Abstract
Background: Genetic testing for cardiovascular diseases (CVD) is vital, but is underutilized in Japan due to limited insurance coverage, accessibility, and public disinterest. This study explores demographic factors influencing the decision to undergo CVD genetic testing.
Methods and Results: We compared the CVD history and baseline demographics of Japanese adults who underwent genetic testing with those who did not, using an Internet survey. The regression model indicated that men, the young, married individuals, parents, and those with CVD, higher score for rationality, and lower quality of life were more inclined to undergo testing.
Conclusions: Targeting strategies for CVD genetic testing could focus on these demographics.
Genetic testing, a rapidly evolving area of research within the broader medical field, has markedly advanced the management of inherited cardiovascular diseases (CVD) by improving diagnostic capabilities and facilitating risk stratification and provision of tailored, individualized treatments.1 Although expanded availability of genetic testing has been instrumental in identifying genetic variants in 20–35% of patients previously diagnosed with idiopathic dilated cardiomyopathy, it remains notably underutilized, as only 1–2% of patients with inherited CVD undergo such testing.2–4
This underutilization can be attributed to various barriers affecting both recipients and providers. Recipients grapple with issues such as anxiety, fear, and disinterest, including concerns about test outcomes and the implications of low-risk results.5 Providers face challenges from inadequate knowledge, lack of testing experience, skepticism regarding test utility, and concerns about triggering unnecessary subsequent tests.6 Moreover, fundamental demographic factors, including age, sex, education level, and income, have been recognized as having a significant role in shaping general acceptance of genetic testing.7 However, these findings predominantly focus on genetic diseases overall, with limited exploration of specific conditions such as CVD.
In Japan, integrating genetic testing for CVD into clinical practice has unique challenges. First, limited insurance coverage significantly hampers its adoption; for example, hypertrophic cardiomyopathy was only added to insurance coverage in 2022. Furthermore, availability of such testing is confined to university hospitals, and it is still predominantly in the research phase. In fact, only about 10 university hospital facilities across the country currently conduct genetic analyses for primary cardiomyopathy.7 This situation is likely exacerbated not only by a general lack of interest in genetic testing among the broader population but also among patients with CVD, indicating widespread ambivalence towards this diagnostic tool even among those directly affected by these conditions.
Recognizing these complexities, our study focused on identifying basic patient-side factors affecting the decision to undergo genetic testing for CVD in Japan. This foundational pilot research is essential for addressing the significant knowledge gap, particularly regarding demographic determinants and their role in the acceptance and implementation of genetic testing.
Methods
Study Design and Population
A cross-sectional, anonymous, self-administered online survey was conducted targeting Japanese citizens aged ≥20 years in October 2023. Following the recruitment protocol detailed below, a total of 15,000 individuals were recruited from among 13 million voluntarily registered participants at a web-based Internet survey company (Freeasy; iBRIDGE Company, Tokyo, Japan). The questionnaire was disseminated via Freeasy’s online platform. An invitation email containing the survey link was sent to all applicable registrants in the original database simultaneously. We applied filters based on the demographic distribution of prefectures and the sex ratio to ensure a representative sample of the population. Before participation, the respondents familiarized themselves with the privacy policies of the study. They were informed that they would be considered willing to participate if they chose to complete and submit the survey.8 We initiated the online survey on October 23, 2023, and upon receiving 15,000 responses, we closed the survey on October 24, 2023.
Questionnaire
Our survey was designed to compare background factors between individuals who had undergone genetic testing for CVD and those who had not. It included queries on cardiovascular history, CVD genetic testing experience at a medical facility or through direct-to-consumer survices, Kemp Quality of Life Scale;9 1 question designed to assess the overall quality of life (QOL) of the individual, taking into consideration various aspects of life on a 1–7 scale, the Rational-Experiential Inventory-10 (REI-10);10 a set of 10 questions that comprised a psychological assessment tool used to measure 2 different styles of cognition: rational (analytical, logical reasoning) and experiential (intuitive, emotion-based decision-making); as well as demographic details (age, sex, marital status, parental status, and occupation). The specific content of the questionnaire comprising 4 questions is shown in Table 1. For the purposes of our survey, CVD was defined as heart failure, cardiomyopathy, angina pectoris, myocardial infarction, arrhythmia, valvular heart disease, congenital heart disease, transient cerebral ischemic attacks, cerebral infarction, cerebral hemorrhage, subarachnoid hemorrhage, peripheral vascular disease, and pulmonary thromboembolism. In this study, CVD was categorized as congestive heart failure, cardiomyopathy, arrhythmia, and other CVDs.
