Abstract
Cardiac rehabilitation (CR) is a well-known intervention for the secondary prevention of cardiovascular diseases. However, in Japan, the outpatient CR participation rate is estimated to be very low. Cardiac telerehabilitation (CTR) can be defined as a remote CR program using digital health technology to support it. Evidence regarding the use of CTR has been accumulated, and the COVID-19 pandemic has accelerated the need for CTR. Japan has sufficient potential to benefit from CTR because, nationally, digital literacy is high and the infrastructure for telemedicine is developed. To overcome several barriers, evidence of CTR in Japan, well-educated multidisciplinary CTR teams, a good combination of center-based CR and CTR, and sophisticated systems including social insurance and adequate legislation need to be developed immediately. CTR has the potential to increase the low CR participation rate in Japan. CTR also has many different effects that not only cardiologists, but also paramedics who engage in CTR, have to be aware of.
Cardiac Rehabilitation (CR)
Importance of CR
CR is a well-known multidisciplinary intervention for the secondary prevention of coronary artery disease (CAD), heart failure (HF), and other cardiac diseases.1
In addition to exercise advice and guideline-based exercise prescription, CR consists of dietary guidance, psychosocial management, therapy adherence, control of cardiovascular risk factors, and occupational support.2
CR has substantial effects on reducing the risks of hospitalization and cardiovascular mortality in CAD patients.3
CR probably reduces all-cause hospital admissions and may reduce HF-specific hospital admissions,4
and the Japanese Circulation Society (JCS) statement for HF in 2019 also noted the effects of CR.5
Moreover, in addition to improving patients’ quality of life, CR is a cost-effective treatment.3
These benefits of CR have been noted in international guidelines.1,6
In Japan, the 2021 JCS/Japanese Association of Cardiac Rehabilitation (JACR) guideline confirmed the importance of CR for secondary prevention of CAD and chronic HF.7
Underuse of Outpatient CR in Japan
The outpatient CR participation rate is generally low (30–50% in Europe;8
19–34% in the US9). In Japan, although 150 days CR is covered by medical insurance for patients with cardiovascular disease (CVD), recent outpatient CR participation rates for HF, ACS, and stable CAD patients were 7%, 9%, and 3%, respectively, which are extremely low.10,11
There are several explanations for the low CR participation rates in Japan. First, the number of institutions equipped to provide outpatient CR is not sufficient. According to 2009 data,12
