Circulation Journal Awards for the Year 2017
Article ID: CJ-66-0149

Details
Article ID: CJ-66-0149
Dear Colleagues,
On behalf of the Editorial Team of Circulation Journal, I am pleased to announce the Circulation Journal Awards for the Year 2017.
The aim of these Awards is to recognize papers published in 2017, both clinical and experimental studies, that were highly appreciated by the Editorial Team. The selection process comprises 2 steps. In the first step, from 256 original papers published in the Journal in 2017, our 40 Japanese Associate Editors selected papers with a high scientific level in their respective fields, and in the second step, the 4 Associate Editorial Teams (10 on 1 team) further evaluated the selected papers in terms of originality, contribution to cardiovascular science, manner of paper preparation, and future possibilities.
In the year of 2017, the following 8 papers have been selected for the Circulation Journal Awards.
(Circ J 2017; 81: 96–102)1
| Variant Aldehyde Dehydrogenase 2 (ALDH2*2 in East Asians Interactively Exacerbates Tobacco Smoking Risk for Coronary Spasm ― Possible Role of Reactive Aldehydes ― Yuji Mizuno, Seiji Hokimoto, Eisaku Harada, Kenji Kinoshita, Michihiro Yoshimura, Hirofumi Yasue (Division of Cardiovascular Medicine, Kumamoto Kinoh Hospital, Kumamoto Aging Research Institute, Kumamoto (Y.M., E.H., H.Y.); Department of Cardiovascular Medicine, Graduate School of Medical Sciences, Kumamoto University, Kumamoto (S.H.); School of Pharmaceutical Sciences, Mukogawa Women’s University, Nishinomiya (K.K.); and Division of Cardiology, Department of Internal Medicine, The Jikei University School of Medicine, Tokyo (M.Y.), Japan) |
 |
Background: Coronary spastic angina (CSA) is common among East Asians and tobacco smoking (TS) is an established risk factor for CSA. Aldehyde dehydrogenase 2 (ALDH2) plays a key role in removing reactive toxic aldehydes and a deficient variant ALDH2 genotype (ALDH2*2) is prevalent among East Asians. We examined the interaction between TS and ALDH2*2 as a risk factor for CSA to better understand the disease pathogenesis.
Methods and Results: The study subjects comprised 410 patients (258 men, 152 women; mean age, 66.3±11.5) in whom intracoronary injection of acetylcholine was performed on suspicion of CSA. ALDH2 genotyping was performed by direct application of the Taqman polymerase chain reaction system. Of the study subjects, 244 had CSA proven and 166 were non-CSA. The frequencies of male sex, ALDH2*2, alcohol flushing syndrome, TS, coronary organic stenosis, and plasma levels of uric acid were higher (P<0.001, P<0.001, P<0.001, P<0.001, P<0.001, and P=0.015, respectively) and that of high-density lipoprotein cholesterol lower (P=0.002) in the CSA than non-CSA group. Multivariable logistic regression analysis revealed that ALDH2*2 and TS were significant risk factors for CSA (P<0.001 and P=0.002, respectively). ALDH2*2 exacerbated TS risk for CSA more than the multiplicative effects of each.
Conclusions: ALDH2*2 synergistically exacerbates TS risk for CSA, probably through aldehydes.

Relationship of ALDH2*2 and tobacco smoking (TS) with coronary spasm. ALDH2*2 with deficient ALDH2 activity leads to increased reactive aldehydes, such as 4-hydoxy-2 nonenal, associated with increased reactive oxygen species, which are augmented by TS. Increased reactive aldehydes and reactive oxygen species cause coronary artery injury, which may lead to coronary spasm. ALDH2*2 carriers also have increased acetaldehyde because of deficient ALDH2 activity on alcohol intake and may thereby suffer from alcohol flushing syndrome. ALDH, aldehyde dehydrogenase.
