Abstract
Background:
Sequential assessment using CT coronary angiography (coronary CT) and nuclear myocardial perfusion imaging (MPI) is considered an anatomical and functional evaluation of coronary artery disease (CAD). However, there can be unexpected radiation exposure. Hybrid MPI with stress-only nuclear MPI and rest CT-MPI using coronary CT may contribute to reducing the radiation dose in sequential assessment with nuclear MPI after coronary CT. We analyzed the diagnostic performance and total radiation dose of hybrid MPI for detection of significant CAD compared with sequential assessment using nuclear MPI after coronary CT.
Methods and Results:
The results for 101 patients who underwent coronary CT, nuclear MPI and invasive coronary angiography within 3 months of all imaging were analyzed. We calculated the summed difference score (SDS) from standard nuclear MPI and hybrid SDS from hybrid MPI, which revealed myocardial ischemia. The diagnostic performance of SDS and hybrid SDS for detecting significant CAD was analyzed using receiver-operating characteristic (ROC) curve analysis. We also compared the total radiation dose of both methods. The area under the ROC curve was not different between SDS and hybrid SDS (0.901 and 0.815, P=0.079). Total radiation dose of hybrid MPI was significantly lower than standard nuclear MPI with CT angiography (4.62 mSv vs. 9.72 mSv, P<0.0001).
Conclusions:
Hybrid MPI showed a precise diagnostic accuracy for significant CAD detection.
Standard nuclear myocardial perfusion imaging (MPI) is based on a combination of rest and stress perfusion imaging and clinically used for qualitative and semiquantitative assessment of ischemia by a visual scoring system.1
Rest nuclear MPI is used for the assessment of myocardial scarring or resting ischemia and is known to have diagnostic value for the estimation of prognosis,2
but has the negative effect of additional radiation exposure in the stress-first MPI protocol.
Previous studies have reported that the stress-only nuclear MPI protocol is one of the best practices for reducing the radiation dose because the subsequent rest perfusion imaging can be omitted if the stress image is completely normal.3,4
However, the requirement for all stress images to be securely assessed on the need for a subsequent resting image, can make a stress-only nuclear MPI protocol problematic. In order to resolve this difficulty of the stress-only MPI protocol, we need to obtain the information supplied by rest nuclear MPI by another non-nuclear imaging modality before stress-only nuclear MPI.
Sequential assessment with stress nuclear MPI after anatomical assessment of the coronary arteries using coronary CT with judgement of intermediate coronary stenosis or insufficient image quality is considered an appropriate clinical choice.5
Clinically, CT perfusion (CT-MPI) in coronary CT may not be assessed. However, the image dataset from coronary CT can be used not only for anatomical assessment of the coronary arteries but also for resting myocardial perfusion, including myocardial scar or infarction detection. A previous study suggested that CT-MPI showed good enough correlation with delayed enhancement on magnetic resonance imaging (MRI) for assessment of the size of the myocardial infarction (correlation coefficient r=0.93, P<0.001).6
Therefore, a protocol of stress-only nuclear MPI in sequential assessment with prior coronary CT protocol would have the benefit of reduced radiation dose and acquisition time.4
In the previous studies or in statements of hybrid imaging with a combination of nuclear MPI and cardiac CT, cardiac CT is assigned only to the detection of the anatomical region of CAD and nuclear MPI is used for physiological assessment of myocardial perfusion.7–12
The objective of our study was to analyze the diagnostic performance and total radiation dose of a hybrid MPI protocol using stress-only nuclear MPI with rest CT-MPI vs. standard sequential assessment with stress/rest nuclear MPI performed after coronary CT.
Methods
Study Population
We analyzed 101 consecutive patients who underwent coronary CT, stress/rest nuclear MPI and then invasive coronary angiography (CAG) within 3 months of all imaging between 1 April 2015 and 30 September 2016. The nuclear MPI study was performed after coronary CT that resulted in equivocal coronary stenosis or insufficient image quality, in addition to direct referrals by physicians (Figure 1). Coronary anatomical findings were validated by invasive CAG following the standard stress/rest nuclear MPI or hybrid MPI protocol of stress-only nuclear MPI and rest CT-MPI (Figure 1).
Coronary CT Protocol
Coronary CT scanning was performed by 320-detector row CT (Aquilion One Vision edition, Canon Medical Systems, Japan). The single-phase real-time bolus tracking method with prospective gating half scan during venous injection of contrast medium (Iomeprol 350 mg/mL) in the right arm was performed for patients with heart rate <65 beats/min and no arrhythmia. The region of interest (ROI) was set in the ascending aorta in order to detect if contrast enhancement reached the threshold level (150 HU). Scan phase was set between 75% and 85% of the R-R interval on ECG for the single-phase scan. Intravenous landiolol hydrochloride (0.125 mg/kg) was used for the patients with heart rate >65 beats/min. Fast-acting nitrates were given sublingually to patients with systolic blood pressure ≥110 mmHg. All the patients were scanned with a peak tube voltage of 120 kV. CT CAG and rest CT-MPI were performed simultaneously as previously described.13
Rest CT-MPI was expressed as a multiplanar reconstruction (MPR) generated by dedicated software (Ziostation2, Ziosoft, Tokyo, Japan).
