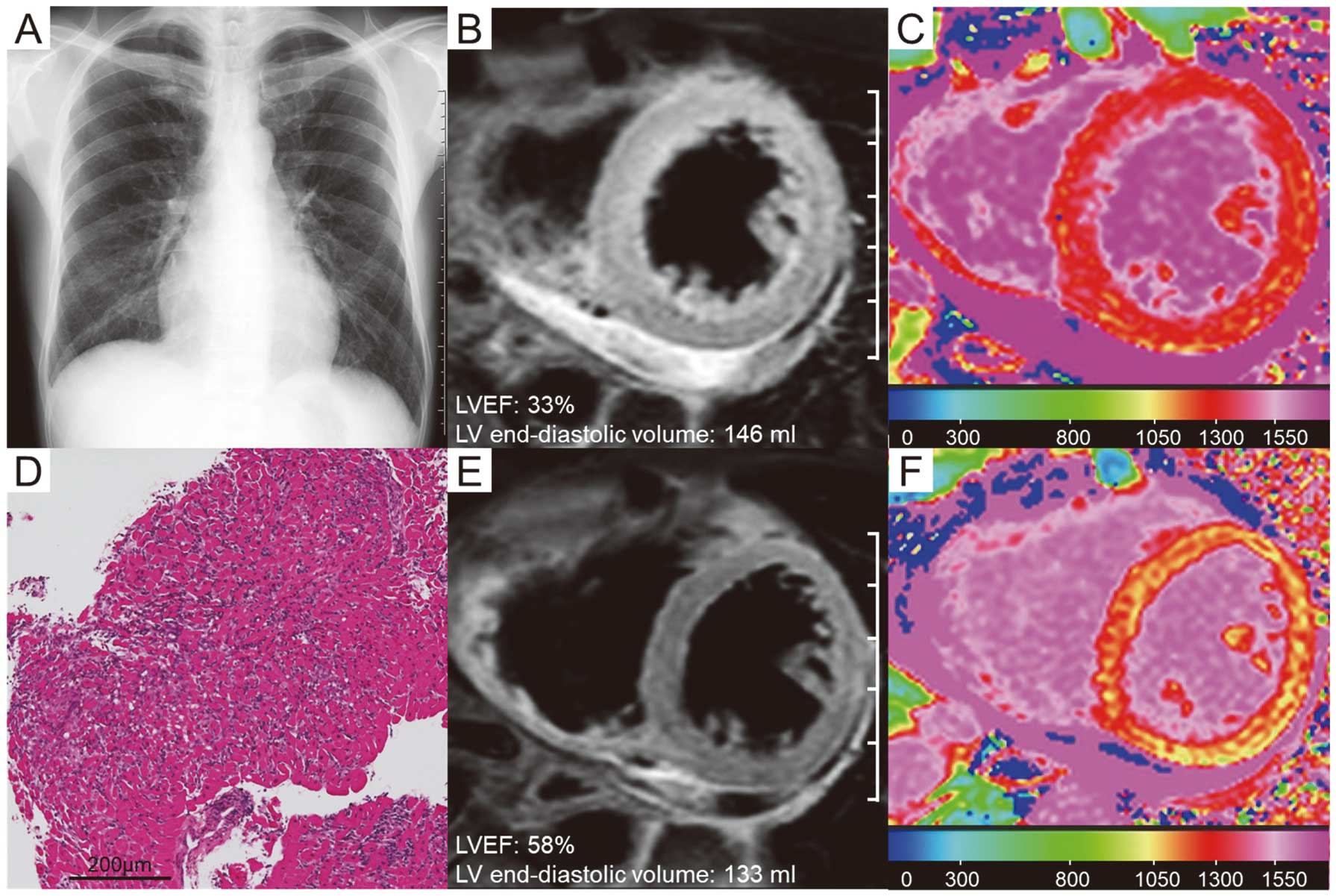
A previously healthy 49-year-old man presented to hospital 11 days after a 2nd dose of the BNT162b2-mRNA (Pfizer-BioNTech) vaccine for essential workers. He began to notice fever, appetite loss, cough, and orthopnea 4 days after vaccination. Oral nonsteroidal anti-inflammatory drug and antibiotics for several days failed to relieve his symptoms. On admission, physical examination revealed fever of 37.3℃, blood pressure of 95/67 mmHg, pulse of 93 beats/min and pericardial friction rub on auscultation. ECG demonstrated low voltage in the limb leads and poor R waves in V1–2. Chest X-ray showed mild congestion (Figure A). Laboratory evaluation showed elevated B-type natriuretic peptide of 1,113.0 pg/mL, troponin I of 4,364.5 pg/mL, and C-reactive protein of 19.78 mg/mL. Blood cell count was normal with no peripheral eosinophilia. Nasopharyngeal SARS CoV-2 antigen and other viral studies were negative. Cardiac magnetic resonance imaging (CMR) showed diffuse myocardial edema on T2-weighted imaging (Figure B), reduced left ventricular ejection fraction of 33%, diffuse late gadolinium enhancement (LGE), and increased global native T1 value of 1,301 ms (Figure C). Endomyocardial biopsy revealed diffuse lymphocytic infiltrates and some eosinophils (Figure D), confirming the diagnosis of myocarditis. Oral diuretics and aspirin relieved his symptoms. CMR on day12 showed resolution of the myocardial edema (Figure E), decrease in the native T1 value to 1,176 ms (Figure F), and partial LGE. He was discharged home on day 15.
To our knowledge, this is the first case of presumed COVID-19 vaccine-related myocarditis diagnosed by myocardial biopsy and CMR in a middle-aged man. Although myocarditis following COVID-19 vaccine can be mild and occur in the young,1
more intense myocarditis might occur in individuals of any age. Thus, careful attention to myocarditis is necessary.
Disclosure
K.I.-Y. received an independent medical educational grant >1,000,000 yen from Pfizer Japan Inc.