Table 1.
Questionnaire on Demographic Factors, Cardiovascular Disease History, and Genetic Testing
| 1. Do you have any of the following cardiovascular diseases? Please select all that apply. |
| • Heart failure |
| • Cardiomyopathy |
| • Angina |
| • Myocardial infarction |
| • Arrhythmia |
| • Valvular heart disease |
| • Congenital heart disease |
| • Ischemic stroke (cerebral infarction) |
| • Hemorrhagic stroke (cerebral hemorrhage, subarachnoid hemorrhage) |
| • Transient ischemic attack |
| • Peripheral vascular disease (e.g., obstructive arteriosclerosis, chronic limb ischemia) |
| • Pulmonary thromboembolism |
| • Aortic disease (e.g., aortic dissection, aortic aneurysm) |
| • Pulmonary hypertension |
| • Hypertension (not a cardiovascular disease itself, but please indicate if you have hypertension) |
| • Cancer (not directly related to cardiovascular disease, but please check if you have been diagnosed with any type of cancer) |
| • Other |
| • None of the above |
| 2. Have you ever undergone genetic testing related to cardiovascular disease? |
| • I have undergone genetic testing for cardiovascular disease at a medical facility. |
| • I have undergone direct-to-consumer genetic testing for cardiovascular disease, or testing that I could do myself. |
| • I have undergone genetic testing but am unsure if it was related to cardiovascular disease (or it was for something else like cancer). |
| • No, I have not undergone any genetic testing. |
3. Questions about Rationality and Intuition. For each item, please choose from the following scale: 1: Completely false, 2: Mostly
false, 3: Neither true nor false, 4: Mostly true, 5: Completely true. |
| • I do not like to have to do a lot of thinking. |
| • I try to avoid situations that require thinking in depth about something. |
| • I prefer to do something that challenges my thinking abilities rather than something that requires little thought. |
| • I prefer complex to simple problem. |
| • Thinking hard and for a long time about something gives me little satisfaction. |
| • I trust my initial feelings about people. |
| • I believe in trusting my hunches. |
| • My initial impressions of people are almost always right. |
| • When it comes to trusting people, I can usually rely on my “gut feelings.” |
| • I can usually feel when a person is right or wrong even if I cannot explain how I know. |
4. Taking everything in your life into account, please rate your overall Quality of Life (QOL) on the following 7-point scale. One (1)
means life is very distressing; it is hard to imagine how it could get much worse. Seven (7) means life is great; it is hard to
imagine how it could get much better. Four (4) means life is so-so; neither good nor bad. |
| Now, where are you? Choose a number on the figure below that best describes your current overall QOL. |
| • 1 • 2 • 3 • 4 • 5 • 6 • 7 |
Statistical Analysis
The participants were divided into 2 groups: those who had undergone genetic testing for cardiovascular conditions and those who had not. We used descriptive statistics to outline respondent demographic and clinical characteristics and their survey responses, and compared the baseline demographics of the 2 groups. For categorical variables, including sex, marital status, parental status, and presence of CVD, frequencies and percentages were used. Continuous variables, such as age, rationality score, and QOL score, were summarized using median values and the 25th and 75th percentiles (interquartile range). To identify the factors associated with undergoing genetic testing for CVD, we used a logistic regression model and estimated the odds ratios (ORs) with 95% confidence intervals (CIs), considering P values <0.05 as indicative of statistical significance. We evaluated the model’s performance by calculating sensitivity, specificity, and accuracy. In addition, to address class imbalance between groups in the logistic regression model, we used the Synthetic Minority Over-sampling Technique (SMOTE) for data resampling as the robustness check. In the SMOTE algorithm, the default values in the R function ‘SMOTE()’ in the package ‘DMwR’ were used, except that the number of oversamplings was set to 100. All analyses were conducted using R software (version 4.2.3, R Foundation for Statistical Computing, Vienna, Austria).
