Abstract
Objectives: Management of unstable intertrochanteric fractures is challenging, especially in patients with osteoporosis. Comminuted unstable intertrochanteric fractures require postoperative immobilization. Several recent reports have recommended hemiarthroplasty for treatment of unstable intertrochanteric fractures to avoid various immobilization-associated complications. The purpose of this study was to evaluate the functional and clinical outcomes of bipolar hemiarthroplasty for unstable intertrochanteric fractures in older persons.
Methods: Sixty patients aged over 75 years underwent hemiarthroplasty to treat unstable intertrochanteric fractures and were followed up over 12 months. All surgeries were performed by the same surgical team using the standard posterolateral approach. Wires, cables, and plates were used as required. Use of cemented protheses was considered when the lesser trochanter had been displaced. All patients were allowed full weight-bearing as tolerated. Clinical evaluation was based on Harris Hip Scores.
Results: The cohort comprised 16 men and 44 women (aged 75–96 years). According to the Jensen classification, 24 fractures were type III, 14 type IV, and 22 type V. Cement was used in 24 patients. At 12 months follow-up, Harris Hip Scores were excellent in 18%, good in 42%, fair in 25%, and poor in 15%. No radiological abnormalities were detected.
Conclusions: Primary bipolar hemiarthroplasty for treating unstable intertrochanteric fractures eliminates the need for prolonged immobilization and permits early ambulation. As reported by others, hip hemiarthroplasty is an effective treatment choice for unstable intertrochanteric femoral fracture in older patients.
Introduction
Intertrochanteric fractures comprise approximately 45%–50% of all hip fractures in older persons1 and 50%–60% of them are classified as unstable.2 Unstable intertrochanteric fractures are of major cause of concern in older patients because of the associated high morbidity and mortality.3
Intramedullary nailing is the treatment of choice for stable hip fractures. Intramedullary nailing techniques require only a small incision and protect patients’ bone structure. Intramedullary nailing reduces surgical complications, blood loss, and infection.4 Thus, the minimally invasive procedure of intramedullary nailing is considered the most appropriate for geriatric patients.