only 21% of all facilities in Japan in which cardiologists perform coronary interventions have outpatient CR centers. Second, the social awareness of CR is low. In Japan, CR participation rates are significantly lower than participation rates for cerebrovascular or orthopedic rehabilitation, and the low level of CR awareness applies to both patients and medical professionals.13
Third, geographically, Japan is country with a lot of inhabited islands and steep mountains. Transportation to and from larger cities, as well as physical cardiology follow-up in rural areas, are sometimes limited.
Cardiac Telerehabilitation (CTR)
Effects of Using CTR and CR Teams
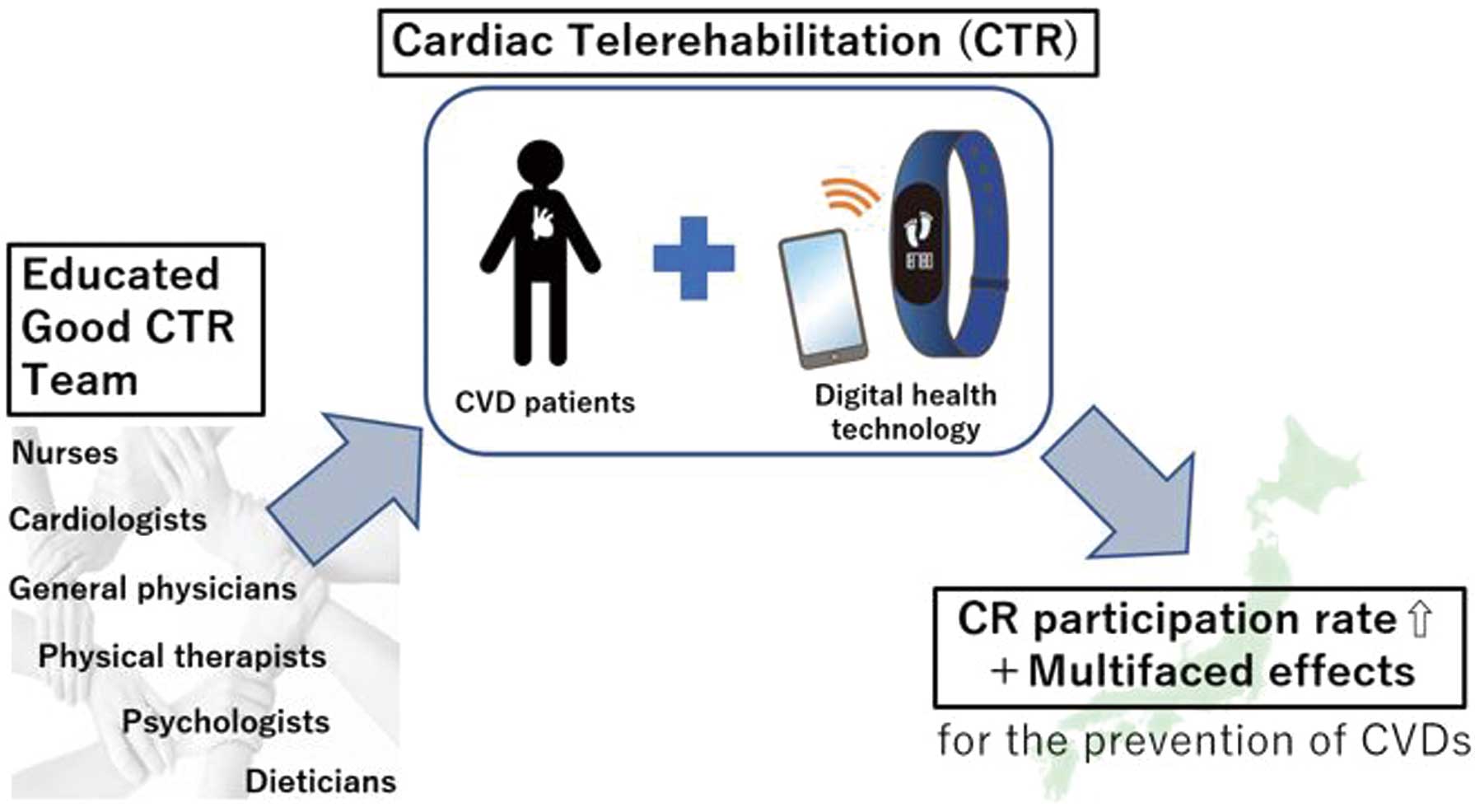
CTR can be defined as a remote CR program that makes use of digital health technology, such as monitoring devices, to support the program. CTR enables interactions with cardiac patients outside the hospital. A recent review reported measures for the future distribution of CTR in the US and indicated that CTR has multiple effects and may be a good option for stable low- to moderate-risk CVD patients.14
Another review, in Europe, also indicated that CTR has multiple effects and that he current COVID-19 pandemic has accelerated the need for CTR.15
Furthermore, the need for CTR will be accelerated by cost considerations with regard to CAD and HF.16
CTR is a solution for geographical barriers that mean patients cannot easily reach CR centers in their local hospitals. A previous systematic review concluded that CTR is superior to usual CR in reducing hospitalizations and improving adherence to physical activity guidelines.17
CTR may induce long-term exercise effects for CAD patients.18
Regarding HF, CTR could reduce both the time lost owing to unplanned cardiovascular hospital admissions and all-cause mortality.19
Theoretically, CTR has a greater potential of maintaining a lifelong effect than center-based CR, which is an important consideration. Furthermore, an automatic CR referral strategy could achieve a higher CR enrollment rate.20
The aim of the recent European Union-funded CoroPrevention project (https://coroprevention.eu/ [accessed May 11, 2021]) was to develop digital solutions to make personalized and sustainable interventions possible, as well as to monitor and motivate patients as part of the overall CR process. Specifically, the CoroPrevention methodology includes decision support systems for case nurses and doctors, shared decision making (SDM) during encounters, an electronic tablet and mobile application for patients, and a caregiver dashboard to facilitate SDM with caregivers and patients. The systems allow the registration and follow-up of patients’ data lifelong and the use of these data to support healthy lifestyles.