Results
Our study encompassed a cohort of 15,000 individuals, of which 510 participants (3.4%) reported having undergone genetic testing for CVD, either at a medical facility or through direct-to-consumer services. Of the remaining participants, 13,998 (93.3%) had not received any genetic testing, and 492 participants (3.3%) underwent genetic testing for conditions other than CVD.
The characteristics of these groups are detailed in Table 2. Among those who underwent CVD genetic testing, a greater proportion were male (64.5% vs. 47.9%), and the median age was lower (42.9 years vs. 50.3 years). A history of CVD was more prevalent in the tested group, including higher rates of congestive heart failure (11.4% vs. 0.3%), cardiomyopathy (8.6% vs. 0.1%), arrhythmia (14.1% vs. 2.5%), and other CVDs (24.7% vs. 2.3%), along with a history of hypertension (22.2% vs. 11.9%) and cancer (7.8% vs. 3.4%). Additionally, this group reported higher rationality scores (15.3 vs. 14.6) and lower QOL scores (3.7 vs. 4.0).
Table 2.
Demographic Distribution of Those Who Had Undergone Genetic Testing for Cardiovascular Diseases
| Characteristic |
Undergone genetic testing |
P value |
| Yes |
No |
| No. of participants, n |
510 |
13,998 |
|
| Male, n (%) |
329 (64.5) |
6,702 (47.9) |
<0.001 |
| Age, years |
42.9 [28.3, 57.0] |
50.3 [38.0, 63.0] |
<0.001 |
| Marriage, n (%) |
296 (58.0) |
8,089 (57.8) |
0.910 |
| Child, n (%) |
273 (53.5) |
7,306 (52.2) |
0.553 |
| Healthcare provider, n (%) |
7 (1.4) |
273 (2.0) |
0.352 |
| Coexisting conditions, n (%) |
| Congestive heart failure |
58 (11.4) |
40 (0.3) |
<0.001 |
| Cardiomyopathy |
44 (8.6) |
18 (0.1) |
<0.001 |
| Arrhythmia |
72 (14.1) |
350 (2.5) |
<0.001 |
| Other cardiovascular disease |
126 (24.7) |
324 (2.3) |
<0.001 |
| Hypertension |
113 (22.2) |
1,661 (11.9) |
<0.001 |
| Cancer |
40 (7.8) |
473 (3.4) |
<0.001 |
