Abstract
Background:
There is a paucity of data on the management and prognosis of cancer-associated venous thromboembolism (VTE), leading to uncertainty about optimal management strategies.
Methods and Results:
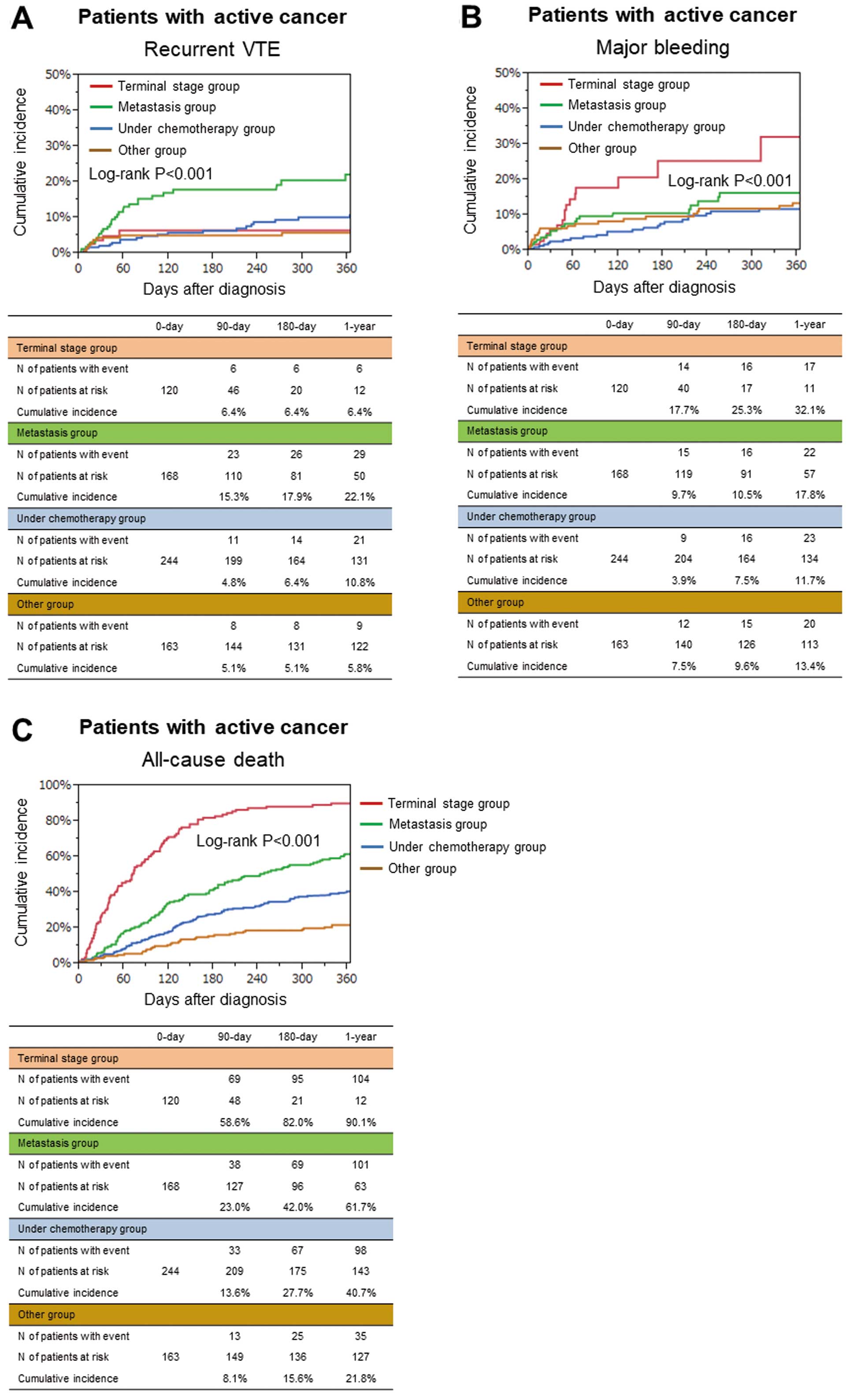
The COMMAND VTE Registry is a multicenter registry enrolling 3,027 consecutive acute symptomatic VTE patients in Japan between 2010 and 2014. We divided the entire cohort into 3 groups: active cancer (n=695, 23%), history of cancer (n=243, 8%), and no history of cancer (n=2089, 69%). The rate of anticoagulation discontinuation was higher in patients with active cancer (43.5%, 27.0%, and 27.0%, respectively, at 1 year, P<0.001). The cumulative 5-year incidences of recurrent VTE, major bleeding, and all-cause death were higher in patients with active cancer (recurrent VTE: 17.7%, 10.2%, and 8.6%, P<0.001; major bleeding: 26.6%, 8.8%, and 9.3%, P<0.001; all-cause death: 73.1%, 28.6%, 14.6%, P<0.001). Among the 4 groups classified according to active cancer status, the cumulative 1-year incidence of recurrent VTE was higher in the metastasis group (terminal stage group: 6.4%, metastasis group: 22.1%, under chemotherapy group: 10.8%, and other group: 5.8%, P<0.001).
Conclusions:
In a current real-world VTE registry, patients with active cancer had higher risk for VTE recurrence, bleeding, and death, with variations according to cancer status, than patients without active cancer. Anticoagulation therapy was frequently discontinued prematurely in patients with active cancer in discordance with current guideline recommendations.