(Circ J 2017; 81: 1116–1122)2
| AVJ-514 Trial ― Baseline Characteristics and 30-Day Outcomes Following MitraClip® Treatment in a Japanese Cohort ― Kentaro Hayashida, Satoshi Yasuda, Takashi Matsumoto, Makoto Amaki, Shingo Mizuno, Tetsuya Tobaru, Kentaro Jujo, Tatsushi Ootomo, Junichi Yamaguchi, Keiichi Fukuda, Shigeru Saito, Elyse Foster, Atif Qasim, Masafumi Kitakaze, Ryohei Yozu, Morimasa Takayama (Keio University School of Medicine, Tokyo (K.H., K.F., R.Y.); National Cerebral and Cardiovascular Center, Suita (S.Y., M.A., M.K.); Sendai Kousei Hospital, Sendai (T.M., T.O.); Shonan Kamakura General Hospital, Kanagawa (S.M., S.S.); Sakakibara Heart Institute, Tokyo (T.T., M.T.); Tokyo Women’s Medical University Hospital, Tokyo (K.J., J.Y.), Japan; and University of California at San Francisco, CA (E.F., A.Q.), USA) |
 |
Background: The MitraClip® system is a transcatheter-based therapeutic option for patients with chronic mitral regurgitation (MR) who are at high risk for surgery. A prospective, multicenter, single-arm study was initiated to confirm the transferability of this system to Japan.
Methods and Results: Patients with symptomatic chronic moderate-to-severe (3+) or severe (4+) functional or degenerative MR with a Society of Thoracic Surgery (STS) score ≥8%, or the presence of 1 predefined risk factor were enrolled. Patients with left ventricular (LV) ejection fraction (EF) <30% were excluded. MR severity and LV function were assessed by an independent echocardiography core lab. Primary outcome included major adverse events (MAE) at 30 days and acute procedural success (APS). A total of 30 patients (age: 80±7 years; STS score: 10.3%±6.6%) were treated with the MitraClip®. At baseline, all patients had MR 3+/4+ with 53%/47% patients with degenerative/functional etiology with mean LVEF of 50.2±12.8%, and 37% of patients were NYHA class III/IV. APS was achieved in 86.7% with no occurrence of MAE. At 30 days, 86.7% of patients had MR ≤2+ and 96.7% were NYHA class I/II.
Conclusions: The MitraClip® procedure resulted in clinically meaningful improvements in MR severity, function and quality of life measures, and low MAE rates. These early results suggest the transferability of this therapy to appropriately selected Japanese patients. (Trial Registration: clinicaltrials.gov Identifier NCT02520310.)
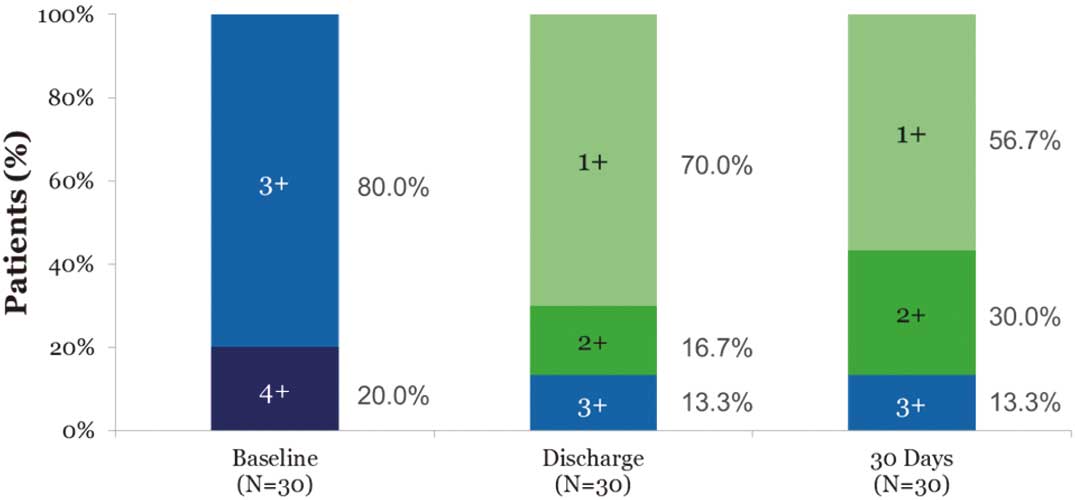
Mitral regurgitation severity grade assessed by echocardiography core laboratory at baseline, discharge, and 30 days.
