide in cardiovascular disease. Lancet 2003; 362: 316–322.
- 8.
Martinez-Rumayor A, Richards AM, Burnett JC, Januzzi JL Jr. Biology of the natriuretic peptides. Am J Cardiol 2008; 101: 3–8.
- 9.
Masson S, Latini R, Anand IS, Vago T, Angelici L, Barlera S, et al. Direct comparison of B-type natriuretic peptide (BNP) and amino-terminal proBNP in a large population of patients with chronic and symptomatic heart failure: The Valsartan Heart Failure (Val-HeFT) data. Clin Chem 2006; 52: 1528–1538.
- 10.
Redfield MM, Rodeheffer RJ, Jacobsen SJ, Mahoney DW, Bailey KR, Burnett JC Jr. Plasma brain natriuretic peptide concentration: Impact of age and gender. J Am Coll Cardiol 2002; 40: 976–982.
- 11.
Waku S, Iida N, Ishihara T. Significance of brain natriuretic peptide measurement as a diagnostic indicator of cardiac function. Methods Inf Med 2000; 39: 249–253.
- 12.
Wang TJ, Larson MG, Levy D, Leip EP, Benjamin EJ, Wilson PW, et al. Impact of age and sex on plasma natriuretic peptide levels in healthy adults. Am J Cardiol 2002; 90: 254–258.
- 13.
Christ M, Laule-Kilian K, Hochholzer W, Klima T, Breidthardt T, Perruchoud AP, et al. Gender-specific risk stratification with B-type natriuretic peptide levels in patients with acute dyspnea: Insights from the B-type natriuretic peptide for acute shortness of breath evaluation study. J Am Coll Cardiol 2006; 48: 1808–1812.
- 14.
Hsich EM, Grau-Sepulveda MV, Hernandez AF, Eapen ZJ, Xian Y, Schwamm LH, et al. Relationship between sex, ejection fraction, and B-type natriuretic peptide levels in patients hospitalized with heart failure and associations with inhospital outcomes: Findings from the Get With The Guideline-Heart Failure Registry. Am Heart J 2013; 166: 1063–1071.e1063.
- 15.
Hoshide S, Yano Y, Haimoto H, Yamagiwa K, Uchiba K, Nagasaka S, et al. Morning and evening home blood pressure and risks of incident stroke and coronary artery disease in the Japanese general practice population: The Japan Morning Surge-Home Blood Pressure Study. Hypertension 2016; 68: 54–61.
- 16.
Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure of the European Society of Cardiology (ESC) developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 2016; 37: 2129–2200.
- 17.
Kara K, Lehmann N, Neumann T, Kalsch H, Mohlenkamp S, Dykun I, et al. NT-proBNP is superior to BNP for predicting first cardiovascular events in the general population: The Heinz Nixdorf Recall Study. Int J Cardiol 2015; 183: 155–161.
- 18.
Ballo P, Betti I, Barchielli A, Balzi D, Castelli G, De Luca L, et al. Prognostic role of N-terminal pro-brain natriuretic peptide in asymptomatic hypertensive and diabetic patients in primary care: Impact of age and gender: Results from the PROBE-HF study. Clin Res Cardiol 2016; 105: 421–431.
- 19.
Chen C, Sung KT, Shih SC, Liu CC, Kuo JY, Hou CJ, et al. Age, gender and load-related influences on left ventricular geometric remodeling, systolic mid-wall function, and NT-proBNP in asymptomatic Asian population. PLoS One 2016; 11: e0156467.
- 20.
Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WP. Prognostic implications of echocardiographically determined left ventricular mass in the Framingham Heart Study. N Engl J Med 1990; 322: 1561–1566.
- 21.
Creatsa M, Armeni E, Stamatelopoulos K, Rizos D, Georgiopoulos G, Kazani M, et al. Circulating androgen levels are associated with subclinical atherosclerosis and arterial stiffness in healthy recently menopausal women. Metabolism 2012; 61: 193–201.
- 22.
Ohkuma T, Ninomiya T, Tomiyama H, Kario K, Hoshide S, Kita Y, et al. Brachial-ankle pulse wave velocity and the risk prediction of cardiovascular disease: An individual participant data meta-analysis. Hypertension 2017; 69: 1045–1052.
- 23.
Stein JH, Korcarz CE, Post WS. Use of carotid ultrasound to identify subclinical vascular disease and evaluate cardiovascular disease risk: Summary and discussion of the American Society of Echocardiography consensus statement. Prev Cardiol 2009; 12: 34–38.
- 24.
Glisic M, Rojas LZ, Asllanaj E, Vargas KG, Kavousi M, Ikram MA, et al. Sex steroids, sex hormone-binding globulin and levels of N-terminal pro-brain natriuretic peptide in postmenopausal women. Int J Cardiol 2018; 261: 189–195.
- 25.
Raymond I, Groenning BA, Hildebrandt PR, Nilsson JC, Baumann M, Trawinski J, et al. The influence of age, sex and other variables on the plasma level of N-terminal pro brain natriuretic peptide in a large sample of the general population. Heart 2003; 89: 745–751.
- 26.
Clerico A, Recchia FA, Passino C, Emdin M. Cardiac endocrine function is an essential component of the homeostatic regulation network: Physiological and clinical implications. Am J Physiol Heart Circ Physiol 2006; 290: H17–H29.
- 27.
Hong M, Yan Q, Tao B, Boersma A, Han KK, Vantyghem MC, et al. Estradiol, progesterone and testosterone exposures affect the atrial natriuretic peptide gene expression in vivo in rats. Biol Chem Hoppe-Seyler 1992; 373: 213–218.