Management of unstable intertrochanteric fractures is challenging in older patients because of their poor bone quality and high risk of morbidity and mortality.5 Osteoporosis and instability are two of the most important factors leading to unsatisfactory treatment outcomes.6,7
Selection of the implant type is extremely important because it affects these patients’ survival and functional outcomes. Intramedullary nailing is also the most commonly performed procedure for unstable intertrochanteric fractures; however, a review of published reports indicates there is a lack of consensus regarding this choice.4
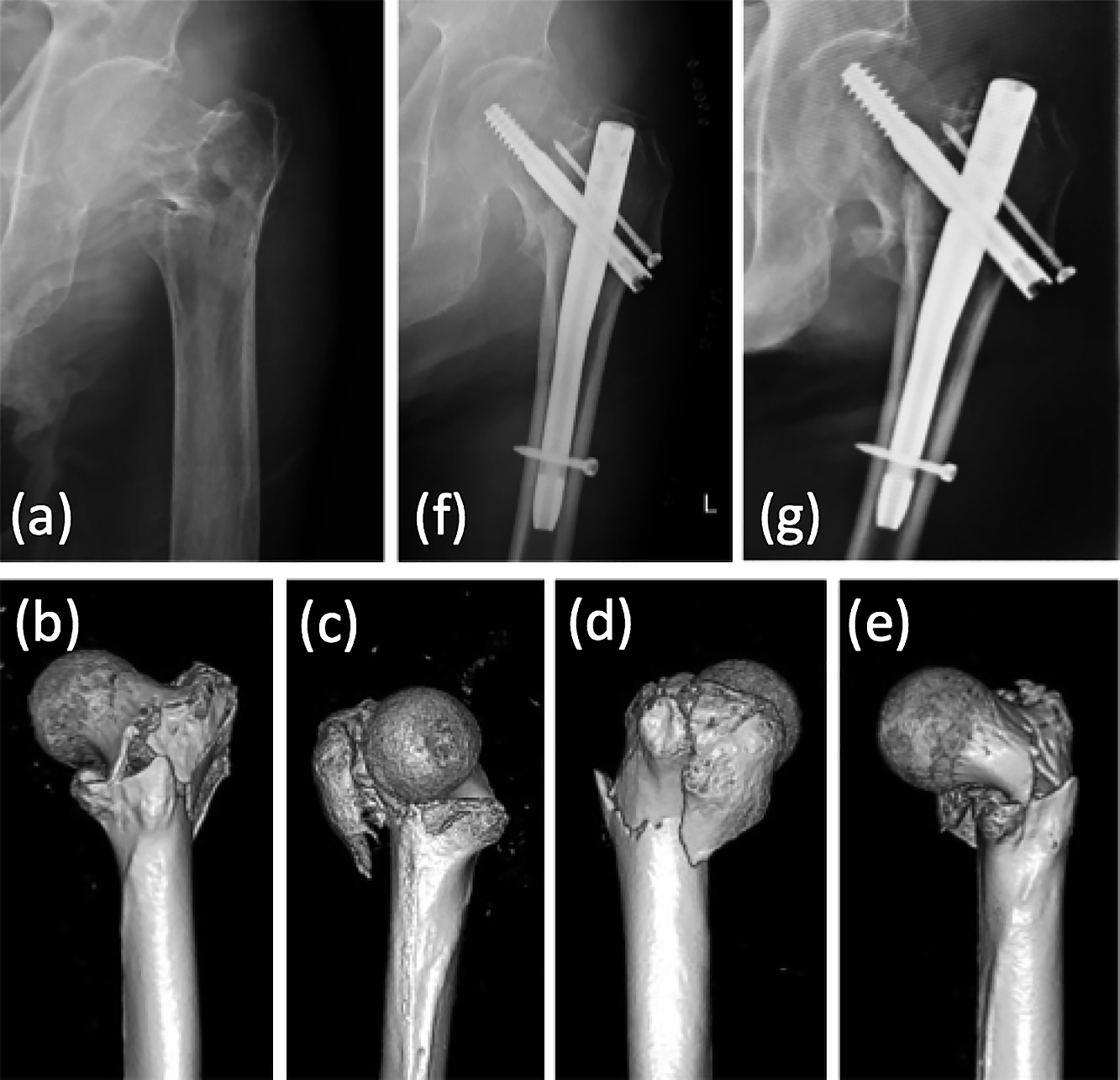
Early postoperative resumption of full weight-bearing is difficult after intramedullary nailing because of the combination of an unstable fracture pattern, osteoporosis, and the tendency of geriatric patients to have restricted mobility for various reasons.8 Internal fixation of unstable fractures may be accompanied by problems such as collapse, loss of fixation, and cut-out that lead to impaired function (Figure 1).9 Many surgeons have therefore recently suggested hemiarthroplasty to allow early full loading and prevent collapse in the fracture area.8,10–16
The purpose of this study was to evaluate the functional and clinical outcomes of bipolar hemiarthroplasty as the primary treatment for unstable intertrochanteric fracture in older patients.
Material and Methods
This retrospective study was conducted in accordance with the guidelines of the ethics committees of our institutes.
Of the 760 proximal femoral fractures in ambulatory patients treated surgically between 2013 and 2018 in our institutes, 66 unstable intertrochanteric fractures were treated by hemiarthroplasty and 60 of them were followed up over 12 months.
All study patients was aged over 75 years. Anteroposterior X-ray films of the pelvis, lateral X-ray films of the hip joint, and CT scan of the pelvis with multi planner reconstruction and 3D views were taken in all cases. The patients underwent elective surgery after management of avoidable anesthetic risks. The surgeries were performed under spinal or general anesthesia.