(Circ J 2017; 81: 227–234)3
| Empagliflozin and Cardiovascular Outcomes in Asian Patients With Type 2 Diabetes and Established Cardiovascular Disease ― Results From EMPA-REG OUTCOME® ― Kohei Kaku, Jisoo Lee, Michaela Mattheus, Stefan Kaspers, Jyothis George, Hans-Juergen Woerle on behalf of the EMPA-REG OUTCOME® Investigators (Department of General Internal Medicine, Kawasaki Medical School, Kurashiki (K.K.), Japan; Boehringer Ingelheim Pharma GmbH & Co. KG, Ingelheim (J.L., M.M., S.K., H.-J.W.), Germany; and Boehringer Ingelheim Ltd, Bracknell, Berkshire (J.G.), UK) |
 |
Background: In the EMPA-REG OUTCOME® trial, empagliflozin added to standard of care reduced the risk of 3-point major adverse cardiovascular (CV) events (3-point MACE: composite of CV death, non-fatal myocardial infarction, or non-fatal stroke) by 14%, CV death by 38%, hospitalization for heart failure by 35%, and all-cause mortality by 32% in patients with type 2 diabetes (T2DM) and established CV disease. We investigated the effects of empagliflozin in patients of Asian race.
Methods and Results: Patients were randomized to receive empagliflozin 10 mg, empagliflozin 25 mg, or placebo. Of 7,020 patients treated, 1,517 (21.6%) were of Asian race. The reduction in 3-point MACE in Asian patients was consistent with the overall population: 3-point MACE occurred in 79/1,006 patients (7.9%) in the pooled empagliflozin group vs. 58/511 patients (11.4%) in the placebo group (hazard ratio: 0.68 [95% confidence interval: 0.48–0.95], P-value for treatment by race interaction (Asian, White, Black/African-American): 0.0872). The effects of empagliflozin on the components of MACE, all-cause mortality, and heart failure outcomes in Asian patients were consistent with the overall population (P-values for interaction by race >0.05). The adverse event profile of empagliflozin in Asian patients was similar to the overall trial population.
Conclusions: Reductions in the risk of CV outcomes and mortality with empagliflozin in Asian patients with T2DM and established CV disease were consistent with the overall trial population.

(A) Cumulative incidence of 3-point MACE (CV death, non-fatal myocardial infarction, or non-fatal stroke), (B) cumulative incidence of CV death, and (C) Kaplan-Meier estimate for all-cause mortality in Asian patients. Hazard ratios are based on Cox regression analyses in patients treated with ≥1 dose of study drug. HR, hazard ratio; other abbreviations as in Figure 1.
(Circ J 2017; 81: 1580–1588)4
| Development of a Basic Risk Score for Incident Atrial Fibrillation in a Japanese General Population ― The Suita Study ― Yoshihiro Kokubo, Makoto Watanabe, Aya Higashiyama, Yoko M Nakao, Kengo Kusano, Yoshihiro Miyamoto (Department of Preventive Medicine (Y.K., M.W., Y.M.), Department of Preventive Medicine and Epidemiologic Informatics (A.H., Y.M.N., Y.M.), Department of Cardiovascular Medicine (K.K.), National Cerebral and Cardiovascular Center, Suita, Japan) |
 |
Background: An atrial fibrillation (AF) risk score for a non-Western general population has not been established.
Methods and Results: A total of 6,898 participants (30–79 years old) initially free of AF have been prospectively followed for incident AF since 1989. AF was diagnosed when AF or atrial flutter was present on ECG at a biannual health examination; was indicated as a current illness; or was in the medical records during follow-up. Cox proportional hazard ratios were analyzed after adjusting for cardiovascular risk factors at baseline. During the 95,180 person-years of follow-up, 311 incident AF events occurred. We developed a scoring system for each risk factor as follows: 0/−5, 3/0, 7/5, and 9/9 points for men/women in their 30 s–40 s, 50 s, 60 s, and 70 s, respectively; 2 points for systolic hypertension, overweight, excessive drinking, or coronary artery disease; 1 point for current smoking; −1 point for moderate non-high-density lipoprotein-cholesterol; 4 points for arrhythmia; and 8, 6, and 2 points for subjects with cardiac murmur in their 30 s–40 s, 50 s, and 60 s, respectively (C-statistic 0.749; 95% confidence interval, 0.724−0.774). Individuals with score ≤2, 10–11, or ≥16 points had, respectively, ≤1%, 9%, and 27% observed probability of developing AF in 10 years.
