Abstract
Objective: To examine the associations of self-efficacy and outcome expectancy with adherence to continuous positive airway pressure (CPAP) therapy among Japanese men with obstructive sleep apnea (OSA) using objective adherence data for CPAP therapy.
Methods: We conducted a retrospective study of 497 Japanese men with OSA who were receiving CPAP therapy. Good adherence was defined as CPAP use of ≥4 hours per night for ≥70% of nights. Logistic regression models were used to calculate odds ratios (ORs) and 95% confidence intervals (CIs) for the associations of good adherence to CPAP therapy with self-efficacy and outcome expectancy (measured with the CPAP Self-Efficacy Questionnaire for Sleep Apnea in Japanese). The models were adjusted for age, duration of CPAP therapy, body mass index, apnea–hypopnea index, Epworth Sleepiness Scale score, and comorbidities (diabetes mellitus and hypertension).
Results: In total, 53.5% of participants had good adherence to CPAP therapy. The mean CPAP use was 5.18±1.53 hours/night. After adjusting for related factors, we found significant associations of good adherence to CPAP therapy with self-efficacy scores (OR, 1.10; 95% CI, 1.05–1.13; p<0.001) and outcome expectancy scores (OR, 1.10; 95% CI, 1.02–1.15; p=0.007).
Conclusions: Our results indicate that self-efficacy and outcome expectancy are associated with good adherence to CPAP therapy among Japanese men with OSA.
Introduction
Obstructive sleep apnea (OSA) is a common clinical condition characterized by repetitive upper airway collapse during sleep; it is a known risk factor for metabolic disease, hypertension, neurological disorders, cardiovascular disease, and mortality.1–6 Globally, an estimated 425 million people have moderate to severe OSA, for which treatment is generally recommended.7
Continuous positive airway pressure (CPAP) is considered the first-line therapy for OSA. CPAP reduces snoring, hypoxemia, and resultant arousals in patients with OSA, thereby improving their quality of life and neurocognitive function. Patients’ use of CPAP is critically important for effective treatment of OSA. However, adherence to CPAP therapy has been objectively measured from the records of CPAP devices, revealing low adherence.8 Low adherence to CPAP therapy among patients with OSA has been associated with several factors, including sociodemographic characteristics, disease severity, side effects, and psychosocial factors.8–10
Bandura’s social cognitive theory posits that there are multiple influences on behavior, with an emphasis on personal (e.g., cognitive) and environmental (e.g., social) factors.11,12 Psychosocial factors derived from this model include self-efficacy and outcome expectation. For patients with OSA treated with CPAP therapy, self-efficacy refers to the confidence and ability to self-manage CPAP treatment, and outcome expectancy refers to the self-perceived expectation of benefiting from CPAP treatment. Many studies have examined associations of adherence to CPAP therapy with self-efficacy and outcome expectancy in patients with OSA treated with CPAP therapy, but their results were inconsistent.12–20 In Asian patients with OSA, including Japanese patients, no studies have explored the association of self-efficacy and outcome expectancy with adherence to CPAP therapy using objective adherence data.
In the present study, we examined associations of adherence to CPAP therapy with self-efficacy and outcome expectancy among Japanese men with OSA using adherence data recorded with a CPAP device.
Methods
Participants
This study involved 998 Japanese men with OSA who were being treated with CPAP at SDB Research Laboratory, Takaoka Clinic, in August 2011. The patients’ apnea–hypopnea index (AHI) before CPAP therapy was obtained from overnight polysomnography recordings (Embla N7000; Embla Systems, Inc., Broomfield, CO, USA). The data obtained from these recordings included a continuous electroencephalogram, oculogram, electrocardiogram, electromyogram, respiratory channels including nasal and oronasal airflow, thoracic and abdominal respiratory movements and pulse oximetry, snoring, position, and video monitoring. Sleep stages and respiratory events were scored using the standard diagnostic criteria of the American Academy of Sleep Medicine and a criterion published by registered polysomnogram technicians.1 All participants in this study were patients with OSA who had an AHI of ≥20 events/hour or 5 to 19 events/hour and had undergone failed therapy with an oral appliance.21 Participants were excluded if therapy with their oral appliance was successful.