The fractures were classified according to the Jensen–Michaelsen classification.17
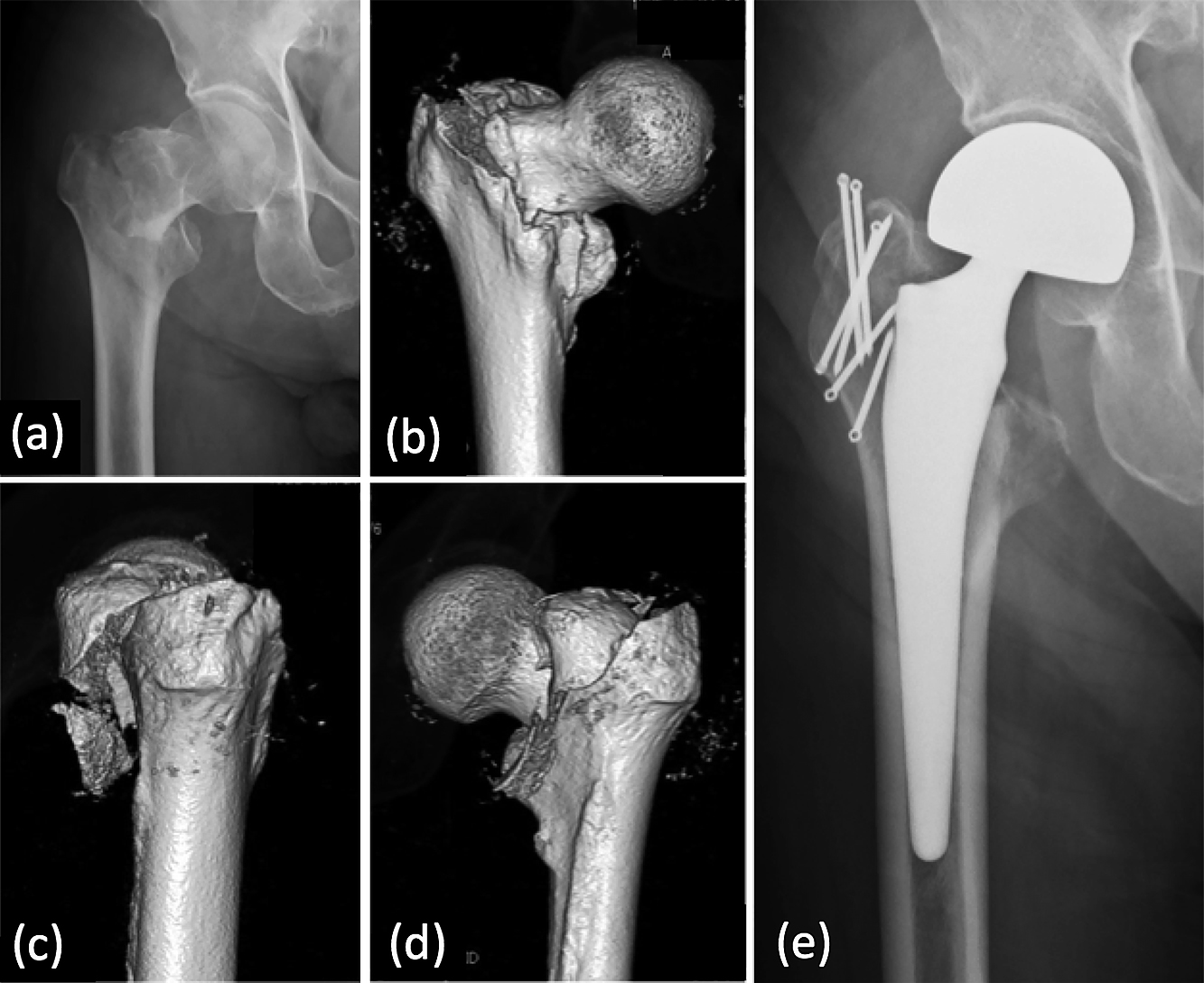
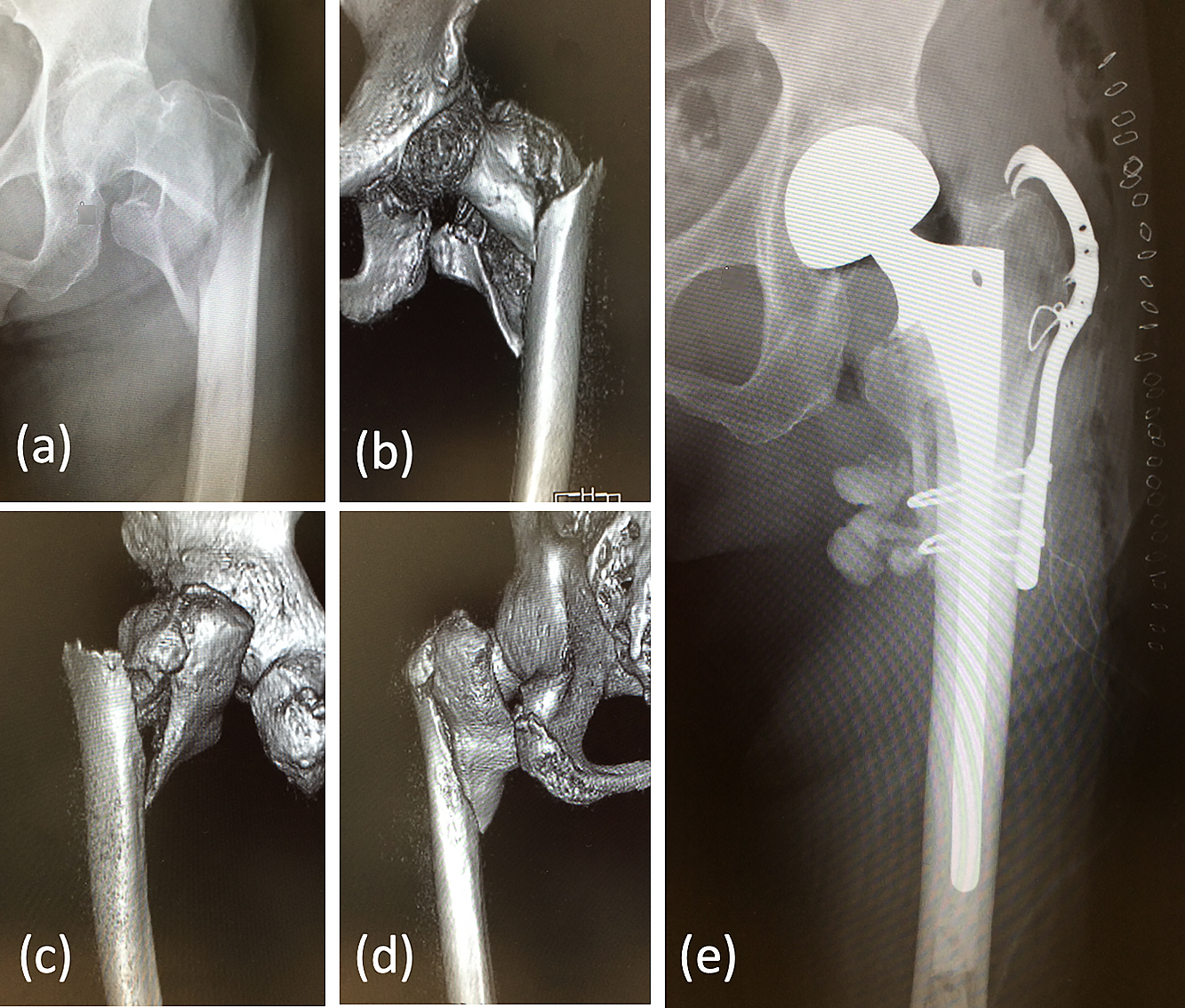
All surgeries were performed by the same surgical team using the standard posterolateral approach. After assessing the fracture, a T-shaped incision was made in the joint capsule and the femoral head was removed. In cases of posteromedial comminution, reconstruction was achieved using stainless steel surgical wires, Kirschner wires, or polyethylene cables, after which a cemented or uncemented bipolar prosthesis was inserted. In cases of comminution of the greater trochanter, stainless steel surgical wires, Kirschner wires, polyethylene cables, ring-pins or plates were used for reconstruction (Figures 2, 3). Use of cemented protheses was considered when the lesser trochanter had been displaced (Figure 3).
Antibiotics were administered only on the day of surgery. Postoperatively, adequate analgesics were given. The affected limb was kept in 30° of abduction with the help of a pillow between the thighs for 2 weeks.