Cancer is a progressive disease with a high mortality rate despite intensive treatment, but many cancer patients are surviving longer because of progress in early diagnosis and treatment.1,2
Thus, complications during the treatment course of cancer are becoming more clinically relevant. Cancer is a strong risk factor for the development of venous thromboembolism (VTE), and patients with cancer are reported to have a 7-fold higher incidence compared with patients without cancer.3
VTE is reported to be the second most frequent cause of death in patients with cancer undergoing chemotherapy.4
Furthermore, VTE in patients with cancer could develop through not only hypercoagulability with cancer, but also treatment-related factors including new molecular target therapeutic agents, which have further increased the risk for development of VTE in the current era.5
A recent study reported that the incidence of VTE in patients with cancer has been increasing over time, but not in patients without cancer.6
Optimal management strategies of VTE patients with cancer have become a major concern that challenges clinicians in daily clinical practice. VTE patients with active cancer are reported to have a markedly higher risk of recurrence as well as bleeding, compared with those without active cancer, creating difficulty in achieving a good risk-benefit balance with anticoagulation therapy.7
Despite several guideline recommendations about treatment strategies including anticoagulation therapy for patients with cancer-associated VTE, there is still a lack of data on these patients, leading to uncertainty about optimal management strategies.8
Data on current real-world management strategies and clinical outcomes in cancer-associated VTE patients are important for understanding the current issues and unmet needs. Therefore, we sought to evaluate the clinical characteristics, management strategies, and outcomes of patients with cancer-associated VTE in the real world using a large Japanese observational database of VTE.
Methods
Study Population
The COMMAND VTE (COntemporary ManageMent AND outcomes in patients with Venous ThromboEmbolism) Registry is a physician-initiated, retrospective, multicenter cohort study enrolling consecutive patients with acute symptomatic VTE objectively confirmed by imaging examinations or autopsy in 29 centers in Japan between January 2010 and August 2014 before the introduction of direct oral anticoagulants (DOAC) for VTE in Japan. The design of the registry has been reported in detail.9,10
The relevant review board or ethics committee in all 29 participating centers (Supplementary Appendix 1) approved the research protocol.
A total of 3,027 consecutive patients with acute symptomatic VTE were enrolled in the registry after screening of 19,634 consecutive patients with suspected VTE for eligibility through chart review by physicians at each institution. In the current study, we divided the entire cohort into 3 groups according to cancer status: active cancer, history of cancer, and no history of cancer (Figure 1).
Definitions of Patients’ Characteristics
Patients with active cancer were defined as those on treatment for cancer such as chemotherapy or radiotherapy, those scheduled to undergo surgery for cancer, those with metastasis to other organs, and/or those with terminal cancer (expected life expectancy ≤6 months) at the time of diagnosis of VTE. Patients with active cancer were further subdivided into 4 groups according to the most advanced cancer status: terminal stage group, metastasis group, under chemotherapy group, and other group. Patients with a history of cancer were defined as those who were previously diagnosed as having cancer, but did not meet the criteria for active cancer.
The initial parenteral anticoagulation therapy was defined as parenteral anticoagulation therapy in the acute phase (heparin or fondaparinux) for ≤10 days after the diagnosis, whereas anticoagulation therapy beyond the acute phase was defined as anticoagulation therapy (warfarin, DOACs, or heparin) that was continued beyond 10 days after the diagnosis. The definitions of other characteristics are described in
Supplementary Appendix 2.
Clinical Follow-up and Endpoints
Collection of follow-up information was mainly through review of hospital charts, and additional follow-up information was collected through contact with patients, relatives, and/or referring physicians by phone and/or mail with questions regarding vital status, recurrent VTE, bleeding, invasive procedures, and status of anticoagulation therapy. In this retrospective cohort study, data collection for follow-up events was performed between July 2016 and March 2017.
The outcome measure was recurrent VTE, major bleeding, and all-cause death. Recurrent VTE was defined as pulmonary embolism (PE) and/or deep vein thrombosis (DVT) with symptoms accompanied by confirmation of new thrombus or exacerbation of the thrombus by objective imaging examinations or autopsy.11
Major bleeding was defined as International Society of Thrombosis and Hemostasis (ISTH) major bleeding, which consisted of a reduction in the hemoglobin level by at least 2 g/dL, a transfusion of ≥2 units of blood, or symptomatic bleeding in a critical area or organ.12
Stroke event was also evaluated, which was defined as ischemic or hemorrhagic stroke either requiring or prolonging hospitalization with symptoms lasting >24 h.
The independent clinical event committee (Supplementary Appendix 3), unaware of the patient characteristics, reviewed all study outcomes, and classified the cause of deaths as PE, cardiac event, cancer, bleeding event, other non-cardiac event, or unknown cause.13
Death was judged to be caused by PE (fatal PE) if it was confirmed by autopsy or if death followed a clinically severe PE, either initially or after recurrent PE events. Death from endstage cancer without a specific cause of death was regarded as cancer origin. Death was judged to be bleeding-related if it followed an intracranial hemorrhage or a bleeding episode leading to hemodynamic deterioration. Death was judged to be from cardiac events if it followed acute myocardial infarction, heart failure, or ventricular arrhythmia. Final classification of the cause of death was made by full consensus of the independent clinical event committee.
Anticoagulation therapy cessation was classified as discontinuation or interruption according to prespecified definitions. Discontinuation of anticoagulation was defined as withdrawal of anticoagulation therapy lasting >14 days for any reason such as bleeding event, drug side effect, physicians’ judgment in the absence of adverse events, and non-adherence of the patient. Interruption of anticoagulation was defined as temporary cessation of anticoagulation therapy with reinstitution within 14 days for any reason including invasive procedure and bleeding events, etc. Scheduled switch from one anticoagulation therapy to another was not regarded as interruption of anticoagulation. Data for the international normalized ratio (INR) during follow-up in patients receiving warfarin were collected from the hospital charts of the centers where the index VTE was diagnosed. Time in therapeutic range (TTR) was calculated by the Rosendaal method,14
according to a therapeutic INR range of 1.5–2.5, which is recommended in the Japanese guidelines,8
as well as a therapeutic INR range of 2.0–3.0, which is recommended in the Western guidelines.15–17
Statistical Analysis
Categorical variables are presented as numbers and percentages. Continuous variables are presented as the mean and standard deviation or the median and interquartile range based on their distributions. Categorical variables were compared with the chi-square test when appropriate; otherwise, Fisher’s exact test was used. Continuous variables were compared using one-way analysis of variance or Kruskal-Wallis test based on their distributions. We used the Kaplan-Meier method to estimate the cumulative incidence and assessed the differences with the log-rank test. To adjust for clinically relevant confounders, we used the multivariable Cox proportional hazard to estimate the hazard ratio (HR) and 95% confidence interval (CI) for the risk of patients with active cancer and patients with a history of cancer relative to patients with no history of cancer for the clinical outcomes. Based on the previous reports15–17
and consideration of clinical relevance, we selected 8 risk-adjusting variables for recurrent VTE, 9 risk-adjusting variables for major bleeding, and 16 risk-adjusting variables for all-cause death (Table 1). Furthermore, we compared the clinical outcomes among the 4 groups classified according to active cancer status. All statistical analyses were conducted using JMP version 10.0.2 (SAS Institute Inc., Cary, NC, USA). All reported P-values are 2-tailed, and P<0.05 was considered statistically significant.