A multidisciplinary team, including cardiologists, healthcare workers, and general physicians, will still be needed for CTR. Most importantly, CTR is an information and communication technology (ICT)-facilitated solution, not a treatment in itself. Patients undergoing CTR still need good CR centers for their follow-up. If the medical staff involved in a patient’s treatment are not located the same place, ICT can also strengthen the relationships with the “CTR team”. The implementation of training for multidisciplinary teams can be based on the new core curriculum for preventive cardiology.21
Characteristic Circumstances in Japan Relevant to CTR
As of 2019, Japan has the longest average life expectancy in the world.22
Nevertheless, in Organisation for Economic Co-operation and Development countries, individuals aged 16–65 years have the highest levels of digital literacy and numeracy skills.23
Thus, Japan has good potential for digital transformation. When the population ages further and home health care may become the mainstay, CTR has considerable potential to be implemented in Japan. In Japan, legislation enacted in the 1990 s means that CR is not permitted in convalescent hospitals. This needs to be revised in line with the dissemination of CTR. Outside of large cities like Tokyo, there are only a few institutes providing CR in each prefecture in Japan. Thus, it is unrealistic for patients to perform CR a several times a week.24
However, under such circumstances, CTR can be done at any time, if it is well organized. Moreover, the concept of “hybrid CR” may be suitable, in which patients start with short-term center-based CR that is followed by a long-term CTR.25
This system does not lose the knowledge of the existing CR teams and can treat and follow-up more patients by CTR.26
In this “hybrid CR” system, an important concept is that of “hub facilities”, which serve as coordinating centers for local medical staff. For example, it may be difficult to locate educated dietitians or psychologists across all districts in Japan; however, ICT could facilitate patient education by these paramedics, who could be located in a “hub facility”.
Barriers to CTR Implementation in Japan and How to Overcome Them
Although CTR is an attractive solution for Japan, there are many barriers regarding knowledge acquisition of CTR for both patients and medical professionals, reimbursement for CTR, technical considerations, and legal and ethical issues, among others.27
CTR team members who follow-up patients and collect and process data need to be trained, and may need to become digitally literate if they are not familiar with the technology used and management processes. In particular, good trust relationships between nurses, patients, and their families are crucial for CTR to be adopted by the Japanese community. Cardiologists consulted by general physicians about patients’ physical activity needs must be appropriately trained in CTR. Because general physicians, in addition to cardiologists, can recommend CTR to patients in primary health care, information sessions with general physicians (or cardiologists) and patients in the community are required. If these relationships work well, and doctors or nurses can use the data to follow-up with patients who drop out of their CTR program, the CTR participation rate could be improved.
Reimbursement for CTR is a big problem in Japan, as well as in Europe and the US. However, a previous review found that CTR is associated with similar or lower long-term costs as center-based CR with equal or superior clinical impacts.16
Currently, CTR is not covered by insurance in Japan, and at this stage evidence is being accumulated regarding CTR. There have been some studies published on remote CR programs28
or an Internet of things-equipped ergometer.29
Another study, registered with the University Hospital Medical Information Network (UMIN) Clinical Trials Registry (ID: UMIN000042942), will use an ergometer with home-based real-time remote monitoring system to evaluate the effects of remote CR. The JACR is lobbying for CTR reimbursement and this, with evidence of the long-term cost-effectiveness of CTR, could promote its use in Japan.
In addition, the validation of devices used as part of CTR remains an issue. Evidence of the safety and trustworthiness of programs with devices needs to be accumulated, and the liability of medical professionals who monitor the tremendous amounts of data generated by digital devices is another issue. Security and privacy problems are issues that will always need to be considered with a telemonitoring system. However, who has accessed what data can be clearly tracked using digital health, and the data are more secure. In 2016, the Basic Act on the Advancement of Public and Private Sector Data Utilization was enacted in Japan,30
and CTR should be expanded based on the law.
Why Could CTR Be the Future Approach for Japan?
CTR has many different effects on patients with CVDs in Japan. A recent paper published by the Ministry of Health, Labour and Welfare in Japan stated a basic plan for measures against CVD to extend healthy life expectancy and listed 10 points for “enhancing service provision systems related to health, medical care, and welfare services”.31
CTR has the potential to increase the uptake of core components of CR, it can be more reasonable than building CR centers across the entire country, and it can reduce recurrent CVD events and mortality. These effects address some of the 10 points in the paper from the Ministry of Health, Labour and Welfare.31
CTR needs to be expanded because otherwise many patients would not participate in CR. Furthermore, accumulated CTR data in digital devices can be used to optimize secondary prevention in Japan. To achieve this goal, cardiologists and other CTR team members will need to be trained in the core curriculum for preventive cardiology. The JACR is expected to create a Japanese version of the core curriculum, certify centers providing the ICT tools, and plead for a change in the legislation, as well as reimbursement, to increase the number of hospitals that can provide CTR in the future. Then, good CTR facilities can start to be built that follow-up patients all over Japan, without any problems, to increase the uptake of CR and to improve patient outcomes. This should be done in Japan immediately, and, in that sense, we really want to persuade every cardiologist that CTR could be the future in cardiovascular care (Figure).
