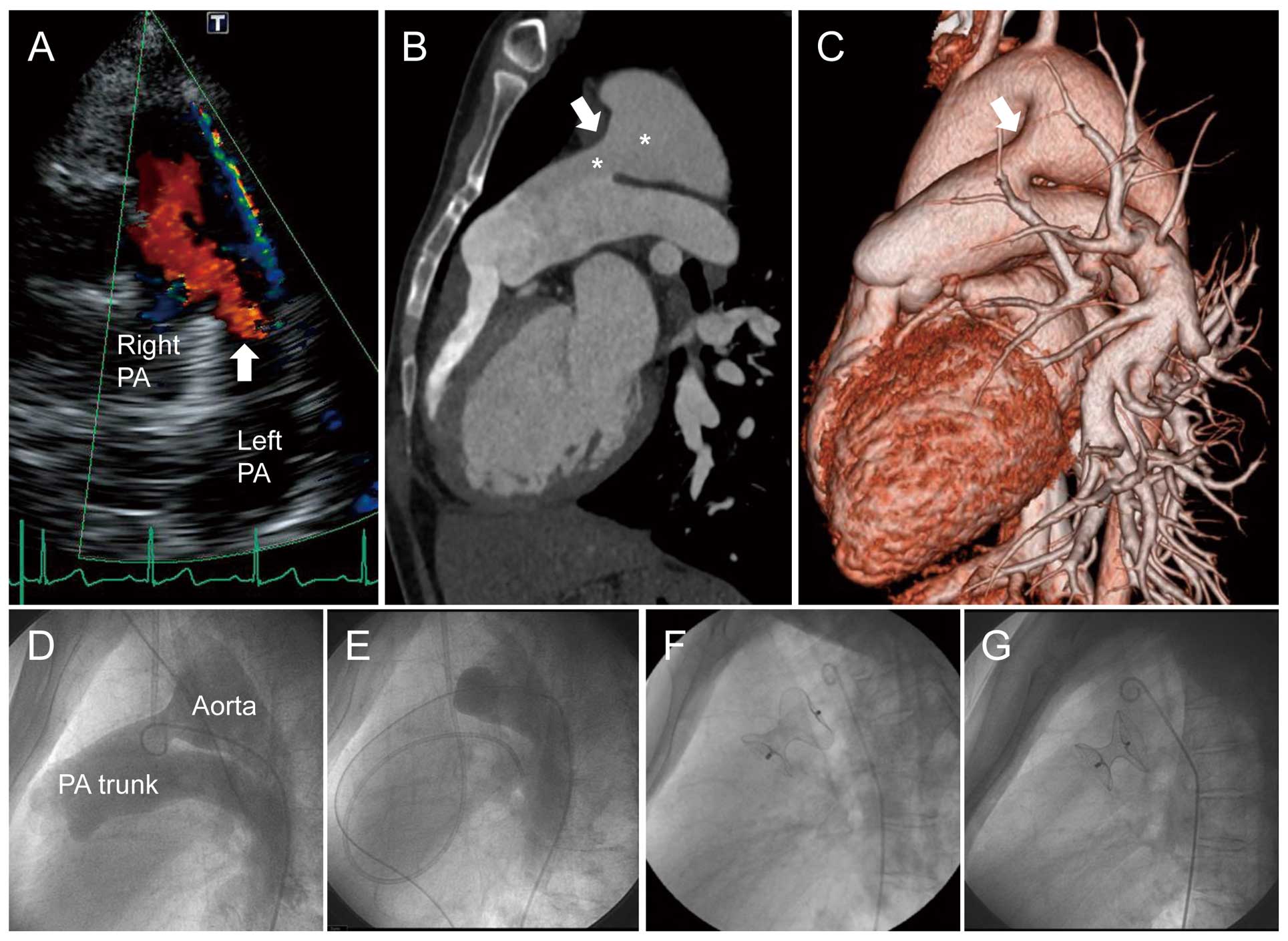
A 34-year-old woman was referred due to a patent ductus arteriosus (PDA) and pulmonary hypertension (PH). She presented with oxygen saturation 92–93% in both the upper and lower limbs. Transthoracic echocardiography indicated significant PDA flow (Figure A). Computed tomography showed a very large elongated-type PDA (Figure B,C). On cardiac catheterization, mean pulmonary arterial pressure (mPAP) was 74 mmHg; pulmonary-to-systemic pressure (Pp/Ps), 0.85; and pulmonary vascular resistance (PVR), 14.0 Wood units; whereas left-to-right shunt (Qp/Qs; 1.75) was still prevalent. Aortography confirmed that the contrast medium drained toward the pulmonary trunk (Figure D; Supplementary Movie 1). We decided to trial PDA occlusion to clarify PH reversibility (Figure E), which markedly decreased mPAP (41 mmHg) and Pp/Ps (0.42) to below 0.5, the cut-off for persistent PH.1
Nitric oxide inhalation further improved mPAP (33 mmHg) during occlusion. Because the PDA was too large for the PDA occluders, we deployed a 24-mm Amplatzer Septal Occluder®, which had a waist diameter 71% larger than the pulmonary end,2
without developing a pressure gradient inside the aorta or the pulmonary artery, after institution ethics committee approval (Figure F). The moderate shunt remaining after the procedure had disappeared almost completely 6 months later (Figure G; Supplementary Movie 2), with improved mPAP (39 mmHg), PVR (11.0 Wood units), and oxygen saturation (97–100%). We introduced 10-mg/day macitentan, an endothelin receptor antagonist. This repair-and-treat strategy consequently improved mPAP and PVR to 29 mmHg and 8.0 Wood units, respectively.
Disclosures
The authors declare no conflicts of interest.
Supplementary Files
Supplementary Movie 1.
Descending aortography, a lateral projection showing that contrast medium drains from the aorta mostly in the direction of the pulmonary trunk.
Supplementary Movie 2.
At 6 months after the successful device closure of the patent ductus arteriosus, descending aortography, a lateral projection showed that the residual shunt had disappeared almost completely.
Please find supplementary file(s);
http://dx.doi.org/10.1253/circj.CJ-19-0144
References
- 1.
Zhang DZ, Zhu XY, Lv B, Cui CS, Han XM, Sheng XT, et al. Trial occlusion to assess the risk of persistent pulmonary arterial hypertension after closure of a large patent ductus arteriosus in adolescents and adults with elevated pulmonary artery pressure. Circ Cardiovasc Interv 2014; 7: 473–481.
- 2.
Garcia-Montes JA, Camacho-Castro A, Sandoval-Jones JP, Buendia-Hernandez A, Calderon-Colmenero J, Patino-Bahena E, et al. Closure of large patent ductus arteriosus using the Amplatzer septal occluder. Cardiol Young 2015; 25: 491–495.