Conclusions: We developed a 10-year risk score for incident AF using traditional risk factors that are easily obtained in routine outpatient clinics/health examinations without ECG.

The 10-year risk of incident atrial fibrillation (AF) based on traditional risk factors, including age, sex, cardiac murmur, and the 2 axes of “Lifestyle and Lipids” and “Cardiovascular Risks”. The Lifestyle and Lipids axis consists of excessive drinking (2 points), current smoking (1 point), and moderate non-high-density lipoprotein-cholesterol (−1 point). The Cardiovascular Risks axis consists of arrhythmia other than AF (4 points) and systolic hypertension, overweight, and coronary artery disease (2 points each). The value shown in each colored square is the percentage of incident AF within 10 years.
(Circ J 2017; 81: 1014–1021)5
| Identification and Assessment of Cardiac Amyloidosis by Myocardial Strain Analysis of Cardiac Magnetic Resonance Imaging Seitaro Oda, Daisuke Utsunomiya, Takeshi Nakaura, Hideaki Yuki, Masafumi Kidoh, Kosuke Morita, Seiji Takashio, Megumi Yamamuro, Yasuhiro Izumiya, Kyoko Hirakawa, Toshifumi Ishida, Kenichi Tsujita, Mitsuharu Ueda, Taro Yamashita, Yukio Ando, Hiroyuki Hata, Yasuyuki Yamashita (Department of Diagnostic Radiology (S.O., D.U., T.N., H.Y., M.K., Y.Y.), Department of Cardiology (S.T., M.Y., Y.I., K.H., T.I., K.T.), Department of Neurology (M.U., T.Y., Y.A.), Department of Informative Clinical Sciences (H.H.), Faculty of Life Sciences, Kumamoto University, Kumamoto; Department of Central Radiology, Kumamoto University Hospital, Kumamoto (K.M.), Japan) |
 |
Background: We explored the usefulness of myocardial strain analysis on cardiac magnetic resonance imaging (CMR) scans for the identification of cardiac amyloidosis.
Methods and Results: The 61 patients with systemic amyloidosis underwent 3.0-T CMR, including CMR tagging and late-gadolinium enhanced (LGE) imaging. The circumferential strain (CS) of LGE-positive and LGE-negative patients was measured on midventricular short-axis images and compared. Logistic regression modeling of CMR parameters was performed to detect patients with LGE-positive cardiac amyloidosis. Of the 61 patients with systemic amyloidosis 48 were LGE-positive and 13 were LGE-negative. The peak CS was significantly lower in the LGE-positive than in the LGE-negative patients (−9.5±2.3 vs. −13.3±1.4%, P<0.01). The variability in the peak CS time was significantly greater in the LGE-positive than in the LGE-negative patients (46.1±24.5 vs. 21.2±20.1 ms, P<0.01). The peak CS significantly correlated with clinical biomarkers. The sensitivity, specificity, and accuracy of the diagnostic model using CS parameters for the identification of LGE-positive amyloidosis were 93.8%, 76.9%, and 90.2%, respectively.
Conclusions: Myocardial strain analysis by CMR helped detect LGE-positive amyloidosis without the need for contrast medium. The peak CS and variability in the peak CS time may correlate with the severity of cardiac amyloid deposition and may be more sensitive than LGE imaging for the detection of early cardiac disease in patients with amyloidosis.
| Explanatory variable | OR | 95% CI | P value |
|---|---|---|---|
| Clinical model | |||
| Age | 1.08 | 1.01–1.16 | 0.02 |
| E/e’ ratio | 1.39 | 1.08–1.79 | 0.01 |
| CMR model | |||
| Mean peak CS (per %) | 3.57 | 1.57–8.10 | <0.01 |
| Variability in peak CS time (per ms) | 1.48 | 1.10–1.98 | <0.01 |
| Combined model | |||
| E/e’ ratio | 1.30 | 0.98–1.74 | 0.04 |
| Mean peak CS (per %) | 3.81 | 1.41–10.26 | <0.01 |
| Variability in peak CS time (per ms) | 1.32 | 0.97–1.80 | 0.04 |
CI, confidence interval; OR, odds ratio. Other abbreviations as in Tables 1,2,4.