All patients were referred to the rehabilitation department for prevention of disuse syndrome on admission, and allowed full weight-bearing as tolerated from the day after surgery. Sutures were removed 2 weeks after surgery. Patients were followed up for 12 months or more postoperatively and assessed both clinically and radiologically. Clinical evaluation was based on Harris Hip Scores,18 scores of <70 being classified as poor, 70–79 as fair, 80–89 as good, and 90–100 as excellent.
Results
Six of the 66 patients were excluded from the study because they died of non-surgery related causes. Thus, 60 patients were evaluated in this study.
The 60 patients comprised 16 men (27%) and 44 women (73%), and were aged from 75–96 years (average 86). Only 43 patients (72%) could walk without any support prior to the injury.
According to the Jensen–Michaelsen classification, 24 fractures were type III, 14 type IV, and 22 type V. Cement was used in 24 patients.
Surgery was performed under general anesthesia in 36 cases and spinal anesthesia in 24 cases. The average duration of surgery was 66.1±25.9 minutes (range 40–145). Additional wiring was used in 52 cases and additional plates in seven. The average volume of intraoperative hemorrhage was 207±145 mL (range 12–459) and 47 patients (78%) required blood transfusion, the total average amount transfused on the day of surgery and the following day being 2.1±1.8 units (range 0–6). The average duration of hospital stay was 24.5±15.0 days (range 6–59). Five patients were discharged home and 55 were transferred to nearby hospitals for rehabilitation. No dislocations occurred; however, two patients required additional surgeries because of periprosthetic fracture caused by falling out of bed. No surgical site or deep infections, pulmonary embolism (PE), deep vein thrombosis (DVT), or pneumonia occurred in this series; however, six patients had urinary tract infections (UTI).
At 12 months follow up, the outcomes of 11 patients (18%) were graded as excellent, of 25 (42%) as good, of 15 (25%) as fair, and of 9 (15%) as poor according to Harris Hip Scores (Table 1). No radiological abnormalities were detected.
Table1
Result of bipolar hemiarthroplasty for unstable intertrochanteric fractures
| Cases |
60 (16 males, 44 females) |
| Age (years) |
75–96 (average 86) |
| ADL before injury |
walk without support or cane for long walk: 43
with cane, crutch or walker: 14
wheel chair or cannot walk: 3 |
| Fracture type (Jensen-Michaelsen classification17) |
III: 24
IV: 14
V: 22 |
| Type of anesthesia |
General: 36
Spinal: 24 |
| Surgical time (minutes) |
40–145 (average 66±26) |
| Intraoperative hemorrhage (mL) |
12–459 (average 207±145) |
| Blood transfusion (on the day and the next day of surgery) |
47 cases
0–6 units (average 2.1±1.8) |
| Surgical site infection |
None |
| Harris Hip Score18 (at 12 months) |
Excellent: 11 (18%)
Good: 25 (42%)
Fair: 15 (25%)
Poor: 9 (15%) |
| ADL after surgery (at final follow up) |
walk without support or cane for long walk: 30
with cane, crutch or walker: 20
wheel chair or cannot walk: 10 |
Discussion
Management of unstable intertrochanteric fractures remains controversial, especially in patients with osteoporosis.19 Stable intertrochanteric fractures can easily be treated by osteosynthesis with predictable good results.2,20,21 Internal fixation achieves good results in stable fractures with good bone stock; however, all types of fixation devices have failed to achieve the same success rate in comminuted unstable and osteoporotic intertrochanteric fractures.22 The biological and biomechanical changes associated with osteoporosis make the management of these fractures more difficult. Cortical bone becomes thin and cancellous bone has reduced bone mineral density with changes in the trabecular pattern. Thus, the management of unstable intertrochanteric fractures is challenging because of poor bone quality and osteoporosis, as well as other age-associated comorbidities.7,21
Hip fractures are associated with notable morbidity and mortality in older patients. Rigid fixation and early rehabilitation can drastically reduce the mortality associated with intertrochanteric fractures.
Internal fixation in patients with age-related osteoporosis often has a high failure rate because of the poor bone quality,23 hindering early mobilization. The incidence of general complications such as PE, DVT, and pneumonia ranges from 22%–50% when mobilization is delayed after internal fixation.24,25
Restoration of mobility depends on the quality of bone and the type of implant used. In cases of comminuted fractures, fixation of the fragments is difficult and the posteromedial void in this region makes the fracture very unstable. The incidence of failure with unstable intertrochanteric fractures is as high as 50%,2 and the cut-out rate can be high as 4%–16.5% for hip screws.23,26,27 Thus, rigid internal fixation and early mobilization are the keys to successful treatment.