Interpretation of Rest CT-MPI
The rest CT-MPI was interpreted and scored automatically based on a measured attenuation value of the myocardium prior to the assessment of rest nuclear-MPI. The image of the left ventricular (LV) myocardium on the MPR was analyzed by the double oblique technique for assessment in the short-axial view, and the AHA 17-segment model was used for LV segmentation. Myocardial scar or hypoperfusion on the CT image was assessed with an optimized window setting based on the recommendation of the Society of Cardiovascular Computed Tomography (SCCT).14
Normal myocardium has ≥70 HU of attenuation whereas myocardial infarction is identified as a hypoattenuated segment in the range of 0–20 HU on first-pass CT-MPI.15,16
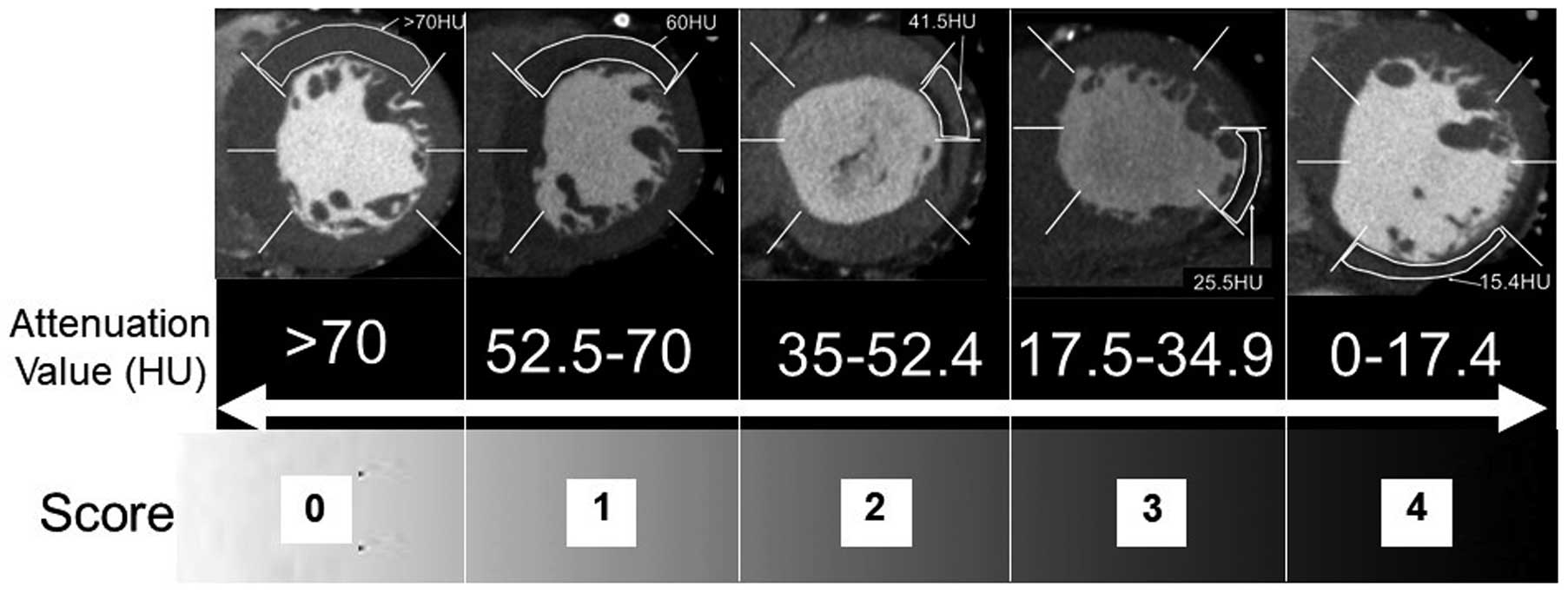
We defined that the attenuation value of myocardium from calculating as an average in the ROI of each segment in the present study, and the scoring scale of CT-MPI was assigned a quartile range of attenuation between 0 and 70 HU using a 5-point scoring system ranging from 0 to 4 (>70 HU: 0; 52.5–70 HU: 1; 35–52.4 HU: 2; 17.5–34.9 HU: 3; 0–17.4 HU: 4) (Figure 2). The summed score for rest CT-MPI was calculated and defined as the CT summed rest score (CT-SRS). In the present study, segments scoring 0 or 1 were determined as normal. CT-SRS was calculated for segments scoring ≥2.
Nuclear MPI was performed by semiconductor scanner D-SPECT (Spectrum Dynamics Medical, Israel). The stress/rest nuclear MPI protocol was a stress-first 1-day protocol with injection of 296 MBq 99 mTc-tetrofosmin for stress and 740 MBq 99 mTc-tetrofosmin for rest imaging. The stress protocol was performed by pharmacological stress (adenosine or dobutamine) or exercise stress testing. Single-photon emission computed tomography (SPECT) images (short-axis, vertical and horizontal long-axis) were generated by Autoquant (Cedars-Sinai Medical Center, LA, USA). The LV ejection fraction (EF) and end-diastolic volume (EDV) in both stress and rest ECG-gated MPI were automatically calculated by the same software.