Table 1.
Patients’ Characteristics
| |
Active cancer
(n=695) |
History of cancer
(n=243) |
No history of cancer
(n=2,089) |
P value |
| Baseline characteristics |
| Age (years)*,†,‡ |
66.5±12.2 |
72.2±11.4 |
66.8±16.5 |
<0.001 |
| Women*,†,‡ |
414 (60%) |
133 (55%) |
1,311 (63%) |
0.03 |
| Body weight (kg) |
55.3±12.3 |
55.3±12.0 |
59.1±14.3 |
<0.001 |
| Body mass index (kg/m2) |
22.1±4.0 |
22.5±3.8 |
23.7±4.6 |
<0.001 |
| ≥30 kg/m2* |
26 (3.7%) |
8 (3.3%) |
135 (6.5%) |
0.007 |
| Comorbidities |
| Hypertension‡ |
202 (29%) |
101 (42%) |
858 (41%) |
<0.001 |
| Diabetes mellitus‡ |
88 (13%) |
38 (16%) |
260 (12%) |
0.37 |
| Dyslipidemia |
97 (14%) |
51 (21%) |
460 (22%) |
<0.001 |
| Chronic kidney disease†,‡ |
117 (17%) |
58 (24%) |
397 (19%) |
0.053 |
| Dialysis |
5 (0.7%) |
2 (0.8%) |
14 (0.7%) |
0.96 |
| History of chronic lung disease |
56 (8.1%) |
33 (13.6%) |
182 (8.7%) |
0.03 |
| History of heart failure |
10 (1.4%) |
13 (5.4%) |
78 (3.7%) |
0.003 |
| History of myocardial infarction |
6 (0.9%) |
6 (2.5%) |
41 (2.0%) |
0.11 |
| History of stroke‡ |
36 (5.2%) |
33 (13.6%) |
201 (9.6%) |
<0.001 |
| Atrial fibrillation |
24 (3.5%) |
15 (6.2%) |
90 (4.3%) |
0.19 |
| Liver cirrhosis†,‡ |
8 (1.2%) |
5 (2.1%) |
13 (0.6%) |
0.046 |
| Connective tissue disease‡ |
21 (3.0%) |
18 (7.4%) |
205 (9.8%) |
<0.001 |
| Varicose vein*,‡ |
13 (1.9%) |
14 (5.8%) |
112 (5.4%) |
<0.001 |
| History of VTE*,‡ |
40 (5.8%) |
18 (7.4%) |
120 (5.7%) |
0.57 |
| History of major bleeding†,‡ |
72 (10.4%) |
20 (8.2%) |
139 (6.7%) |
0.006 |
| Transient risk factors for VTE*,†,‡ |
196 (28%) |
86 (35%) |
804 (38%) |
<0.001 |
| Presentation |
| PE with or without DVT*,†,‡ |
393 (57%) |
130 (54%) |
1,192 (57%) |
0.57 |
| Hypoxemia |
161/393 (41%) |
61/130 (47%) |
628/1,192 (53%) |
<0.001 |
| Shock |
25/393 (6.4%) |
15/130 (11.5%) |
139/1,192 (11.7%) |
0.01 |
| Cardiac arrest/collapse |
7/393 (1.8%) |
8/130 (6.2%) |
65/1,192 (5.5%) |
0.008 |
| DVT only*,†,‡ |
302 (43%) |
113 (46%) |
897 (43%) |
0.57 |
| Proximal DVT*,†,‡ |
217/302 (72%) |
79/113 (70%) |
625/897 (70%) |
0.77 |
| Out-of-hospital onset |
458 (66%) |
185 (76%) |
1,665 (80%) |
<0.001 |
| Laboratory tests at diagnosis |
| Anemia†,‡ |
529 (76%) |
139 (57%) |
959 (46%) |
<0.001 |
| Thrombocytopenia (platelet count <100×109/L)†,‡ |
55 (7.9%) |
20 (8.2%) |
92 (4.4%) |
<0.001 |
| D-dimer (μg/mL) (n=2,852) |
13.3 (6.2–25.5) |
9.9 (4.5–19.5) |
9.7 (5.0–19.7) |
<0.001 |
| Thrombophilia*,‡ |
19 (2.7%) |
11 (4.5%) |
117 (5.6%) |
0.009 |
| Treatment in the acute phase |
| Initial parenteral anticoagulation therapy |
577 (83%) |
207 (85%) |
1,750 (84%) |
0.73 |
| Thrombolysis |
53 (7.6%) |
28 (11.5%) |
349 (16.7%) |
<0.001 |
| Inferior vena cava filter use |
191 (27%) |
51 (21%) |
478 (23%) |
0.03 |
| Ventilator support |
10 (1.4%) |
11 (4.5%) |
71 (3.4%) |
0.01 |
| Percutaneous cardiopulmonary support |
1 (0.1%) |
4 (1.7%) |
34 (1.6%) |
0.01 |
| Concomitant medications at discharge |
| Corticosteroids |
109 (16%) |
25 (10%) |
213 (10%) |
<0.001 |
| Non-steroidal anti-inflammatory drugs |
111 (16.0%) |
17 (7.0%) |
169 (8.1%) |
<0.001 |
| Proton pump inhibitors/H2-blockers |
313 (45%) |
104 (43%) |
919 (44%) |
0.81 |
| Statins |
54 (7.8%) |
34 (14.0%) |
349 (16.7%) |
<0.001 |
| Antiplatelet agents |
43 (6.2%) |
29 (11.9%) |
235 (11.3%) |
<0.001 |
| Anticoagulation therapy beyond the acute phase |
614 (88%) |
221 (91%) |
1,968 (94%) |
<0.001 |
| Warfarin |
576 (83%) |
211 (87%) |
1,889 (90%) |
|
| Direct oral anticoagulant |
20 (2.9%) |
6 (2.5%) |
52 (2.5%) |
<0.001 |
| Heparin |
18 (2.6%) |
4 (1.7%) |
27 (1.3%) |
|
| TTR for INR 1.5–2.5 (%) (n=2,509) |
60.7 (36.8–81.3) |
67.2 (43.8–90.1) |
75.8 (50.5–93.8) |
<0.001 |
| TTR for INR 2.0–3.0 (%) (n=2,509) |
30.9 (11.6–50.6) |
31.9 (8.1–56.7) |
30.6 (7.4–57.7) |
0.94 |
Maximum INR value during warfarin administration
(n=2,620) |
3.4±1.8 |
3.0±1.4 |
2.7±1.1 |
<0.001 |