(Circ J 2017; 81: 110–118)6
| Transcriptional Analysis of Intravenous Immunoglobulin Resistance in Kawasaki Disease Using an Induced Pluripotent Stem Cell Disease Model Kazuyuki Ikeda, Yasutaka Mizoro, Tomonaga Ameku, Yui Nomiya, Shin-Ichi Mae, Satoshi Matsui, Yuki Kuchitsu, Chinatsu Suzuki, Akiko Hamaoka- Okamoto, Tomoyo Yahata, Masakatsu Sone, Keisuke Okita, Akira Watanabe, Kenji Osafune, Kenji Hamaoka (Department of Pediatric Cardiology and Nephrology, Graduate School of Medical Science, Kyoto Prefectural University of Medicine, Kyoto (K.I., Y.K., C.S., A.H.-O., T.Y., K.H.); Center for iPS Cell Research and Application (CiRA) (K.I., Y.M., T.A., Y.N., S. Mae, S. Matsui, K. Okita, A.W., K. Osafune), Institute for Integrated Cell-Material Sciences (iCeMS) (Y.M., A.W.), Kyoto University, Kyoto; and Department of Metabolic Medicine, Department of Diabetes, Endocrinology and Nutrition, Kyoto University Graduate School of Medicine, Kyoto (M.S.), Japan) |
 |
Background: Approximately 10–20% of Kawasaki disease (KD) patients are resistant to intravenous immunoglobulin (IVIG) treatment. Further, these patients are at a particularly high risk of having coronary artery abnormalities. The mechanisms of IVIG resistance in KD have been analyzed using patient leukocytes, but not patient vascular endothelial cells (ECs). The present study clarifies the mechanisms of IVIG resistance in KD using an induced pluripotent stem cell (iPSC) disease model.
Methods and Results: Dermal fibroblasts or peripheral blood mononuclear cells from 2 IVIG-resistant and 2 IVIG-responsive KD patients were reprogrammed by the episomal vector-mediated transduction of 6 reprogramming factors. KD patient-derived iPSCs were differentiated into ECs (iPSC-ECs). The gene expression profiles of iPSC-ECs generated from IVIG-resistant and IVIG-responsive KD patients were compared by RNA-sequencing analyses. We found that the expression of CXCL12 was significantly upregulated in iPSC-ECs from IVIG-resistant KD patients. Additionally, Gene Set Enrichment Analysis (GSEA) revealed that gene sets involved in interleukin (IL)-6 signaling were also upregulated.
Conclusions: The first iPSC-based model for KD is reported here. Our mechanistic analyses suggest that CXCL12, which plays a role in leukocyte transmigration, is a key molecule candidate for IVIG resistance and KD severity. They also indicate that an upregulation of IL-6-related genes may be involved in this pathogenesis.

Gene set enrichment analysis (GSEA) of endothelial cells (ECs) differentiated from induced pluripotent stem cells (iPSCs) from a patient with Kawasaki disease (KD-iPSCs). (A) GSEA using RNA-sequencing data of iPSC-ECs derived from intravenous immunoglobulin (IVIG)-responder KD patients and IVIG-non-responder KD patients. A larger number of black lines are found at the left side of the panel, indicating that the expression levels of interleukin (IL)-6 related genes are higher in the IVIG non-responder group than in the IVIG responder group. (B) The expression levels of a (a) breast cancer-related gene set; (b) NRAS (a member of the RAS oncogene family) related gene set; and (c) cervical carcinoma related gene set are also higher in the IVIG non-responder group.