Interpretation of Nuclear MPI
The nuclear MPI was scored semiquantitatively by 2 experienced readers based on the 17-segment model of the LV using a 5-point scoring system (0, normal uptake; 1, mildly reduced uptake; 2, moderately reduced uptake; 3, severely reduced uptake; 4, almost no uptake).17,18
Consensus reading between readers resolved discordance of image interpretation. The SRS, summed stress score (SSS) and summed difference score (SDS) were calculated as previously described.19
Hybrid Assessment of CAD With Stress-Only Nuclear MPI and Rest CT-MPI
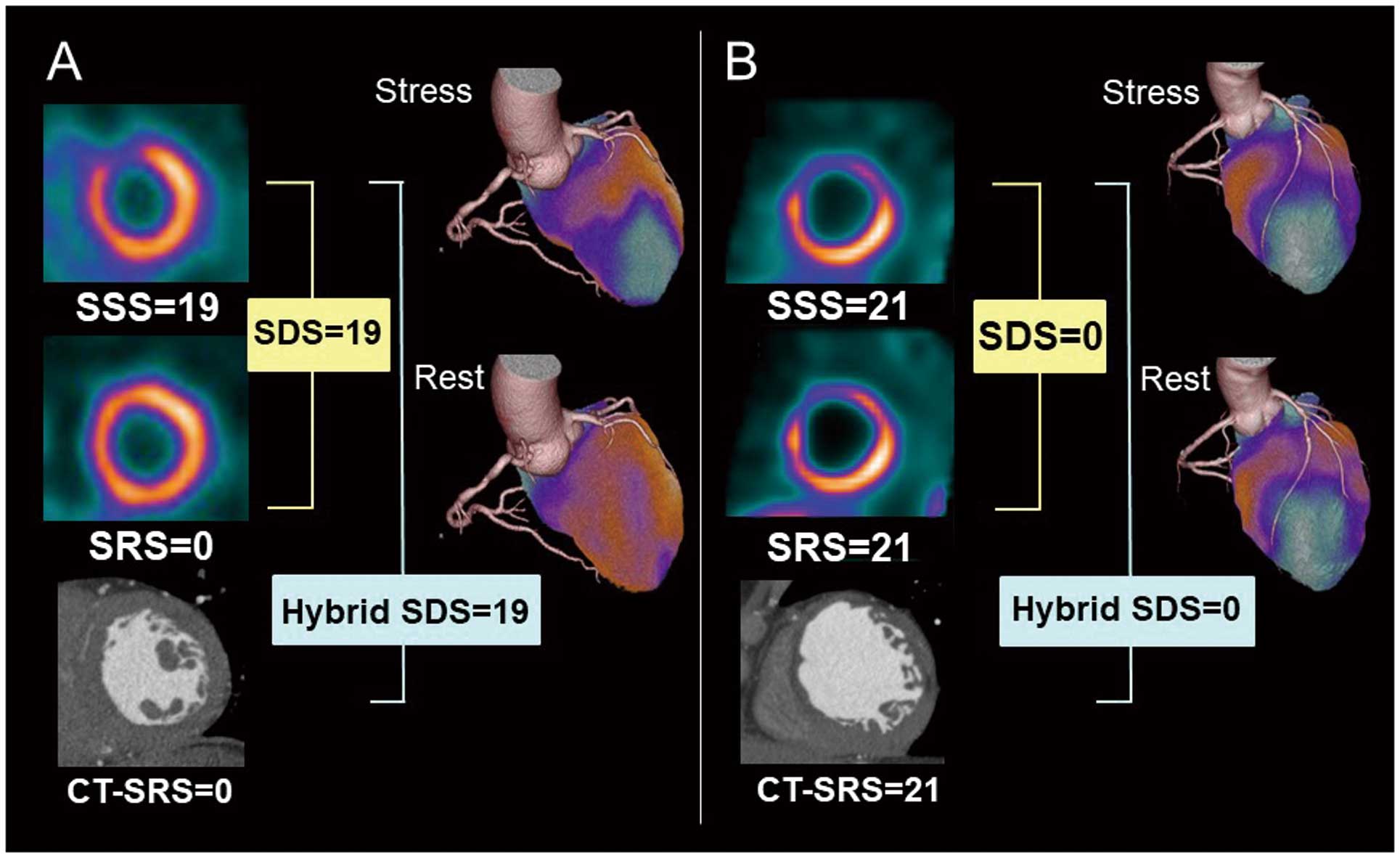
In order to compare the diagnostic performance of detecting significant CAD between standard nuclear stress/rest MPI and the hybrid MPI, we defined a new index of hybrid SDS by subtracting the CT-SRS from SSS. Examples of the hybrid SDS for ischemic and infarcted patients are shown in
Figure 3. In this study the CT-SRS and nuclear SRS were scored independently; we scored the hybrid SDS as 0 when the CT-SRS was larger than the SSS.
Comparison of Total Radiation Dose
We compared the total estimated effective radiation dose between hybrid MPI and stress/rest nuclear MPI with prior coronary CT, based on the recommendation of the International Commission on Radiological Protection (ICRP).20
For cardiac CT it was calculated using the dose-length product and a conversion factor of 0.014 mSv/(mGy · cm). The radiation dose of stress and rest nuclear MPI with 99 mTc-tetrofosmin was calculated by a conversion factor of 0.0069 mSv/MBq.
Invasive CAG
All patients underwent invasive CAG within 3 months of nuclear MPI. Significant CAD was defined as stenosis ≥75% in >1 coronary artery or ≥75% stenosis in the left main coronary artery.