| Rationality score |
15.3 [14.0, 17.0] |
14.6 [13.0, 16.0] |
<0.001 |
| Quality of life score |
3.7 [3.0, 4.0] |
4.0 [4.0, 5.0] |
<0.001 |
Data are n (%) or median [interquartile range].
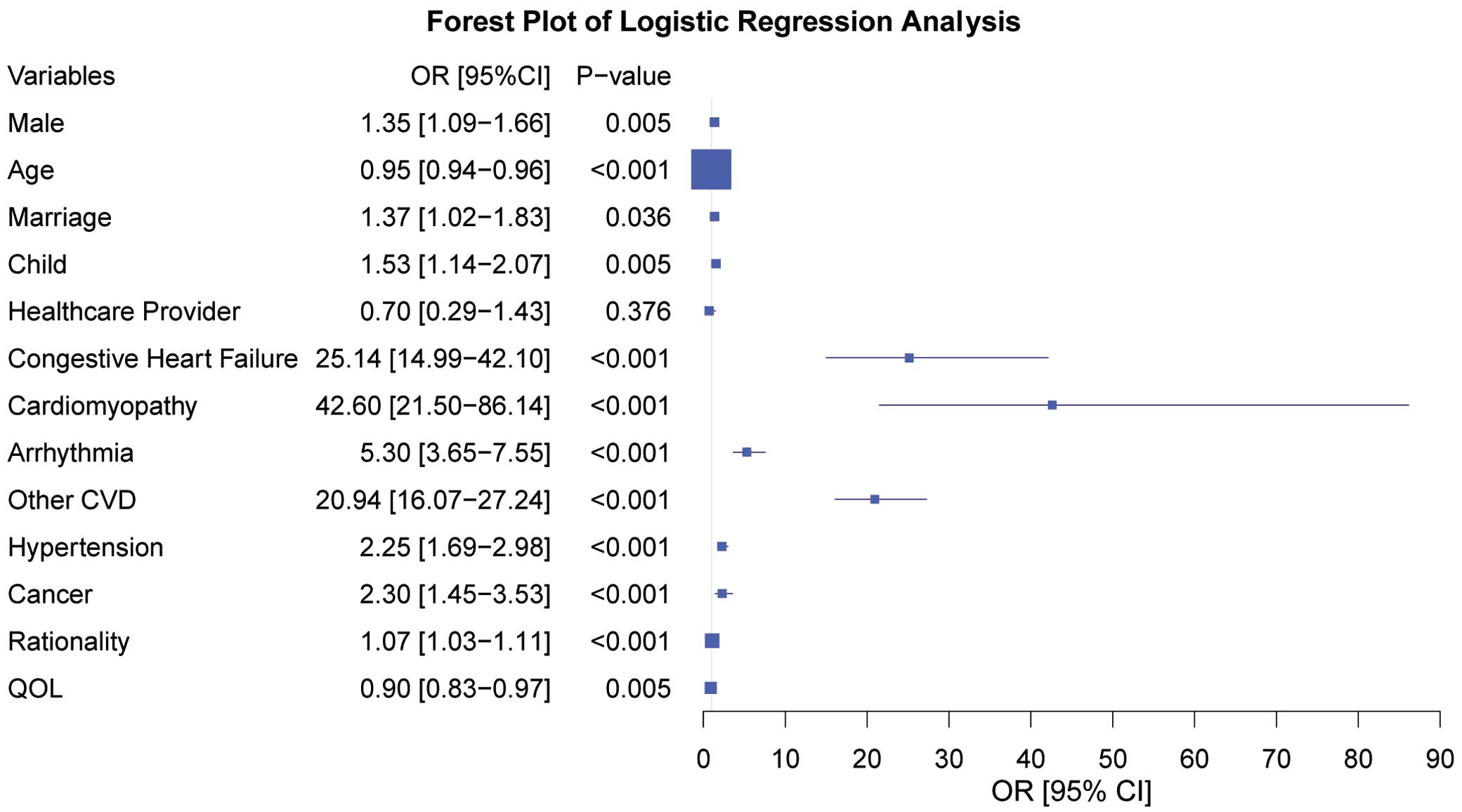
Based on the logistic regression model, we identified being male (OR=1.35 [95% CI, 1.09–1.66], P=0.005), being younger (OR=0.95 [95% CI, 0.94–0.96], P<0.001), being married (OR=1.37 [95% CI, 1.02–1.83], P=0.04), and having a child (OR=1.53 [95% CI, 1.14–2.07], P=0.005), along with having existing congestive heart failure (OR=25.10 [95% CI, 14.99–42.10], P<0.001), cardiomyopathy (OR=42.6 [95% CI, 21.50–86.14], P<0.001), arrhythmia (OR=5.30 [95% CI, 3.65–7.55], P<0.001), other CVDs (OR=20.90 [95% CI, 16.07–27.24], P<0.001), hypertension (OR=2.25 [95% CI, 1.69–2.98], P<0.001), cancer (OR=2.30 [95% CI, 1.45–3.53], P<0.001), higher rationality score (OR=1.07 [95% CI, 1.03–1.11], P<0.001), and lower QOL (1/OR=0.90 [95% CI, 0.83-0.97], P=0.005) as independent factors associated with the likelihood of undergoing genetic testing (Figure). Regarding the model’s performance, the sensitivity, specificity, and accuracy were 19.8%, 99.7%, and 96.9%, respectively. The low sensitivity is attributable to the class imbalance in the model, and thus we report the results from using SMOTE as the robustness check: the sensitivity, specificity and accuracy were 74.2% 92.4%, and 83.3%, respectively.
Discussion
This study uncovered significant demographic differences in attitudes towards genetic testing, indicating a higher propensity for genetic testing among males, younger individuals, married people, parents, and those with a personal history of CVD. The group that underwent genetic testing for CVD was characterized by higher rationality and lower QOL. Our findings provide valuable insights for developing targeted strategies for promoting genetic testing for CVD.