| Discontinuation of anticoagulation during follow-up |
266/614 |
92/221 |
731/1968 |
0.02 |
| Reason for discontinuation |
| Physician’s judgment |
81/266 (30%) |
54/92 (59%) |
513/731 (70%) |
<0.001 |
| Bleeding event |
86/266 (32%) |
21/92 (23%) |
94/731 (13%) |
|
| Other |
99/266 (37%) |
17/92 (18%) |
124/731 (17%) |
|
| Interruption of anticoagulation during follow-up period |
107/614 (17%) |
25/221 (11%) |
215/1,968 (11%) |
0.001 |
Categorical variables are presented as numbers and percentages, and continuous variables are presented as the mean and standard deviation or the median and interquartile range based on their distributions. Categorical variables were compared using the chi-squared test when appropriate; otherwise, Fisher’s exact test was used. Continuous variables were compared using one-way analysis of variance or Kruskal-Wallis test based on their distributions. Chronic kidney disease was diagnosed if there was persistent proteinuria or if estimated glomerular filtration rate (eGFR) was <60 mL/min/1.73 m2 for more than 3 months. The eGFR was calculated based on the equation reported by Japan Association of Chronic Kidney Disease Initiative [male: 194*Scr−1.094*age−0.287, female: 194*Scr−1.094*age−0.287*0.739]. Thrombophilia included protein C deficiency, protein S deficiency, antithrombin deficiency, and antiphospholipid syndrome. *Risk-adjusting variables for the multivariable Cox regression model to estimate the risk for recurrent VTE. †Risk-adjusting variables for the multivariable Cox regression model to estimate the risk for major bleeding. ‡Risk-adjusting variables for the multivariable Cox regression model to estimate the risk for all-cause death. DVT, deep vein thrombosis; INR, international normalized ratio; PE, pulmonary embolism; TTR, time in therapeutic range; VTE, venous thromboembolism.
Results
Patients’ Characteristics
The groups with active cancer, a history of cancer, and no history of cancer comprised 695 (23%), 243 (8%), and 2,089 (69%) patients, respectively. Baseline characteristics were different across the 3 groups in several aspects (Table 1). Patients with active cancer were younger, and more often had a history of major bleeding and anemia. As for cancer site in patients with active cancer, lung cancer was the most common (16.4%), followed by colorectal cancer (12.7%), hematological malignancy (8.9%), uterine (8.8%), and ovarian cancer (8.5%) (Table 2). Among the patients with active cancer, more than half were under chemotherapy, and approximately one-third had distant metastasis.
Table 2.
Cancer Characteristics
| |
Overall
(n=938) |
Active cancer
(n=695) |
History of cancer
(n=243) |
| Cancer site |
| Lung |
127 (13.5) |
114 (16.4) |
13 (5.4) |
| Colon |
127 (13.5) |
88 (12.7) |
39 (16.1) |
| Stomach |
90 (9.6) |
51 (7.3) |
39 (16.1) |
| Uterus |
78 (8.3) |
61 (8.8) |
17 (7.0) |
| Blood |
75 (8.0) |
62 (8.9) |
13 (5.4) |
| Ovary |
64 (6.8) |
59 (8.5) |
5 (2.1) |
| Prostate |
57 (6.1) |
36 (5.2) |
21 (8.6) |
| Breast |
53 (5.7) |
26 (3.7) |
27 (11.1) |
| Pancreas |
44 (4.7) |
41 (5.9) |
3 (1.2) |
| Bladder |
25 (2.7) |
14 (2.0) |
11 (4.5) |
| Brain |
23 (2.5) |
18 (2.6) |
5 (2.1) |
| Kidney/ureter |
16 (1.7) |
10 (1.4) |
6 (2.5) |
| Esophagus |
15 (1.6) |
10 (1.4) |
5 (2.1) |
| Gall bladder/bile duct |
14 (1.5) |
13 (1.9) |
1 (0.4) |
| Skin |
13 (1.4) |
8 (1.2) |
5 (2.1) |
| Thyroid gland |
12 (1.3) |
4 (0.6) |
8 (3.3) |
| Liver |
11 (1.2) |
11 (1.6) |
0 (0.0) |
| Oral cavity/pharynx |
9 (1.0) |
7 (1.0) |
2 (0.8) |
| Small intestine |
3 (0.3) |
2 (0.3) |
1 (0.4) |
| Others |
24 (2.6) |
20 (2.9) |
4 (1.7) |
| Multiple |
58 (6.2) |
40 (5.8) |
18 (7.4) |
| Cancer status |
| Scheduled to be operated |
|
72 (10) |
|
| Under chemotherapy |
– |
381 (55) |
– |
| Distant metastasis |
– |
223 (32) |
– |
| Terminal stage |
– |
120 (17) |
– |
Variables are presented as numbers and proportions (%).