Statistical Analysis
Continuous variables are expressed as median and quartile. The correlation between SRS and CT-SRS was analyzed by Spearman’s rank regression test, in addition to the same analysis between hybrid SDS and SDS. We calculated the sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and accuracy in detecting significant CAD on a per-patient basis with usual equations. Paired t-test was performed for the evaluation of EF and EDV between stress and rest. Receiver-operating characteristic (ROC) curve analysis for detection of significant CAD was performed and area under the ROC curve (AUC) was calculated. We compared the ROC curves of SDS and hybrid SDS. We determined the cutoff value of hybrid SDS and SDS for detection of significant ischemia as ≥3.
The Wilcoxson test was used for comparison of total effective radiation dose between standard stress/rest nuclear MPI with prior coronary CT and hybrid MPI. Statistical analysis was performed by dedicated software (MedCalc ver. 19.1.5).
Research Ethics
This study was performed in accordance with the Declaration of Helsinki and the ethical standards of the hospital’s institutional review board (reference no. 20170904). Written informed consent was given by all the study patients.
Results
Patients’ Characteristics (Table 1)
Coronary risk factors were as follows: hypertension, 74.3%; dyslipidemia, 56.4%; diabetes, 37.6%; current smoking, 11.9%. The median body mass index (BMI) was 25.0 (kg/m2).
Table 1.
Patients’ Characteristics
| |
Median [quartile] or n (%) |
| n |
101 |
| Age |
67.0 [59.0, 74.0] |
| Female |
26 (25.7) |
| Height (cm) |
165.0 [159.0, 170.0] |
| Weight (kg) |
68.0 [56.0, 77.0] |
| BMI (kg/m2) |
25.0 [22.0, 28.0] |
| Prior MI |
16 (16.0) |
| Prior PCI |
33 (32.7) |
| Hypertension |
75 (74.3) |
| Dyslipidemia |
57 (56.4) |
| Diabetes |
38 (37.6) |
| Current smoking |
12 (11.9) |
| Family history of CAD |
2 (2.0) |
| CKD |
17 (16.8) |
BMI, body mass index; CAD, coronary artery disease; CKD, chronic kidney disease; MI, myocardial infarction; PCI, percutaneous coronary intervention.
We determined the cutoff value of hybrid SDS and SDS for detection of significant CAD as ≥3. Adenosine stress test was performed in 96 patients (95.0%), 2 patients (1.9%) underwent dobutamine stress test and 3 patients (2.9%) had an exercise stress test. Defect scores and functional parameters in nuclear MPI are listed in
Table 2. The median nuclear SRS was 0 but 9 patients had nuclear SRS ≥3 and 16 patients had CT-SRS ≥3 (Tables 2,3).
Table 2.
Defect Score and Functional Parameters in ECG-Gated MPI
| |
Median [quartile] |
| n |
101 |
| SSS |
2.0 [1, 5.0] |
| SRS |
0 [0, 1.0] |
| SDS |
2.0 [0, 3.0] |
| EF at stress (%) |
63.0 [53.0, 69.0]* |
| EF at rest (%) |
67.0 [55.0, 73.0] |
| EDV at stress (mL) |
83.0 [64.0, 102.0]** |
| EDV at rest (mL) |
75.0 [61.0, 96.0] |
*P<0.0001, paired t-test between stress and rest EF; **P<0.0001, paired t-test between stress and rest EDV. EDV, end-diastolic volume; EF, ejection fraction; SDS, summed difference score; SRS, summed rest score; SSS, summed stress score.
Table 3.
Comparison of CT-SRS, SRS, Hybrid SDS and SDS
| |
SRS (%) |
CT-SRS (%) |
SDS (%) |
Hybrid SDS (%) |
| <3 |
≥3 |
<3 |
≥3 |
<3 |
≥3 |
<3 |
≥3 |
| CAD (−) n=74 |
65 (87.8) |
9 (12.2) |
58 (78.4) |
16 (21.6) |
57 (77.0) |
17 (23.0) |
58 (78.4) |
16 (21.6) |
| CAD (+) n=27 |
20 (74.1) |
7 (25.9) |
20 (74.1) |
7 (25.9) |
3 (11.1) |
24 (88.9) |
7 (25.9) |
20 (74.1) |
CAD, coronary artery disease; SDS, summed difference score; SRS, summed rest score.
Median heart rate during CT scanning was 58 beats/min, the median contrast dose was 50 mL, and 15 patients (14.8%) were able to undergo coronary CT without the β-blocker.
Invasive CAG Findings
Of the 101 patients who underwent invasive CAG, 18 (17.8%) had 1-vessel disease, 5 (4.9%) had 2-vessel disease, and 4 (3.9%) had 3-vessel disease; 14 patients (13.8%) had significant stenosis in the left anterior descending coronary artery, 17 (16.8%) had it in the left circumflex coronary artery, and 9 (8.9%) had it in the right coronary artery.