To enable early postoperative weight-bearing and rapid rehabilitation, several authors have recommended hemiarthroplasty for treatment of unstable intertrochanteric fractures.8,10–16
Tronzo28 claimed to be the first to use long, straight-stemmed prostheses for the primary treatment of intertrochanteric fractures. Subsequent studies also achieved good results with hemiarthroplasty.
In a comparative study of hemiarthroplasty versus internal fixation, Kayali et al.19 concluded that the clinical results of these procedures are similar. Grimsrud et al.29 also reported good outcomes.
Esen et al.30 compared proximal femoral nail-antirotation (PFNA) and cemented arthroplasty. They reported that duration of surgery, units of blood transfusion, and duration of hospital stay were less for PFNA; however, there was no significant difference in postoperative complications, Harris hip scores, or one-year mortality.30 They concluded that these techniques for performing bipolar hemiarthroplasty have equivalent outcomes in patients in an acceptable general condition.
Mansukhani et al. randomized 60 intertrochanteric fractures into three groups, and compared the clinical results of cemented hemiarthroplasty, dynamic hip screws, and proximal femoral nails, and found no significant disadvantage for arthroplasty.27
Patients who have undergone hemiarthroplasty are permitted immediate mobilization; thus, rehabilitation is quick and there are markedly fewer complications related to prolonged immobilization, such as decubitus ulcers, respiratory infection, and atelectasis.31 Treatment of unstable intertrochanteric fracture in older patients with bipolar hemiarthroplasty results in fewer complications of prolonged immobilization and easy rehabilitation along with a rapid return of functional level. Rodop32 also reported a successful result.
Treating unstable intertrochanteric fractures in older patients with compromised general health and comminuted fractures in osteoporotic bone stock by primary hemiarthroplasty essentially bypasses the phase of fracture healing by immediately providing a stable, mobile, relatively pain-free joint.8 This eliminates the need for prolonged immobilization and permits early ambulation. Davison et al. have also reported that cemented hemiarthroplasty provides the advantage of load bearing ambulation in the early post-operative period.9
There are reports that delayed surgery leads to muscle mass attenuation by 0.5%–0.6% per day and muscle strength attenuation by 2%–4% per day.33,34 Furthermore, Yamaguchi et al. reported that delaying starting walking rehabilitation results in an additional 2.8 days per days delayed to achieve the ability to walk.35 We have not used conventional surgical techniques that require a long period of non-weight-bearing to treat unstable intertrochanteric femoral fractures and therefore could not perform a comparative study. However, the functional results our patients achieved are comparable to those reported by others, as shown in Table 2. These studies had similar functional results and all concluded that hemiarthroplasty is a beneficial treatment for unstable intertrochanteric femoral fractures.
Table2
Comparison to other studies of Harris Hip Score at 12 months
|
Mansukhani27 |
Rawate8 |
Yadav15 |
Haentjens11 |
Sancheti20 |
Allam16 |
Rodop32 |
Our study |
| n= |
10 |
30 |
27 |
30 |
33 |
27 |
37 |
60 |
| Excellent |
30 (%) |
26.7 |
29.6 |
23.3 |
24.2 |
37.0 |
45.9 |
18.3 |
| Good |
40 |
33.3 |
66.7 |
36.7 |
48.5 |
44.4 |
37.8 |
41.7 |
| Fair |
20 |
33.3 |
3.7 |
23.3 |
18.2 |
18.5 |
8.1 |
25.0 |
| Poor |
10 |
6.7 |
0 |
16.7 |
9.1 |
0 |
8.1 |
15.0 |
To the best of our knowledge, no Japanese studies have yet assessed the outcomes of this surgical procedure. In summary, hip hemiarthroplasty is an effective salvage procedure and is the treatment of choice for unstable intertrochanteric femoral fractures in older patients.