Our analysis indicated that several baseline demographic differences might be linked to the experience of CVD patients with genetic testing. This aligns with previous research in non-CVD populations that demonstrated a sex disparity in interest towards genetic testing,11 greater uptake among younger populations,12 and the influences of marital status and parenthood. Prior studies have suggested that married individuals often have a stronger belief in the benefits of genetic testing,13 and parents typically show a keener interest in genetic information.14 Our study also highlighted the influence of personal health history in motivating genetic testing. Individuals with a history of CVD or related conditions were found to be more inclined towards undergoing genetic testing, echoing past findings that a family history of CVD motivates both providers and recipients to consider such testing.15,16
We observed that individuals who had undergone genetic testing for CVD significantly exhibited lower QOL and higher rationality scores, suggesting a potential correlation between a patient’s health-related state and the propensity to seek genetic testing. Although Di Mattei et al explain that the effect on QOL may be associated with the perception of disease-related risk,17 others report that genetic testing results for CVD do not negatively affect QOL.18,19 It could be that individuals with lower QOL are more motivated to improve their health status, leading them to undergo genetic testing, as supported by reports suggesting that disease severity correlates with interest in genetic testing.20 Beyond health conditions, personal attributes, such as the individual’s belief systems, health literacy, and overall approach to health, may also influence the decision to undergo genetic testing. Although no previous studies have directly linked rationality to CVD genetic testing, factors such as health numeracy6 and motivation20 could be promising drivers, implying a significant role for rationality. Notably, even after adjusting for baseline background information, the correlation between QOL, rationality score, and the decision to undergo genetic testing remained significant, indicating that these factors continue to be relevant and highlighting the need for further research in this area. The robustness check using the SMOTE algorithm showed a significant improvement in sensitivity while maintaining specificity, and a slight degradation in accuracy compared with the original regression results. This finding suggests that if a researcher tries to “predict” the decision on genetic testing, the results of models using the SMOTE algorithm should be considered. However, we emphasize that given the aim of this study was not prediction but identification of some key factors contributing to the decision to undergo genetic testing, the results of the original model still play a key role despite the imbalanced sample sizes.
Study Limitations
This study, while providing valuable insights into the demographic determinants influencing the decision to undergo genetic testing for CVD in Japan, has limitations. First, the reliance on an online survey format may introduce a selection bias, as it inherently limits participation to those with Internet access and willingness to engage in such surveys. This can potentially twist the results towards a more technologically adept and younger demographic. Second, the data were based on self-reported responses, which can be subject to recall bias or subjective interpretations by the participants. Such data may not accurately represent their true health status or attitudes towards genetic testing. Additionally, the cross-sectional study design precludes establishing causal relationships or tracking changes over time, limiting our understanding of the dynamic decision-making processes regarding genetic testing. Despite these limitations, our study offers crucial insights into the current landscape of genetic testing for CVD in Japan and underscores the need for targeted strategies to enhance its adoption by specific demographic groups.
Conclusions
This study identified key factors influencing the decision to undergo genetic testing for CVD in a large cohort. Significant determinants included being male, younger, married, parent, and having CVD. These findings suggest targeted approaches for promoting genetic testing could focus on younger parents with specific health conditions to potentially improve cardiovascular health outcomes. Further research is needed to explore the impact of rationality and QOL on testing decisions.
Acknowledgment
We acknowledge the use of OpenAI’s GPT-4 in the text writing process of this manuscript.
Sources of Funding
This work was supported by grants from Japan Agency for Medical Research and Development (AMED) (JP21ek0109543) (to A.M. and S.N.).
Disclosures
The authors report no conflicts of interest.
IRB Information
This study was approved by the Institutional Review Board of St. Luke’s International Hospital in Tokyo, Japan (number: 23-R067).
Data Availability
The data generated in the study will not be shared.
References
- 1.
Cirino AL, Harris S, Lakdawala NK, Michels M, Olivotto I, Day SM, et al. Role of genetic testing in inherited cardiovascular disease: A review. JAMA Cardiol 2017; 2: 1153–1160.
- 2.
Bui QM, Ding J, Hong KN, Adler EA. The genetic evaluation of dilated cardiomyopathy. Struct Heart 2023; 7: 100200.
- 3.
