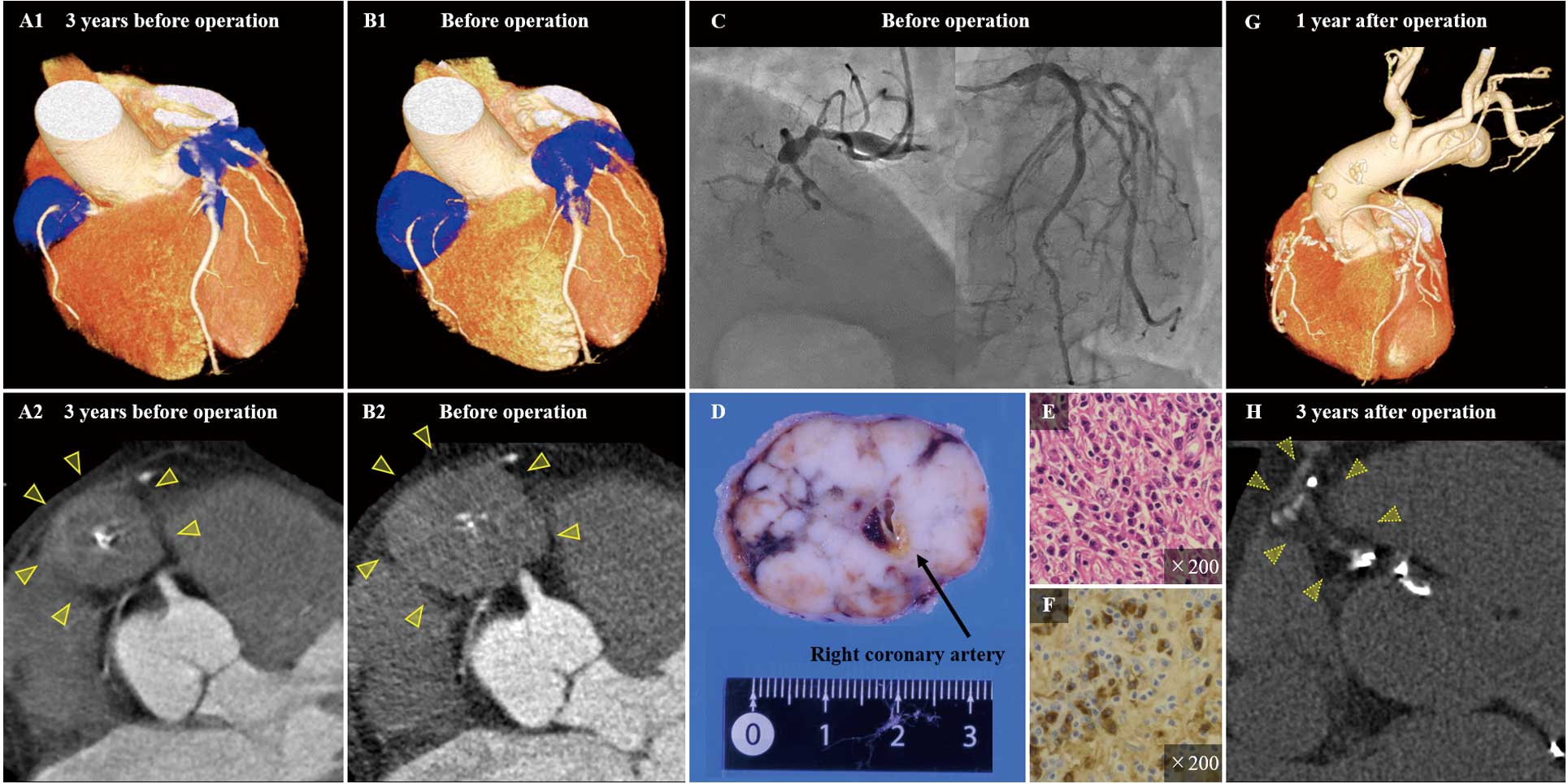
A 66-year-old man underwent emergency surgical repair for acute rupture of an abdominal aortic aneurysm. Cardiac computed tomography angiography (CCTA) revealed an asymptomatic coronary aneurysm (Figure A); however, the patient refused further investigation. Three years later, he presented with unstable angina and CCTA showed progressively developed aneurysms in all coronary arteries (Figure B). Subsequent coronary angiography confirmed a subtotal occlusion in the right coronary artery (Figure C). We performed coronary artery bypass grafting with ligation and concomitant resection of the aneurysms. Histopathological evaluation confirmed lymphoplasmacytic infiltration with fibrosis and immunoglobulin G4 (IgG4)-positive plasma cells (Figure D–F). Blood examination revealed elevated IgG4 (1,060 mg/dL) with hypergammaglobulinemia. We diagnosed IgG4-related periarteritis with aneurysms. Further examinations revealed no abnormalities except for the treated lesions. He has been closely followed up while receiving conservative treatment without steroids, and IgG4-related clinical findings has not been observed for more than 3 years post-operation (Figure G,H).
Prognosis of IgG4-related disease reportedly depends on myocardial ischemia, aortic dissection, and aneurysmal rupture.1
Surgical intervention can help effectively diagnose and treat ischemic IgG4-related coronary pericarditis with aneurysms. The necessity of adjuvant steroid treatment after surgery depends on the presence of residual IgG4-related disease, and the long-term postoperative outcome of IgG4-related coronary periarteritis with aneurysms remains unknown. Our observations suggest that although careful postoperative monitoring may be mandatory, optimal surgical intervention can be curative for localized coronary periarteritis with aneurysms.
Acknowledgment
We thank Takanori Manabe, RT, for image processing support.
Conflicts of Interest
None.
Consent
The patient consented to the publication of this report.