Acknowledgment
We thank Dr Trish Reynolds, MBBS, FRACP, from Liwen Bianji, Edanz Group China (www.liwenbianji.cn/ac), for editing the English text of a draft of this manuscript.
Notes
Conflict of Interest
There are no conflicts of interest to declare.
References
- 1. Zuckerman JD. Hip fracture. N Engl J Med 1996; 334: 1519–1525.
- 2. Lindskog DM, Baumgaertner MR. Unstable intertrochanteric hip fractures in the elderly. J Am Acad Orthop Surg 2004; 12: 179–190.
- 3. Jensen JS. Trochanteric fractures. An epidemiological, clinical and biomechanical study. Acta Orthop Scand Suppl 1981; 188: 1–100.
- 4. Boldin C, Seibert FJ, Fankhauser F, Peicha G, Grechenig W, Szyszkowitz R. The proximal femoral nail (PFN)—a minimal invasive treatment of unstable proximal femoral fractures: a prospective study of 55 patients with a follow-up of 15 months. Acta Orthop Scand 2003; 74: 53–58.
- 5. Sierra RJ, Cabanela ME. Conversion of failed hip hemiarthroplasties after femoral neck fractures. Clin Orthop Relat Res 2002; 399: 129–139.
- 6. Kim WY, Han CH, Park JI, Kim JY. Failure of intertrochanteric fracture fixation with a dynamic hip screw in relation to pre-operative fracture stability and osteoporosis. Int Orthop 2001; 25: 360–362.
- 7. Larsson S. Treatment of osteoporotic fractures. Scand J Surg 2002; 91: 140–146.
- 8. Rawate P, Kale AR, Sonawane CS. Functional outcome of cemented bipolar hemiarthroplasty for unstable intertrochanteric fractures of femur in elderly: an Indian perspective. Int J Sci Study 2017; 5: 48–53.
- 9. Davison JN, Calder SJ, Anderson GH, Ward G, Jagger C, Harper WM, Gregg PJ. Treatment for displaced intracapsular fracture of the proximal femur. A prospective, randomised trial in patients aged 65 to 79 years. J Bone Joint Surg Br 2001; 83: 206–212.
- 10. Chan KC, Gill GS. Cemented hemiarthroplasties for elderly patients with intertrochanteric fractures. Clin Orthop Relat Res 2000; 371: 206–215.
- 11. Haentjens P, Lamraski G. Endoprosthetic replacement of unstable, comminuted intertrochanteric fracture of the femur in the elderly, osteoporotic patient: A review. Disabil Rehabil 2009; 27: 1167–1180.
- 12. Sinno K, Sakr M, Girard J, Khatib H. The effectiveness of primary bipolar arthroplasty in treatment of unstable intertrochanteric fractures in elderly patients. N Am J Med Sci 2010; 2: 561–568.
- 13. Kim SY, Kim YG, Hwang JK. Cementless calcar-replacement hemiarthroplasty compared with intramedullary fixation of unstable intertrochanteric fractures. A prospective, randomized study. J Bone Joint Surg Am 2005; 87: 2186–2192.
- 14. Puttakemparaju KV, Beshaj NR. Unstable intertrochanteric fracture in elderly treated with bipolar hemiarthroplasty: A prospective case series. African J Trauma 2014; 3: 81–86.
- 15. Yadav A, Mishra A, Yadav A, Kumar P, Kumar D. Functional evaluation of cemented hemiorthroplasties as a treatment option for unstable intertrochanteric fractures in the elderly: A prospectively case series study. International Journal of Orthopaedic Sciences 2017; 3: 520–523.
- 16. Allam AS. Primary cemented hemiarthroplasty for unstable intertrochanteric fractures in elderly: an intermediate follow-up. The Egyptian Orthopaedic Journal 2014; 49: 96–100.
- 17. Jensen JS, Michaelsen M. Trochanteric femoral fractures treated with McLaughlin osteosynthesis. Acta Orthop Scand 1975; 46: 795–803.
- 18. Harris WH. Traumatic arthritis of the hip after dislocation and acetabular fractures: treatment by mold arthroplasty. An end-result study using a new method of result evaluation. J Bone Joint Surg Am 1969; 51: 737–755.