The prevalence of initial parenteral anticoagulation therapy was not significantly different among the 3 groups (patients with active cancer: 83%, patients with history of cancer: 85%, and patients with no history of cancer: 84%, P=0.73) (Table 1). Thrombolysis was implemented least frequently in patients with active cancer (7.6%, 11.5%, and 16.7%, respectively; P<0.001), and inferior vena cava filters were placed most frequently in patients with active cancer (27%, 21%, and 23%, P=0.03).
Anticoagulation therapy beyond the acute phase was implemented least frequently in patients with active cancer (88%, 91%, and 94%, P<0.001). Most of the anticoagulation therapy beyond the acute phase was warfarin in all groups, and the prevalence of heparin usage was low even in patients with active cancer (2.6%). Median TTR for warfarin users according to Japanese guideline recommendations was lowest in patients with active cancer (Table 1). The rate of anticoagulation discontinuation was highest in patients with active cancer (43.5% vs. 27.0% vs. 27.0% at 1 year, P<0.001) (Figure 2). Discontinuation because of a bleeding event was most frequent in patients with active cancer, and interruption of anticoagulation during the entire follow-up period was also most frequent in patients with active cancer (Table 1).
Clinical Outcomes
The median follow-up period was 1,218 (IQR: 847–1,764) days for surviving patients (95.1% follow-up rate at 1 year). The cumulative 5-year incidences of recurrent VTE and major bleeding were much higher in patients with active cancer (recurrent VTE: 17.7%, 10.2%, and 8.6%, P<0.001; major bleeding: 26.6%, 8.8%, and 9.3%, P<0.001, respectively) (Figure 3A,B). After adjusting for confounders, the excess risks of patients with active cancer relative to patients with no history of cancer for recurrent VTE and major bleeding remained highly significant (recurrent VTE: adjusted HR 2.94, 95% CI 2.20–3.92, P<0.001; major bleeding: adjusted HR 2.48, 95% CI 1.90–3.23, P<0.001, respectively), whereas the risks of patients with history of cancer relative to patients with no history of cancer for recurrent VTE and major bleeding were not significant (adjusted HR 1.47, 95% CI 0.87–2.36, P=0.15 and adjusted HR 1.01, 95% CI 0.60–1.59, P=0.97, respectively) (Table 3).
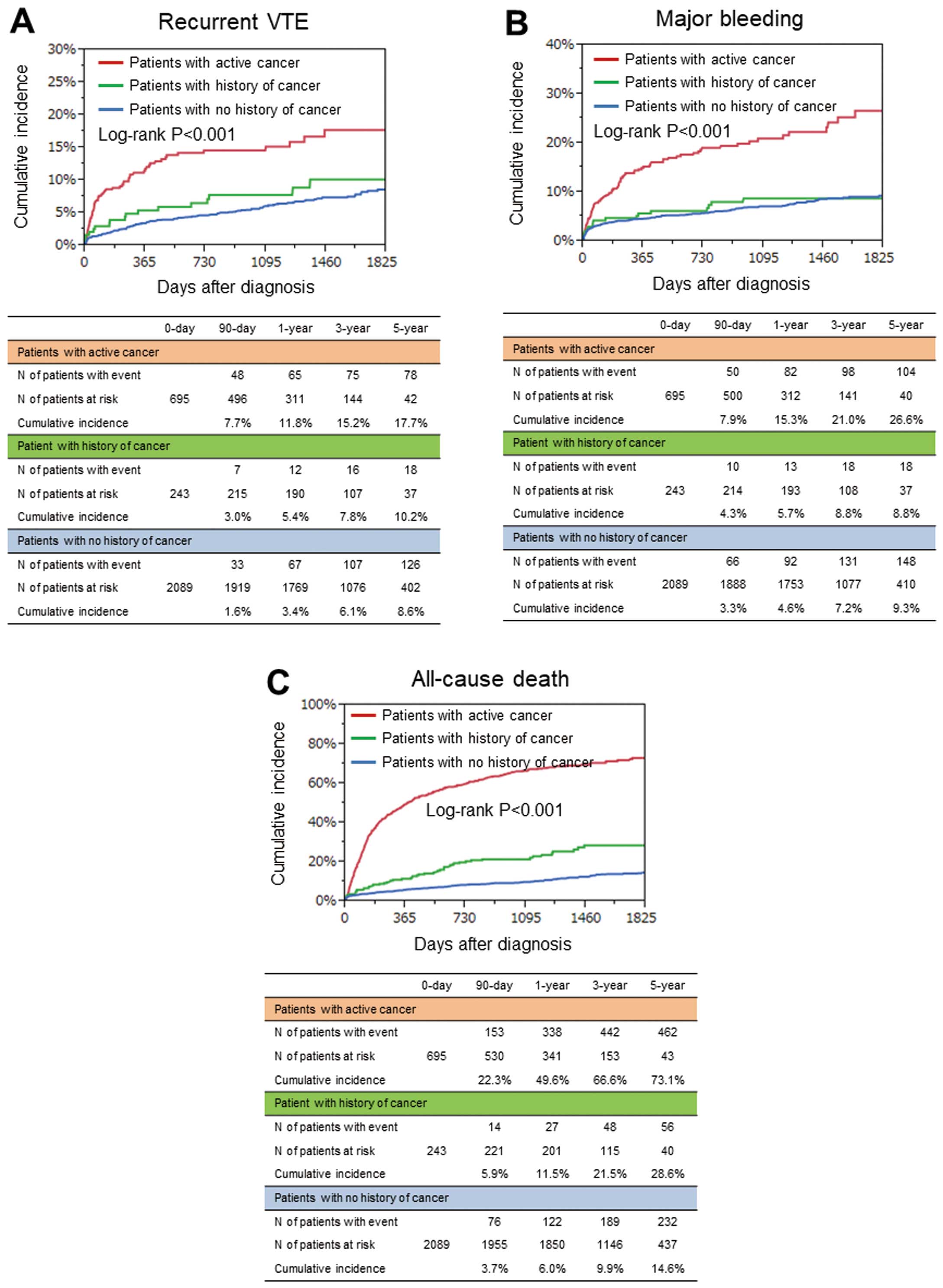
Table 3.