Comparison of Nuclear SRS and CT-SRS
The CT-SRS score for assessment of myocardial scar or infarction significantly correlated with the SRS results from nuclear MPI (correlation coefficient r=0.511, 95% confidence interval (CI): 0.351–0.643, P<0.0001). Scatter plots and Bland-Altman plots are shown in
Figure 4A,B. There were 24 patients who scored SRS=0 and CT-SRS ≥1 and none of patients had visible myocardial scar by CT-MPI. Of these cases, 11 (45.8%) were scored CT-SRS=2 and 13 cases (54.2%) had CT-SRS ≥2 in the apex and adjacent segment. There were 19 cases of CT-SRS=0 and SRS ≥1, and of these, 12 patients (63.2%) were scored SRS=1, 2 patients (10.5%) were scored SRS=2, including a patient with dilated cardiomyopathy, and 4 patients (21.1%) with chronic total occlusion (CTO) of the coronary artery had SRS ≥3. The comparison of CT-SRS and nuclear SRS in CAD (+) and CAD (−) groups are shown in
Table 3. The number of patients scored CT-SRS ≥3 was larger than the number of the patients scored nuclear SRS ≥3 in the CAD (−) group, but the same number of patients scored ≥3 by CT-SRS and nuclear SRS in the CAD (+) group.

Scatter plots and Bland-Altman plots for comparison of nuclear SDS and hybrid SDS are shown in
Figure 4C,D. The value of SDS and hybrid SDS were significantly correlated (r=0.837, P<0.0001, 95% CI: 0.766–0.887). The number of the patients with hybrid SDS ≥3 in CAD (+) group was similar to that for patients with SDS ≥3 in the CAD (−) group (16 (21.6%) vs. 17 (23.0%), respectively), whereas the number of the patients with hybrid SDS ≥3 was slightly lower than the number with SDS ≥3 in the CAD (+) group (20 (74.1%) vs. 24 (88.9%), respectively) (Table 3).
Diagnostic Performance of Hybrid SDS
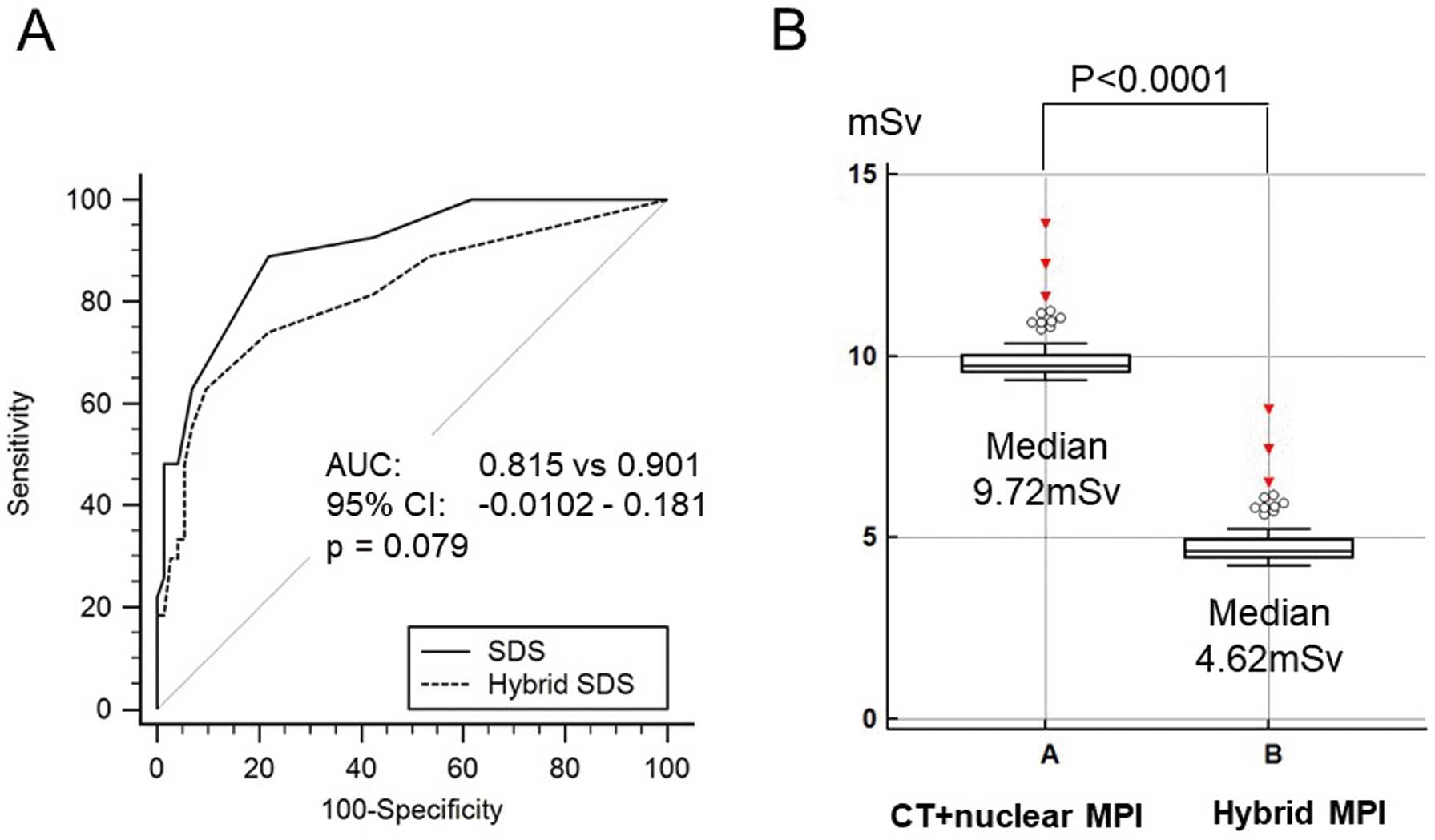
The diagnostic performance of the hybrid SDS for detection of significant CAD on a per-patient basis was not significantly different from the result of standard stress/rest nuclear MPI (AUC: 0.815 vs. 0.901, 95% CI: −0.012 to 0.181, P=0.079;
Figure 5A). Per-patient analysis, sensitivity, specificity, PPV, NPV and accuracy with a cutoff value of SDS and hybrid SDS ≥3 for detection of significant CAD were as follows: 88.9%, 77.0%, 58.5%, 95.0%, 80.2%, for SDS; 74.1%, 78.4%, 55.6%, 89.2%, 77.2%, for hybrid SDS, respectively. Comparisons of the hybrid SDS and SDS in the CAD (+) and CAD (−) groups are shown in
Table 3. The hybrid SDS tended to have lower sensitivity and higher specificity than the SDS.