- 19. Kayali C, Agus H, Ozluk S, Sanli C. Treatment for unstable intertrochanteric fractures in elderly patients: internal fixation versus cone hemiarthroplasty. J Orthop Surg (Hong Kong) 2006; 14: 240–244.
- 20. Sancheti KH, Sancheti P, Shyam A, Patil S, Dhariwal Q, Joshi R. Primary hemiarthroplasty for unstable osteoporotic intertrochanteric fractures in the elderly: A retrospective case series. Indian J Orthop 2010; 44: 428–434.
- 21. Marsh JL, Slongo TF, Agel J, Broderick JS, Creevey W, DeCoster TA, Prokuski L, Sirkin MS, Ziran B, Henley B, Audigé L. Fracture and dislocation classification compendium—2007: Orthopaedic Trauma Association classification, database and outcomes committee. J Orthop Trauma 2007; 10: S1–133.
- 22. Karthik K, Natarajan M. Unstable trochanteric fractures in elderly osteoporotic patients: role of primary hemiarthroplasty. Orthop Surg 2012; 4: 89–93.
- 23. Haidukewych GJ, Berry DJ. Hip arthroplasty for salvage of failed treatment of intertrochanteric hip fractures. J Bone Joint Surg Am 2003; 85: 899–904.
- 24. Kenzora JE, McCarthy RE, Lowell JD, Sledge CB. Hip fracture mortality. Relation to age, treatment, preoperative illness, time of surgery, and complications. Clin Orthop Relat Res 1984; 186: 45–56.
- 25. Baumgaertner MR, Curtin SL, Lindskog DM. Intramedullary versus extramedullary fixation for the treatment of intertrochanteric hip fractures. Clin Orthop Relat Res 1998; 348: 87–94.
- 26. Grisso JA, Kelsey JL, Strom BL, Chiu GY, Maislin G, O’Brien LA, Hoffman S, Kaplan F. Risk factors for falls as a cause of hip fracture in women. The Northeast Hip Fracture Study Group. N Engl J Med 1991; 324: 1326–1331.
- 27. Mansukhani SA, Tuteja SV, Kasodekar VB, Mukhi SR. A comparative study of the dynamic hip screw, the cemented bipolar hemiarthroplasty and the proximal femoral nail for the treatment of unstable intertrochanteric fractures. J Clin Diagn Res 2017; 11: RC14–19.
- 28. Tronzo RG. The use of an endoprosthesis for severely comminuted trochanteric fractures. Orthop Clin North Am 1974; 5: 679–681.
- 29. Grimsrud C, Monzon RJ, Richman J, Ries MD. Cemented hip arthroplasty with a novel cerclage cable technique for unstable intertrochanteric hip fractures. J Arthroplasty 2005; 20: 337–343.
- 30. Esen E, Dur H, Ataoğlu MB, Ayanoğlu T, Turanlı S. Evaluation of proximal femoral nail-antirotation and cemented, bipolar hemiarthroplasty with calcar replacement in treatment of intertrochanteric femoral fractures in terms of mortality and morbidity ratios. Eklem Hastalik Cerrahisi 2017; 28: 35–40.
- 31. Thakur A, Lal M. Cemented Hemiarthroplasty in Elderly Osteoporotic Unstable Trochanteric Fractures using Fracture Window. Malays Orthop J 2016; 10: 5–10.
- 32. Rodop O, Kiral A, Kaplan H. Primary bipolar hemiprosthesis for unstable intertrochanteric fractures. Int Orthop 2002; 26: 233–237.
- 33. Wall BT, Dirks ML, van Loon LJ. Skeletal muscle atrophy during short-term disuse: implications for age-related sarcopenia. Ageing Res Rev 2013; 12: 898–906.
- 34. Müller EA. Influence of training and of inactivity on muscle strength. Arch Phys Med Rehabil 1970; 51: 449–462.
- 35. Yamaguchi T, Sunaga K, Nakano N, Shimada E, Tajima K, Urabe T. Relation between the timing of surgery for hip fractures and postoperative ambulatory ability. Clinical Orthopaedic Surgery 2008; 43: 1177–1181 (in Japanese).