Crude and Adjusted Clinical Outcomes
| |
No history
of cancer
(Reference)
(n=2,089) |
History of cancer
(n=243) |
Active cancer
(n=695) |
N of
patients
with
event* |
N of
patients
with
event* |
Crude HR
(95% CI) |
P value |
Adjusted
HR
(95% CI) |
P value |
N of
patients
with
event* |
Crude HR
(95% CI) |
P value |
Adjusted
HR
(95% CI) |
P value |
Recurrent
VTE |
130
(8.6%) |
18
(10.2%) |
1.31
(0.77–
2.08) |
0.30 |
1.47
(0.87–
2.36) |
0.15 |
78
(17.7%) |
2.81
(2.11–
3.73) |
<0.001 |
2.94
(2.20–
3.92) |
<0.001 |
Major
bleeding |
151
(9.3%) |
19
(8.8%) |
1.16
(0.70–
1.83) |
0.54 |
1.01
(0.60–
1.59) |
0.97 |
105
(26.6%) |
3.08
(2.39–
3.96) |
<0.001 |
2.48
(1.90–
3.23) |
<0.001 |
All-cause
death |
241
(14.6%) |
59
(26.6%) |
2.31
(1.72–
3.04) |
<0.001 |
1.94
(1.44–
2.57) |
<0.001 |
464
(73.1%) |
9.21
(7.87–
10.79) |
<0.001 |
8.55
(7.22–
10.15) |
<0.001 |
Death from
cancer |
18
(1.3%) |
12
(8.2%) |
6.24
(2.93–
12.84) |
<0.001 |
– |
– |
379
(63.9%) |
100.21
(64.37–
166.96) |
<0.001 |
– |
– |
| Fatal PE |
56
(2.7%) |
9
(3.8%) |
1.40
(0.65–
2.69) |
0.37 |
– |
– |
20
(3.2%) |
1.12
(0.66–
1.84) |
0.66 |
– |
– |
Fatal
bleeding |
15
(1.3%) |
2
(1.1%) |
1.29
(0.20–
4.56) |
0.75 |
– |
– |
18
(6.1%) |
6.17
(3.07–
12.57) |
<0.001 |
– |
– |
*Cumulative 5-year incidence. N of patients with event was counted throughout the entire follow-up period. Cumulative 5-year incidence was estimated using the Kaplan-Meier method. Crude and adjusted HRs and 95% CIs were estimated using the Cox proportional hazard models. HRs for the active cancer group and history of cancer group were estimated relative to the no history of cancer group. Recurrent VTE, major bleeding and all-cause death were adjusted by the respective risk-adjusting covariates listed in Table 1. CI, confidence interval; HR, hazard ratio; PE, pulmonary embolism; VTE, venous thromboembolism.
The cumulative 5-year incidence of all-cause death was markedly higher in patients with active cancer (73.1%, 28.6%, and 14.6%, P<0.001) (Figure 3C). After adjusting for confounders, the excess risks of patients with active cancer and patients with history of cancer relative to patients with no history of cancer for all-cause death were significant (patients with active cancer: adjusted HR 8.55, 95% CI 7.22–10.15, P<0.001; patients with history of cancer: adjusted HR 1.94, 95% CI 1.44–2.57, P<0.001, respectively) (Table 3). The cause of death was cancer in the majority of patients with active cancer (81.7%) (Table 4).
Table 4.
Causes of Death During the Entire Follow-up Period
| |
Active cancer
(n=464) |
History of cancer
(n=59) |
No history of cancer
(n=241) |
| Cancer |
379 (81.7) |
12 (20.3) |
18 (7.5) |
| Fatal pulmonary embolism |
20 (4.3) |
9 (15.3) |
56 (23.2) |
| Bleeding events |
18 (3.9) |
2 (3.4) |
15 (6.2) |
| Cardiac events |
4 (0.9) |
6 (10.2) |
27 (11.2) |
| Other non-cardiac events |
24 (5.2) |
21 (35.6) |
92 (38.2) |
| Ischemic stroke |
1 (0.2) |
0 (0.0) |
2 (0.8) |
| Unknown |
19 (4.1) |
9 (15.3) |
33 (13.7) |
Variables are presented as numbers and proportions (%). Death was judged as cardiac if it followed acute myocardial infarction, heart failure, or ventricular arrhythmia.
The cumulative 5-year incidence of stroke was higher in patients with active cancer (9.3%, 4.5%, and 4.5%, P=0.002) (Supplementary Table). The proportion of hemorrhagic stroke was numerically higher than that of ischemic stroke in all groups. The cumulative 5-year incidence of ischemic stroke was also higher in patients with active cancer (4.4%, 1.0%, and 1.8%, P=0.003), whereas the cumulative 5-year incidence of hemorrhagic stroke was not significantly different among the groups (5.2%, 3.6%, and 2.7%, P=0.11). There was 1 patient with active cancer who died of an ischemic stroke (Table 4).
Clinical Outcomes According to Active Cancer Status
The cumulative 1-year incidence of recurrent VTE was much higher in the metastasis group than in the other cancer status groups (terminal stage group: 6.4%, metastasis group: 22.1%, under chemotherapy group: 10.8%, and other group: 5.8%, P<0.001), whereas the cumulative 1-year incidences of major bleeding and all-cause death were much higher in the terminal stage group than in the other cancer status groups (major bleeding: 32.1%, 17.8%, 11.7%, and 13.4%, P<0.001, and all-cause death: 90.1%, 61.7%, 40.7%, and 21.8%, P<0.001) (Figure 4). The rate of anticoagulation discontinuation was highest in the terminal stage group (57.7%, 43.2%, 38.5%, and 45.7%, at 1-year, P=0.004) (Supplementary Figure).
Discussion
The major findings of the current study were: (1) VTE patients with active cancer had a dismal prognosis, with higher rates of recurrent VTE, major bleeding and all-cause death than those without active cancer, while patients with a history of cancer had comparable risks for recurrent VTE and major bleeding as patients with no history of cancer; (2) VTE patient with active cancer had frequent discontinuation of anticoagulation therapy during the follow-up period, and the quality of warfarin control was poor; and (3) the risks for clinical events varied widely according to cancer status in VTE patient with active cancer.