Comparison of Effective Radiation Dose
Total effective radiation dose for hybrid MPI using stress-only nuclear MPI with prior coronary CT angiography was significantly lower than with standard sequential assessment using stress/rest nuclear MPI with prior rest CT angiography (median: 4.62 mSv vs. 9.72 mSv, P<0.0001) (Figure 5B).
Discussion
In our study, automated analysis of myocardial scarring using CT-SRS derived from the attenuation value of rest CT-MPI was significantly associated with the SRS derived from nuclear MPI with a semiconductor scanner as well as showing a correlation between the hybrid SDS and SDS. Lower sensitivity and higher specificity of the hybrid SDS may be attributable to the tendency for CT-SRS to be scored higher than the SRS, which results in a smaller score for the hybrid SDS. Although CT-SRS is not dependent on visual analysis, we may need to be careful about the tendency for a higher score of CT-SRS. In our results CT-SRS tended to show a higher defect score in the apex even in patients with SRS=0. The lower attenuation value of CT-MPI in the apical segment can be explained by the distal area of the coronary territory. Thus, it should be noted that CT-SRS tends to have higher sensitivity than nuclear SRS due to lower attenuation value in the apical segment of CT-MPI. In addition, there were several discrepant cases with CT-SRS=0 and SRS ≥2 in patients with CTO of the coronary artery, which can be attributed to underestimation of viable myocardium by the 99 mTc-labeled tracer.21
In our study, rest CT-MPI was obtained only from the first-pass narrow-band single-shot image without delayed scanning, which may not be enough for detecting myocardial scar or infarction. However, CT-MPI derived from rest coronary CT is useful for detecting myocardial scar, and the necessity of myocardial scar imaging with delayed CT scan is still controversial. In fact, Bettencourt et al reported that the diagnostic performance of rest and stress CT-MPI for detection of CAD was not significantly improved by additional delayed CT-MPI.22
Our results clearly showed a significant association between the rest nuclear SRS and CT-SRS, which may be consistent with the previous report by Yoshinaga et al that described similarity of the myocardial extraction fraction between 99 mTc tracer and iodine contrast medium.23
In the present study, we performed stress imaging with 296 MBq of 99 mTc-labeled tracer and a semiconductor scanner. It may be possible to perform stress-only nuclear MPI with a lower dose of 99 mTc. The imaging guideline of the American Society of Nuclear Cardiology (ASNC) in 2016 recommended 148–222 MBq of 99 mTc tracer for stress-only nuclear MPI if newer technology, including semiconductor scanners, is available.24
Furthermore, a previous study reported the potential of semiconductor scanners to achieve an extremely lower dose protocol using <148 MBq of 99 mTc without sacrificing image quality or diagnostic performance.25,26
Stress-only nuclear MPI with 296 MBq of 99 mTc tracer can be performed even with a conventional gamma camera in a patient with BMI ≤25 (kg/m2).24
Adjustment of 99 mTc activity based on the patient’s BMI must be considered if a conventional gamma camera is used for stress nuclear MPI if diagnostic performance is not to be reduced.24,27
Zafrir et al previously reported using a half-dose (185 MBq) 99 mTc protocol for stress nuclear MPI using a conventional gamma camera and dedicated image processing.24,28
To our knowledge, this is the first study to assess myocardial ischemia using a combination of 2 different modalities: stress nuclear MPI for depiction of MPI in the hyperemic state and rest CT-MPI for detection of myocardial scar or infarction. 99 mTc-tetrofosmin and 201Tl are the most commonly used radiopharmaceuticals for nuclear MPI in Japan. 99 mTc has a shorter half-life (6 h) than 201Tl (73 h), which may lead to minimized radiation dose for sequential assessment by stress-only nuclear MPI and rest CT-MPI. Mouden et al reported that stress nuclear MPI with a semiconductor scanner detected patients more frequently as normal, which was identical to 1-year clinical follow-up, in comparison with conventional gamma camera and concluded that semiconductor scanners lower the need for an additional rest scan, resulting in lower radiation dose.29
Stress-only nuclear MPI protocol has not been considered practical because of the difficulty of secure assessment of the need for additional rest imaging, although it is already known as an effective method of reducing the radiation dose.3,4
Our findings underscore the fact that a hybrid MPI protocol may be a method for decreasing the radiation dose by half. Thus, hybrid assessment using stress-only nuclear MPI with a semiconductor scanner after coronary CT for the assessment of rest MPI may be confidently selected.