(Circ J 2017; 81: 1862–1870)7
| Differential Effects of Myocardial Afadin on Pressure Overload-Induced Compensated Cardiac Hypertrophy Dimitar P. Zankov, Akira Sato, Akio Shimizu, Hisakazu Ogita (Division of Molecular Medical Biochemistry, Department of Biochemistry and Molecular Biology, Shiga University of Medical Science, Otsu, Japan) |
 |
Background: Pressure overload induces cardiac hypertrophy, which often ends in heart failure. Afadin is an adaptor protein that is ubiquitously expressed and, in the heart, it localizes at intercalated disks. The current study aimed to examine the afadin-mediated cardiac phenotype in mice exposed to different types of pressure overload: transverse aortic constriction (TAC) burden and angiotensin II (Ang II) stimulation.
Methods and Results: Conditional knockout mice with selective deletion of afadin (afadin cKO) in cardiomyocytes were generated. TAC-operated and Ang II-infused mice at 4 weeks had a similar degree of pressure overload and cardiac hypertrophy in the heart. In afadin cKO mice, TAC operation caused progressive left ventricular dysfunction and heart failure, while Ang II infusion did not deteriorate cardiac function. Furthermore, TAC operation produced more fibrosis and apoptosis in the heart than Ang II infusion, and the expression of growth differentiation factor 15, which can promote apoptosis, in the afadin cKO heart was higher in TAC-operated mice than Ang II-infused ones.
Conclusions: In the 2 pressure overload models, myocardial afadin is involved in mechanical stress-induced, but not pharmacological Ang II-related, compensated cardiac hypertrophy.

Morphometry of the hearts and lungs after a 4-week transverse aortic constriction (TAC) burden or angiotensin II (Ang II) infusion. (A) Typical images of hearts exposed to sham operation, TAC burden or Ang II infusion. Heart weight is indicated in each image. (B) Summary graphs of normalized heart weight (heart weight to tibia length ratio). (C) Summary graphs of normalized lung weight (lung weight to tibia length ratio). In (B) and (C), n=3–4 per group. Control: afadin-floxed mice. *P<0.05.
(Circ J 2017; 81: 158–164)8
| Clinical Significance of Hematuria in Atrial Fibrillation With Oral Anticoagulation Therapy Hee Tae Yu, Tae-Hoon Kim, Jae-Sun Uhm, Jong-Youn Kim, Hui-Nam Pak, Moon-Hyoung Lee, Boyoung Joung (Division of Cardiology, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea) |
 |
Background: Hematuria is a common and important complication in atrial fibrillation (AF) patients on oral anticoagulation therapy (OAT). This study evaluated the clinical significance of hematuria and its relationship with genitourinary disease in AF patients receiving OAT.
Methods and Results: Among 20,456 consecutive AF patients who visited a tertiary hospital from January 2005 to April 2015, 5,833 had hematuria. Of these 5,833 patients, 3,798 were on OAT (OAT(+) group) and 2,035 were not (OAT(−) group). A total of 1,785 patients from each group were then matched on propensity score analysis. The prevalence of cancer and other diseases in the genitourinary tract was evaluated. While there was no difference in the prevalence of genitourinary stones or urinary tract infection, genitourinary cancer was significantly more common in the OAT(+) group than in the OAT(−) group (1.6% vs. 0.7%, P=0.011). Bladder cancer was the most common genitourinary malignancy, and it was significantly more common in the OAT(+) group (1.2% vs. 0.5%, P=0.019). Subjects on warfarin were more likely to have bladder cancers of lower pathologic grade (63.6% vs. 33.3%, P=0.124).
Conclusions: OAT was associated with a higher prevalence and early detection of genitourinary cancer in AF patients with hematuria. Meticulous evaluation of the cause of hematuria is necessary in AF patients with hematuria receiving OAT.

Location of genitourinary (GU) cancer in hematuria patients in (A) the total and (B) propensity score-matched oral anticoagulation therapy (OAT)(+) and OAT(−) groups.
Awards will be presented to the 8 research groups during the 82nd Annual Scientific Meeting of the Japanese Circulation Society, and will also be announced on the Society website. We look forward to receiving manuscripts with high scientific impact for publication in Circulation Journal in 2018.