A previous study reported that VTE patients with cancer had higher risks of recurrence and bleeding than those without cancer.3
Consistent with that report, the current study showed higher risks of VTE recurrence and bleeding in patients with active cancer than in those without active cancer. However, there are few reports evaluating clinical outcomes in patients not in the active condition of cancer (i.e., patients with history of cancer).18,19
The present study demonstrated comparable risks of VTE recurrence and bleeding in patients with a history of cancer relative to those with no history of cancer, suggesting that the adverse effects of cancer for VTE recurrence and bleeding are significant if cancer is non-active.
Because active cancer is a strong risk factor for recurrence of VTE, VTE patients with active cancer are considered candidates for indefinite anticoagulation therapy. Actually, several current guidelines recommend prolonged anticoagulation therapy as long as the disease is considered active.8,15–17
Furthermore, a previous study reported the importance of cancer-associated hypercoagulability as a possible stroke etiology in patients with cancer.20
Consistent with that report, the current study showed that VTE patients with active cancer had a higher risk for subsequent ischemic stroke. In addition, it should be noted that the proportion of hemorrhagic stroke was numerically greater than that of ischemic stroke. The current study also showed that discontinuation of anticoagulation therapy during follow-up was most frequent in patients with active cancer. This might be partly because patients with active cancer generally have a higher risk for bleeding and they often have difficulty in continuing anticoagulation therapy, because of cancer progression. Patients with active cancer frequently receive various drugs that interact with warfarin, including chemotherapy, and often have unstable dietary intake, leading to difficulty in maintaining good control of warfarin.21,22
In fact, the current study showed poor-quality warfarin control in patients with active cancer. In this context, DOACs have been reported to have comparable efficacy and safety compared with low-molecular-weight heparin in patients with cancer-associated VTE.23,24
Considering the lower likelihood of food and drug interactions of DOACs, they could be good alternative to warfarin for cancer-associated VTE.
The risks for recurrence and bleeding can be higher in more advanced cancer.25–27
Consistent with previous reports, the current study also showed that the risks for recurrence and bleeding, as well as death, tended to be higher in parallel with the progression of cancer status. Furthermore, patients in the terminal stage of cancer had the highest risk for major bleeding with a dismal mortality risk. Actually, the current study also showed that anticoagulation therapy was discontinued most frequently in patients in the terminal stage of cancer, partly because of a bleeding event. We should be cautious about considering the need and duration of anticoagulation therapy for patients in the terminal stage of cancer. A recent study reported that approximately one-third of patients with advanced cancer admitted to palliative care units had a DVT, although thromboprophylaxis for these patients seemed to be of little benefit.28
For the decision-making on anticoagulation therapy in cancer patients in the terminal stage, it might be important to consider not only the prognosis, but also quality of life based on the individual patient. In addition to the progression of cancer status, cancer sites could also have some influence on the recurrence and bleeding risk, which should be take into consideration. Further studies are warranted for optimal treatment strategies according to cancer sites.
Study Limitations
First, this was an observational cohort study with the limitations inherent to the study design. The decisions regarding management strategies were left to the discretion of the attending physicians. Second, demographics, practice patterns as well as clinical outcomes in patients with VTE in Japan may be different from those outside Japan. Third, low-molecular-weight heparin for VTE was not covered by Japanese national insurance. Therefore, warfarin was mostly used as the anticoagulation therapy beyond the acute phase for patients with active cancer, although low-molecular-weight heparin is recommended over warfarin in the Western guideline. Fourth, cancer treatments, including platinum-based chemotherapy and molecular targeted therapy, were not evaluated. Fifth, the time period of cancer relapse-free survival in the patients with history of cancer was also not evaluated. Finally, cancer status was not evaluated after the index VTE event, and we could not assess the influence of the course of cancer during follow-up on clinical outcomes.
Conclusions
In a current real-world Japanese VTE registry, patients with active cancer had higher risk for VTE recurrence, bleeding, and death than patients without active cancer. Anticoagulation therapy was frequently discontinued prematurely in VTE patients with active cancer in discordance with current guideline recommendations.
Acknowledgments
We appreciate the support and collaboration of the co-investigators participating in the COMMAND VTE Registry. We are indebted to the independent clinical research organization (Research Institute for Production Development, Kyoto, Japan) for technical support.
Conflicts of Interest
Dr. Yamashita received lecture fees from Daiichi-Sankyo, Bristol-Myers Squibb, and Bayer Healthcare. Dr. Morimoto received lecture fees from Mitsubishi Tanabe Pharma and Pfizer Japan, and consultant fees from Asahi Kasei, Bristol-Myers Squibb, and Boston Scientific. Dr. Akao received lecture fees from Pfizer, Bristol-Myers Squibb, Boehringer Ingelheim, Bayer Healthcare, and Daiichi-Sankyo. Dr. Kimura received a research grant from Daiichi-Sankyo. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Funding
The COMMAND VTE Registry is supported by the independent clinical research organization (Research Institute for Production Development, Kyoto, Japan) and research funding from Mitsubishi Tanabe Pharma Corporation. The research funder had no role in the design and conduct of the study, collection, management, analysis, and interpretation of the data, and preparation, review, or approval of the manuscript.
Supplementary Files
Please find supplementary file(s);
http://dx.doi.org/10.1253/circj.CJ-19-0515
References
- 1.
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin 2019; 69: 7–34.
- 2.
Ito Y, Miyashiro I, Ito H, Hosono S, Chihara D, Nakata-Yamada K, et al. Long-term survival and conditional survival of cancer patients in Japan using population-based cancer registry data. Cancer Sci 2014; 105: 1480–1486.
- 3.
Blom JW, Doggen CJ, Osanto S, Rosendaal FR. Malignancies, prothrombotic mutations, and the risk of venous thrombosis. JAMA 2005; 293: 715–722.
- 4.
Khorana AA. Venous thromboembolism and prognosis in cancer. Thromb Res 2010; 125: 490–493.
- 5.
