Epicardial Stone ― Unfamiliar Calcified Mass at the Site of Left Ventricular Old Myocardial Infarction ―
Article ID: CJ-18-1102

Details
Article ID: CJ-18-1102
An 80-year-old-man with a history of anteroseptal old myocardial infarction (OMI) had fainted while driving and was referred to Shinshu University Hospital for implantation of implantable cardioverter defibrillator. A sustained ventricular tachycardia was detected.
Computed tomography (CT) incidentally showed a high-density mass measuring 18 mm×11 mm on the anterior left ventricular wall (Figure A–D). Echocardiography indicated no blood flow inside the mass (Figure E), and T2-weighted cardiac magnetic resonance imaging indicated a low-signal area (Figure F). The CT value of the mass, approximately 670 HU, suggested calcification. Coronary angiography also indicated a round area of calcification near the obstructed left anterior descending artery (LAD; Figure G,H). Therefore, the mass was assumed to consist entirely of calcification.
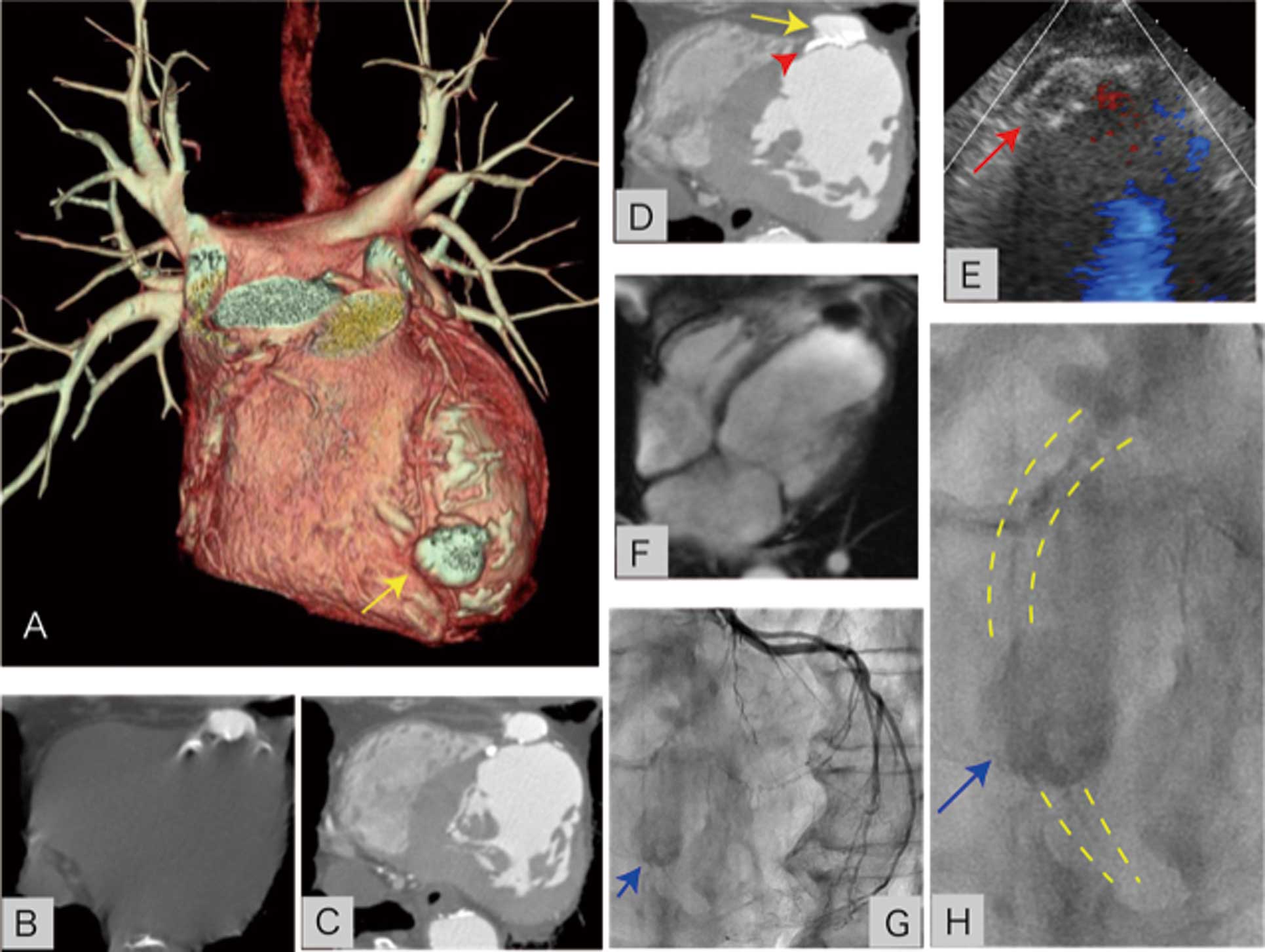
(A–D) Computed tomography. (A) 3-D reconstruction: a round stone (arrow) is visible on the anterior left ventricle wall. (B) Pre-contrast and (C,D) contrast imaging showing (D) the mass (arrow) located on the outside of a calcified aneurysmal area of the anteroseptal wall (arrowhead). (E) Color Doppler echocardiogram: no blood flow was observed inside the mass (arrow). (F) The mass appeared as a homogeneous low-signal area on T2-weighted cardiac magnetic resonance imaging. (G,H) Coronary angiography: the mass (arrow) is visible on the calcified trace of the left anterior descending artery (broken line).
Calcification of the rim of an OMI aneurysm or coronary artery aneurysm has been reported,1,2 but no previous report has described an epicardial stone with no internal blood flow. The origin of the stone remains unclear, but its location near the vestige of LAD suggests the obstruction of a coronary artery aneurysm.
The authors declare no conflicts of interest.