Conclusions
We see CTR as a solution to improve the low CR participation rate in Japan. To this end, we need to accumulate evidence regarding the use of CTR. Attention should be paid not only to the digital technology, but also to the collaboration of a good CTR team.
Acknowledgments
The authors thank all the staff members of the laboratories at Jessa Hospital and St. Marianna University School of Medicine Hospital for their efforts and understanding of the principle in this vision document.
Disclosures
Y.J.A. is a member of
Circulation Reports’ Editorial Team. The remaining authors have no conflicts of interest to disclose.
IRB Information
Not applicable.
References
- 1.
Piepoli MF, Hoes AW, Agewall S, Albus C, Brotons C, Catapano AL, et al. 2016 European guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J 2016; 37: 2315–2381.
- 2.
Ambrosetti M, Abreu A, Corrà U, Davos CH, Hansen D, Frederix I, et al. Secondary prevention through comprehensive cardiovascular rehabilitation: From knowledge to implementation. 2020 update. A position paper from the Secondary Prevention and Rehabilitation Section of the European Association of Preventive Cardiology. Eur J Prev Cardiol, doi:10.1177/2047487320913379.
- 3.
Anderson L, Thompson D, Oldridge N, Zwisler A, Rees K, Martin N, et al. Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst Rev 2016; 1: CD001800.
- 4.
Long L, Mordi IR, Bridges C, Sagar VA, Davies EJ, Coats AJS, et al. Exercise-based cardiac rehabilitation for adults with heart failure. Cochrane Database Syst Rev 2019; 1: CD003331.doi:10.1002/14651858.CD003331.pub5.
- 5.
Izawa H, Yoshida T, Ikegame T, Izawa KP, Ito Y, Okamura H, et al. Standard cardiac rehabilitation program for heart failure. Circ J 2019; 83: 2394–2398.
- 6.
O’Gara PT, Kushner FG, Ascheim DD, Casey DE, Chung MK, De Lemos JA, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction. J Am Coll Cardiol 2013; 61: 78–140.
- 7.
The Japanese Circulation Society and the Japanese Association of Cardiac Rehabilitation. JCS/JACR 2021 guideline on rehabilitation in patients with cardiovascular disease (in Japanese). https://www.j-circ.or.jp/cms/wp-content/uploads/2021/03/JCS2021_Makita.pdf (accessed October 18, 2021).
- 8.
Humphrey R, Guazzi M, Niebauer J. Cardiac rehabilitation in Europe. Prog Cardiovasc Dis 2014; 56: 551–556.
- 9.
Ades P, Keteyian S, Wright J, Hamm L, Lui K, Newlin K, et al. Increasing cardiac rehabilitation participation from 20% to 70%: A road map from the Million Hearts Cardiac Rehabilitation Collaborative. Mayo Clin Proc 2017; 92: 234–242.
- 10.
Kamiya K, Yamamoto T, Tsuchihashi-Makaya M, Ikegame T, Takahashi T, Sato Y, et al. Nationwide survey of multidisciplinary care and cardiac rehabilitation for patients with heart failure in Japan: An analysis of the AMED-CHF study. Circ J 2019; 83: 1546–1552.
- 11.
Kanaoka K, Soeda T, Terasaki S, Nishioka Y, Myojin T, Kubo S, et al. Current status and effect of outpatient cardiac rehabilitation after percutaneous coronary intervention in Japan. Circ Rep 2021; 3: 122–130.
- 12.
Nakanishi M, Nagayama M, Adachi H, Ikeda K, Fujimoto K, Tashiro T, et al. Trends in the implementation rate of cardiac rehabilitation after acute myocardial infarction in Japan. Shinzou Rehabilitation 2011; 16: 188–192 (in Japanese).
- 13.
The Japanese Association of Cardiac Rehabilitation. JACR statement: Mission of the Japanese Association of Cardiac Rehabilitation 2013. https://www.jacr.jp/web/en/jacr-statement/ (accessed June 28, 2020).
- 14.
Thomas RJ, Beatty AL, Beckie TM, Brewer LPC, Brown TM, Forman DE, et al. Home-based cardiac rehabilitation: A scientific statement from the American Association of Cardiovascular and Pulmonary Rehabilitation, the American Heart Association, and the American College of Cardiology. Circulation 2019; 140: E69–E89.
- 15.
Scherrenberg M, Wilhelm M, Hansen D, Völler H, Cornelissen V, Frederix I, et al. The future is now: A call for action for cardiac telerehabilitation in the COVID-19 pandemic from the secondary prevention and rehabilitation section of the European Association of Preventive Cardiology. Eur J Prev Cardiol, doi:10.1177/2047487320939671.