Study Limitations
This was a single-center retrospective study. Rest CT-MPI findings were not confirmed by cardiac MRI with delayed enhancement as the gold standard of myocardial scar assessment. Only 16% of patients had a prior myocardial infarction in the present study. Further research in a larger number of patients with prior myocardial infarction is needed.
Conclusions
Hybrid assessment of myocardial ischemia using a combination of stress-only nuclear MPI and rest CT-MPI had equivalent diagnostic performance and significantly reduced the total radiation dose in comparison to the standard sequential assessment with stress- and rest nuclear MPI with prior coronary CT.
Conflicts of Interest
The authors do not have any conflict of interest to declare.
Data Availability
The de-identified participant data will not be shared.
Disclosures
The authors declare no conflicts of interest.
IRB Information
Name of the institutional review board (IRB): the Review Board of Clinical Research, Nihon University Hospital. Reference no. IRB: 20170904.
References
- 1.
Holly TA, Abbott BG, Al-Mallah M, Calnon DA, Cohen MC, DiFilippo FP, et al. Single photon-emission computed tomography: ASNC Imaging Guideline For Nuclear Cardiology Procedures. J Nucl Cardiol 2010; 17: 941–973.
- 2.
Shaw LJ, Hendel RC, Heller GV, Borges-Neto S, Cerqueira M, Berman DS. Prognostic estimation of coronary artery disease risk with resting perfusion abnormalities and stress ischemia on myocardial perfusion SPECT. J Nucl Cardiol Clin 2008; 15: 762–773.
- 3.
Einstein AJ, Pascual TN, Mercuri M, Karthikeyan G, Vitola JV, Mahmarian JJ, et al. Current worldwide nuclear cardiology practices and radiation exposure: RESULTS from the 65 country IAEA Nuclear Cardiology Protocols Cross-Sectional Study (INCAPS). Eur Heart J 2015; 36: 1689–1696.
- 4.
Ueyama T, Takehana K, Maeba H, Iwasaka T. Prognostic value of normal stress-only technetium-99 m myocardial perfusion imaging protocol: Comparison with standard stress-rest protocol. Circ J 2012; 76: 2386–2391.
- 5.
Ronan G, Wolk MJ, Bailey SR, Doherty JU, Douglas PS, Hendel RC, et al. ACCF/AHA/ASE/ASNC/HFSA/HRS/SCAI/SCCT/SCMR/STS 2013 multimodality appropriate use criteria for the detection and risk assessment of stable ischemic heart disease: A report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, American Heart Association, American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Failure Society of America, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, and Society of Thoracic Surgeons. J Nucl Cardiol 2014; 21: 192–220.
- 6.
Gerber BL, Belge B, Legros GJ, Lim P, Poncelet A, Pasquet A, et al. Characterization of acute and chronic myocardial infarcts by multidetector computed tomography: Comparison with contrast-enhanced magnetic resonance. Circulation 2006; 113: 823–833.
- 7.
Flotats A, Knuuti J, Gutberlet M, Marcassa C, Bengel FM, Kaufmann PA, et al. Hybrid cardiac imaging: SPECT/CT and PET/CT. A joint position statement by the European Association of Nuclear Medicine (EANM), the European Society of Cardiac Radiology (ESCR) and the European Council of Nuclear Cardiology (ECNC). Eur J Nucl Med Mol Imaging 2011; 38: 201–212.
- 8.
Grani C, Benz DC, Schmied C, Vontobel J, Mikulicic F, Possner M, et al. Hybrid CCTA/SPECT myocardial perfusion imaging findings in patients with anomalous origin of coronary arteries from the opposite sinus and suspected concomitant coronary artery disease. J Nucl Cardiol 2017; 24: 226–234.
- 9.
Pazhenkottil AP, Nkoulou RN, Ghadri JR, Herzog BA, Buechel RR, Kuest SM, et al. Prognostic value of cardiac hybrid imaging integrating single-photon emission computed tomography with coronary computed tomography angiography. Eur Heart J 2011; 32: 1465–1471.
- 10.
Rispler S, Aronson D, Abadi S, Roguin A, Engel A, Beyar R, et al. Integrated SPECT/CT for assessment of haemodynamically significant coronary artery lesions in patients with acute coronary syndrome. Eur J Nucl Med Mol Imaging 2011; 38: 1917–1925.
- 11.
Schaap J, de Groot JA, Nieman K, Meijboom WB, Boekholdt SM, Kauling RM, et al. Added value of hybrid myocardial perfusion SPECT and CT coronary angiography in the diagnosis of coronary artery disease. Eur Heart J Cardiovasc Imaging 2014; 15: 1281–1288.
- 12.
Schaap J, de Groot JA, Nieman K, Meijboom WB, Boekholdt SM, Post MC, et al. Hybrid myocardial perfusion SPECT/CT coronary angiography and invasive coronary angiography in patients with stable angina pectoris lead to similar treatment decisions. Heart 2013; 99: 188–194.