Mukai M, Oka T. Mechanism and management of cancer-associated thrombosis. J Cardiol 2018; 72: 89–93.
- 6.
Walker AJ, Card TR, West J, Crooks C, Grainge MJ. Incidence of venous thromboembolism in patients with cancer: A cohort study using linked United Kingdom databases. Eur J Cancer 2013; 49: 1404–1413.
- 7.
Prandoni P, Lensing AW, Piccioli A, Bernardi E, Simioni P, Girolami B, et al. Recurrent venous thromboembolism and bleeding complications during anticoagulant treatment in patients with cancer and venous thrombosis. Blood 2002; 100: 3484–3488.
- 8.
JCS Joint Working Group. Guidelines for the diagnosis, treatment and prevention of pulmonary thromboembolism and deep vein thrombosis (JCS 2009): Digest version. Circ J 2011; 75: 1258–1281.
- 9.
Yamashita Y, Morimoto T, Amano H, Takase T, Hiramori S, Kim K, et al. Anticoagulation therapy for venous thromboembolism in the real world: From the COMMAND VTE Registry. Circ J 2018; 82: 1262–1270.
- 10.
Yamashita Y, Morimoto T, Amano H, Takase T, Hiramori S, Kim K, et al. Influence of baseline platelet count on outcomes in patients with venous thromboembolism (from the COMMAND VTE Registry). Am J Cardiol 2018; 122: 2131–2141.
- 11.
Büller HR, Décousus H, Grosso MA, Mercuri M, Middeldorp S, Prins MH, et al. Edoxaban versus warfarin for the treatment of symptomatic venous thromboembolism. N Engl J Med 2013; 369: 1406–1415.
- 12.
Schulman S, Kearon C; Subcommittee on Control of Anticoagulation of the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J Thromb Haemost 2005; 3: 692–694.
- 13.
Faller N, Limacher A, Mean M, Righini M, Aschwanden M, Beer JH, et al. Predictors and causes of long-term mortality in elderly patients with acute venous thromboembolism: A prospective cohort study. Am J Med 2017; 130: 198–206.
- 14.
Rosendaal FR, Cannegieter SC, van der Meer FJ, Briet E. A method to determine the optimal intensity of oral anticoagulant therapy. Thromb Haemost 1993; 69: 236–239.
- 15.
Konstantinides SV, Torbicki A, Agnelli G, Danchin N, Fitzmaurice D, Galiè N, et al. 2014 ESC guidelines on the diagnosis and management of acute pulmonary embolism. Eur Heart J 2014; 35: 3033–3069, 3069a–3069k.
- 16.
Kearon C, Akl EA, Ornelas J, Blaivas A, Jimenez D, Bounameaux H, et al. Antithrombotic therapy for VTE disease: CHEST Guideline and Expert Panel Report. Chest 2016; 149: 315–352.
- 17.
Jaff MR, McMurtry MS, Archer SL, Cushman M, Goldenberg N, Goldhaber SZ, et al. Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: A Scientific Statement from the American Heart Association. Circulation 2011; 123: 1788–1830.
- 18.
Raskob GE, van Es N, Segers A, Angchaisuksiri P, Oh D, Boda Z, et al. Edoxaban for venous thromboembolism in patients with cancer: Results from a non-inferiority subgroup analysis of the Hokusai-VTE randomised, double-blind, double-dummy trial. Lancet Haematol 2016; 3: e379–e387.
- 19.
Agnelli G, Buller HR, Cohen A, Gallus AS, Lee TC, Pak R, et al. Oral apixaban for the treatment of venous thromboembolism in cancer patients: Results from the AMPLIFY trial. J Thromb Haemost 2015; 13: 2187–2191.
- 20.
Schwarzbach CJ, Schaefer A, Ebert A, Held V, Bolognese M, Kablau M, et al. Stroke and cancer: The importance of cancer-associated hypercoagulation as a possible stroke etiology. Stroke 2012; 43: 3029–3034.
- 21.
Kearon C, Akl EA, Comerota AJ, Prandoni P, Bounameaux H, Goldhaber SZ, et al. Antithrombotic therapy for VTE disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012; 141: e419S–e496S.
- 22.
Elalamy I, Mahé I, Ageno W, Meyer G. Long-term treatment of cancer-associated thrombosis: The choice of the optimal anticoagulant. J Thromb Haemost 2017; 15: 848–857.
- 23.
Raskob GE, van Es N, Verhamme P, Carrier M, Di Nisio M, Garcia D, et al. Edoxaban for the treatment of cancer-associated venous thromboembolism. N Engl J Med 2018; 378: 615–624.
- 24.
Young AM, Marshall A, Thirlwall J, Chapman O, Lokare A, Hill C, et al. Comparison of an oral factor Xa inhibitor with low molecular weight heparin in patients with cancer with venous thromboembolism: Results of a randomized trial (SELECT-D). J Clin Oncol 2018; 36: 2017–2023.
- 25.
Prandoni P, Trujillo-Santos J, Surico T, Dalla Valle F, Piccioli A, Monreal M, et al. Recurrent thromboembolism and major bleeding during oral anticoagulant therapy in patients with solid cancer: Findings from the RIETE registry. Haematologica 2008; 93: 1432–1434.
- 26.
Trujillo-Santos J, Nieto JA, Tiberio G, Piccioli A, Di Micco P, Prandoni P, et al. Predicting recurrences or major bleeding in cancer patients with venous thromboembolism: Findings from the RIETE Registry. Thromb Haemost 2008; 100: 435–439.
- 27.
Chee CE, Ashrani AA, Marks RS, Petterson TM, Bailey KR, Melton LJ, et al. Predictors of venous thromboembolism recurrence and bleeding among active cancer patients: A population-based cohort study. Blood 2014; 123: 3972–3978.
- 28.
White C, Noble SIR, Watson M, Swan F, Allgar VL, Napier E, et al. Prevalence, symptom burden, and natural history of deep vein thrombosis in people with advanced cancer in specialist palliative care units (HIDDen): A prospective longitudinal observational study. Lancet Haematol 2019; 6: e79–e88.