- 16.
Scherrenberg M, Falter M, Dendale P. Cost-effectiveness of cardiac telerehabilitation in coronary artery disease and heart failure patients: Systematic review of randomized controlled trials. Eur Hear J Digit Health 2020; 1: 20–29.
- 17.
Frederix I, Vanhees L, Dendale P, Goetschalckx K. A review of telerehabilitation for cardiac patients. J Telemed Telecare 2015; 21: 45–53.
- 18.
Batalik L, Dosbaba F, Hartman M, Konecny V, Batalikova K, Spinar J. Long-term exercise effects after cardiac telerehabilitation in patients with coronary artery disease: 1-year follow-up results of the randomized study. Eur J Phys Rehabil Med 2021; 57: 807–814.
- 19.
Koehler F, Koehler K, Deckwart O, Prescher S, Wegscheider K, Kirwan BA, et al. Efficacy of telemedical interventional management in patients with heart failure (TIM-HF2): A randomised, controlled, parallel-group, unmasked trial. Lancet 2018; 392: 1047–1057.
- 20.
Grace SL, Russell KL, Reid RD, Oh P, Anand S, Rush J, et al. Effect of cardiac rehabilitation referral strategies on utilization rates: A prospective, controlled study. Arch Intern Med 2011; 171: 235–241.
- 21.
Wilhelm M, Abreu A, Adami PE, Ambrosetti M, Antonopoulou M, Biffi A, et al. EAPC core curriculum for preventive cardiology [published erratum appears in Eur J Prev Cardiol, doi:10.1093/eurjpc/zwab071]. Eur J Prev Cardiol, doi:10.1093/eurjpc/zwab017.
- 22.
Ministry of Health Labour and Welfare in Japan. International comparison of life expectancy (in Japanese). https://www.mhlw.go.jp/toukei/saikin/hw/life/life19/dl/life19-04.pdf (accessed April 23, 2021).
- 23.
Organisation for Economic Co-operation and Development (OECD). OECD skills outlook 2019. Learning for life. Country profile: Japan. https://www.oecd.org/japan/Skills-Outlook-Japan-EN.pdf (accessed April 23, 2021).
- 24.
Kusunoki S, Maruji A, Kobayashi K, Hirao N, Konishi H, Fukui N, et al. Subjective barriers to adherence to cardiac rehabilitation program after hospital discharge in patients with acute myocardial infarction. Nihon Kan Shikkan Gakkai Zasshi 2008; 14: 206–210 (in Japanese).
- 25.
Gouda A, Itoh H, Tajima A, Meda T, Yamaguchi K, Nagayama O, et al. Hybrid home-based exercise therapy for patients with chronic heart failure. Shinzou Rehabilitation 2006; 11: 67–69 (in Japanese).
- 26.
The Japanese Circulation Society and The Japan Stroke Society. The second five-year plan to overcome stroke and cardiovascular disease (in Japanese). https://www.j-circ.or.jp/cms/wp-content/uploads/2021/06/JCS_five_year_plan_2nd_20210622.pdf (accessed June 26, 2021)
- 27.
Frederix I, Caiani EG, Dendale P, Anker S, Bax J, Böhm A, et al. ESC e-Cardiology Working Group position paper: Overcoming challenges in digital health implementation in cardiovascular medicine. Eur J Prev Cardiol 2019; 26: 1166–1177.
- 28.
Nakayama A, Takayama N, Kobayashi M, Hyodo K, Maeshima N, Takayuki F, et al. Remote cardiac rehabilitation is a good alternative of outpatient cardiac rehabilitation in the COVID-19 era. Environ Health Prev Med 2020; 25: 4–9.
- 29.
Kikuchi A, Taniguchi T, Nakamoto K, Sera F, Ohtani T, Yamada T, et al. Feasibility of home-based cardiac rehabilitation using an integrated telerehabilitation platform in elderly patients with heart failure: A pilot study. J Cardiol 2021; 78: 66–71.
- 30.
Prime Minister’s Office of Japan. Declaration to Be the World’s Most Advanced IT Nation Basic Plan for the Advancement of Public and Private Sector Data Utilization. 2016. https://japan.kantei.go.jp/policy/it/2017/20170530_full.pdf (accessed April 27, 2021).
- 31.
Kuwabara M, Mori M, Komoto S. Japanese national plan for promotion of measures against cerebrovascular and cardiovascular disease. Circulation 2021; 143: 1929–1931.