- 13.
George RT, Arbab-Zadeh A, Cerci RJ, Vavere AL, Kitagawa K, Dewey M, et al. Diagnostic performance of combined noninvasive coronary angiography and myocardial perfusion imaging using 320-MDCT: The CT angiography and perfusion methods of the CORE320 multicenter multinational diagnostic study. Am J Roentgenol 2011; 197: 829–837.
- 14.
Leipsic J, Abbara S, Achenbach S, Cury R, Earls JP, Mancini GJ, et al. SCCT guidelines for the interpretation and reporting of coronary CT angiography: A report of the Society of Cardiovascular Computed Tomography Guidelines Committee. J Cardiovasc Comput Tomogr 2014; 8: 342–358.
- 15.
Mehra VC, Valdiviezo C, Arbab-Zadeh A, Ko BS, Seneviratne SK, Cerci R, et al. A stepwise approach to the visual interpretation of CT-based myocardial perfusion. J Cardiovasc Comput Tomogr 2011; 5: 357–369.
- 16.
Mendoza DD, Joshi SB, Weissman G, Taylor AJ, Weigold WG. Viability imaging by cardiac computed tomography. J Cardiovasc Comput Tomogr 2010; 4: 83–91.
- 17.
Berman DS, Kiat H, Friedman JD, Wang FP, van Train K, Matzer L, et al. Separate acquisition rest thallium-201/stress technetium-99 m sestamibi dual-isotope myocardial perfusion single-photon emission computed tomography: A clinical validation study. J Am Coll Cardiol 1993; 22: 1455–1464.
- 18.
Yoda S, Sato Y, Matsumoto N, Tani S, Takayama T, Nishina H, et al. Incremental value of regional wall motion analysis immediately after exercise for the detection of single-vessel coronary artery disease: Study by separate acquisition, dual-isotope ECG-gated single-photon emission computed tomography. Circ J 2005; 69: 301–305.
- 19.
Berman DS, Kang X, Van Train KF, Lewin HC, Cohen I, Areeda J, et al. Comparative prognostic value of automatic quantitative analysis versus semiquantitative visual analysis of exercise myocardial perfusion single-photon emission computed tomography. J Am Coll Cardiol 1998; 32: 1987–1995.
- 20.
Cousins C, Miller DL, Bernardi G, Rehani MM, Schofield P, Vano E, et al. ICRP Publication 120: Radiological protection in cardiology. Ann ICRP 2013; 42: 1–125.
- 21.
Cuocolo A, Pace L, Ricciardelli B, Chiariello M, Trimarco B, Salvatore M. Identification of viable myocardium in patients with chronic coronary artery disease: Comparison of thallium-201 scintigraphy with reinjection and technetium-99 m-methoxyisobutyl isonitrile. J Nucl Med 1992; 33: 505–511.
- 22.
Bettencourt N, Ferreira ND, Leite D, Carvalho M, Ferreira Wda S, Schuster A, et al. CAD detection in patients with intermediate-high pre-test probability: Low-dose CT delayed enhancement detects ischemic myocardial scar with moderate accuracy but does not improve performance of a stress-rest CT perfusion protocol. JACC Cardiovasc Imaging 2013; 6: 1062–1071.
- 23.
Yoshinaga K, Tomiyama Y, Suzuki E, Tamaki N. Myocardial blood flow quantification using positron-emission tomography: Analysis and practice in the clinical setting. Circ J 2013; 77: 1662–1671.
- 24.
Henzlova MJ, Duvall WL, Einstein AJ, Travin MI, Verberne HJ. ASNC imaging guidelines for SPECT nuclear cardiology procedures: Stress, protocols, and tracers. J Nucl Cardiol 2016; 23: 606–639.
- 25.
Nakazato R, Berman DS, Hayes SW, Fish M, Padgett R, Xu Y, et al. Myocardial perfusion imaging with a solid-state camera: Simulation of a very low dose imaging protocol. J Nucl Med 2013; 54: 373–379.
- 26.
Perrin M, Djaballah W, Moulin F, Claudin M, Veran N, Imbert L, et al. Stress-first protocol for myocardial perfusion SPECT imaging with semiconductor cameras: High diagnostic performances with significant reduction in patient radiation doses. Eur J Nucl Med Mol Imaging 2015; 42: 1004–1011.
- 27.
Sharir T, Pinskiy M, Pardes A, Rochman A, Prokhorov V, Kovalski G, et al. Comparison of the diagnostic accuracies of very low stress-dose with standard-dose myocardial perfusion imaging: Automated quantification of one-day, stress-first SPECT using a CZT camera. J Nucl Cardiol 2016; 23: 11–20.
- 28.
Zafrir N, Bental T, Solodky A, Ben-Shlomo A, Mats I, Hassid Y, et al. Feasibility of myocardial perfusion imaging with half the radiation dose in obese patients using ordered-subset expectation maximization with resolution recovery software. J Nucl Cardiol 2013; 20: 111–119.
- 29.
Mouden M, Timmer JR, Ottervanger JP, Reiffers S, Oostdijk AH, Knollema S, et al. Impact of a new ultrafast CZT SPECT camera for myocardial perfusion imaging: Fewer equivocal results and lower radiation dose. Eur J Nucl Med Mol Imaging 2012; 39: 1048–1055.