Longoni M, Bhasin K, Ward A, Lee D, Nisson M, Bhatt S, et al. Real-world utilization of guideline-directed genetic testing in inherited cardiovascular diseases. Front Cardiovasc Med 2023; 10: 1272433.
- 4.
Morales A, Moretz C, Ren S, Smith E, Callis T, Dalton J, et al. Genetic testing underutilization in patients with cardiomyopathy: A real-world data analysis [Abstract]. Circulation 2021; 144: A10555.
- 5.
Shen EC, Srinivasan S, Passero LE, Allen CG, Dixon M, Foss K, et al. Barriers and facilitators for population genetic screening in healthy populations: A systematic review. Front Genet 2022; 13: 865384.
- 6.
Miyoshi T, Watanabe M. Impact of genomic literacy components on genetic testing decision-making in the general Japanese population in the 20s and 30s. PLoS One 2023; 18: e0283432.
- 7.
Kubo T, Kitaoka H. Genetic testing for cardiomyopathy in Japan 2022: Current status and issues of precision medicine. J Card Fail 2023; 29: 805–814.
- 8.
Yang F, Oshio A. A secure mind is a clear mind: The relationship between attachment security, mindfulness, and self-concept clarity. Curr Psychol 2023, doi:10.1007/s12144-023-05250-4.
- 9.
Kemp B, Ettelson D. Quality of life while living and aging with a spinal cord injury and other impairments. Top Spinal Cord Inj Rehabil 2001; 6: 116–127.
- 10.
Epstein S, Pacini R, Denes-Raj V, Heier H. Individual differences in intuitive–experiential and analytical–rational thinking styles. J Pers Soc Psychol 1996; 71: 390–405.
- 11.
Sanderson SC, Wardle J, Jarvis MJ, Humphries SE. Public interest in genetic testing for susceptibility to heart disease and cancer: A population-based survey in the UK. Prev Med (Baltimore) 2004; 39: 458–464.
- 12.
Neghina AM, Anghel A. Hereditary hemochromatosis: Awareness and genetic testing acceptability in Western Romania. Genet Test Mol Biomarkers 2010; 14: 847–850.
- 13.
Bíró K, Dombrádi V, Fekete Z, Bányai G, Boruzs K, Nagy A, et al. Investigating the knowledge of and public attitudes towards genetic testing within the Visegrad countries: A cross-sectional study. BMC Public Health 2020; 20: 1380.
- 14.
Saastamoinen A, Hyttinen V, Kortelainen M, Aaltio J, Auranen M, Ylikallio E, et al. Attitudes towards genetic testing and information: Does parenthood shape the views? J Community Genet 2020; 11: 461–473.
- 15.
Musunuru K, Hershberger RE, Day SM, Klinedinst NJ, Landstrom AP, Parikh VN, et al. Genetic testing for inherited cardiovascular diseases: A Scientific Statement from the American Heart Association. Circ Genomic Precis Med 2020; 13: e000067.
- 16.
Middlemass JB, Yazdani MF, Kai J, Standen PJ, Qureshi N. Introducing genetic testing for cardiovascular disease in primary care: A qualitative study. Br J Gen Pract 2014; 64: e282–e289.
- 17.
Di Mattei VE, Duchini E, Zucchi P, Patricelli MG, Rognone A, Di Pierro R, et al. Cancer genetic counseling and quality of life: The effect of coping strategies and psychopathological symptoms during pre-test genetic counseling. Recenti Prog Med 2015; 106: 380–384 (in Italian).
- 18.
Hickey KT, Sciacca RR, Biviano AB, Whang W, Dizon JM, Garan H, et al. The effect of cardiac genetic testing on psychological well-being and illness perceptions. Heart Lung 2014; 43: 127–132.
- 19.
Brothers C, Etchegary H, Curtis F, Simmonds C, Houston J, Young TL, et al. Psychological distress and quality of life in participants undergoing genetic testing for arrhythmogenic right ventricular cardiomyopathy caused by TMEM43 p. Public Health Genomics 2021; 24: 253–260.
- 20.
Sweeny K, Ghane A, Legg AM, Huynh HP, Andrews SE. Predictors of genetic testing decisions: A systematic review and critique of the literature. J Genet Couns 2014; 23: 263–288.