Survey procedure
Of the 998 participants, 705 (71%) completed a self-administered questionnaire in August 2011. The questionnaire included the CPAP Self-Efficacy Questionnaire for Sleep Apnea in Japanese (CSESA-J),22 the Epworth Sleepiness Scale (ESS),23 and items regarding the patients’ medical history. Weight was also self-reported in the questionnaire. The patients’ AHI before CPAP therapy, age, and height were obtained from clinical records at SDB Research Laboratory, Takaoka Clinic. Their body mass index (BMI) was calculated as weight divided by height in meters squared (kg/m2). Of 705 survey respondents, 579 (82%) provided their CPAP device with a smart card system, which records data on adherence to CPAP therapy.
The mean±standard deviation (SD) age and AHI of the 705 survey respondents was 56.0±11.2 years and 49.0±26.0 events/hour, respectively. The mean±SD age and AHI of the 579 patients who provided CPAP devices were 56.0±11.1 years and 49.8±26.0 events/hour, respectively, which were not significantly different from those for all survey respondents.
CPAP adherence
We obtained data on the participants’ CPAP therapy adherence, which was objectively measured by a smart card system. Using the data for 1 month after the patient completed the questionnaire, we classified CPAP use of ≥4 hours per night for ≥70% of nights as good adherence and other CPAP use as poor adherence.24
Self-efficacy measurement
We used the CSESA-J to measure participants’ self-efficacy and outcome expectancy. The CSESA-J is a scale for Japanese patients with OSA treated with CPAP under the Bandura’s social cognitive theory and has two subscales: self-efficacy and outcome expectancy.22 Its reliability and validity have been confirmed.
Data analyses
Of the 579 patients, we excluded 13 patients with missing questionnaire data, 35 female patients, and 36 patients with a history of cerebral or cardiovascular disease. Therefore, 497 patients with valid data were included in the analyses.
The average age, BMI, and AHI were compared between the good and poor adherence groups using independent-samples t-tests. The median and interquartile range were used to examine the duration of CPAP therapy and ESS score, and these factors were analyzed with the Wilcoxon rank sum test because of the large distortion in the data distribution. Logistic regression models were used to calculate the odds ratios (ORs) and 95% confidence intervals (CIs) for the associations of good adherence to CPAP therapy with self-efficacy and outcome expectancy scores, adjusted for age, duration of CPAP therapy, BMI, AHI, ESS score, and comorbidities (diabetes mellitus and hypertension).9,10,25 The level of statistical significance was set at 0.05. The analyses were performed using IBM SPSS Version 23 for Windows (IBM Japan Ltd., Tokyo, Japan).
Ethical considerations
All participants provided written informed consent before completing the self-administered questionnaire. This study was approved by the Fujita Health University Medical Research Ethics Committee, Aichi, Japan in November 2010 (10-198) and was conducted in accordance with the Declaration of Helsinki.
Results
Figure 1 shows the flow diagram of the study participants. Of the 497 participants analyzed, 266 (53.5%) had good adherence and 231 (46.5%) had poor adherence. The mean±SD duration of CPAP use was 5.18±1.53 hours/night. The participants’ characteristics and CSESA-J scores stratified by adherence group are shown in Table 1. There were no significant differences in mean age, mean BMI, mean AHI, median duration of CPAP therapy, median ESS score, or percentage of comorbid hypertension between the poor and good adherence groups. The percentage of patients with comorbid diabetes mellitus was significantly lower in the good adherence group than in the poor adherence group (p=0.024). The mean±SD self-efficacy and outcome expectancy scores in the good adherence group were 35.9±6.1 and 22.1±3.9, respectively, and those in the poor adherence group were 32.2±6.1 and 20.6±3.9, respectively. There were significant differences in the mean self-efficacy and outcome expectancy scores between the two adherence groups (Table 1).
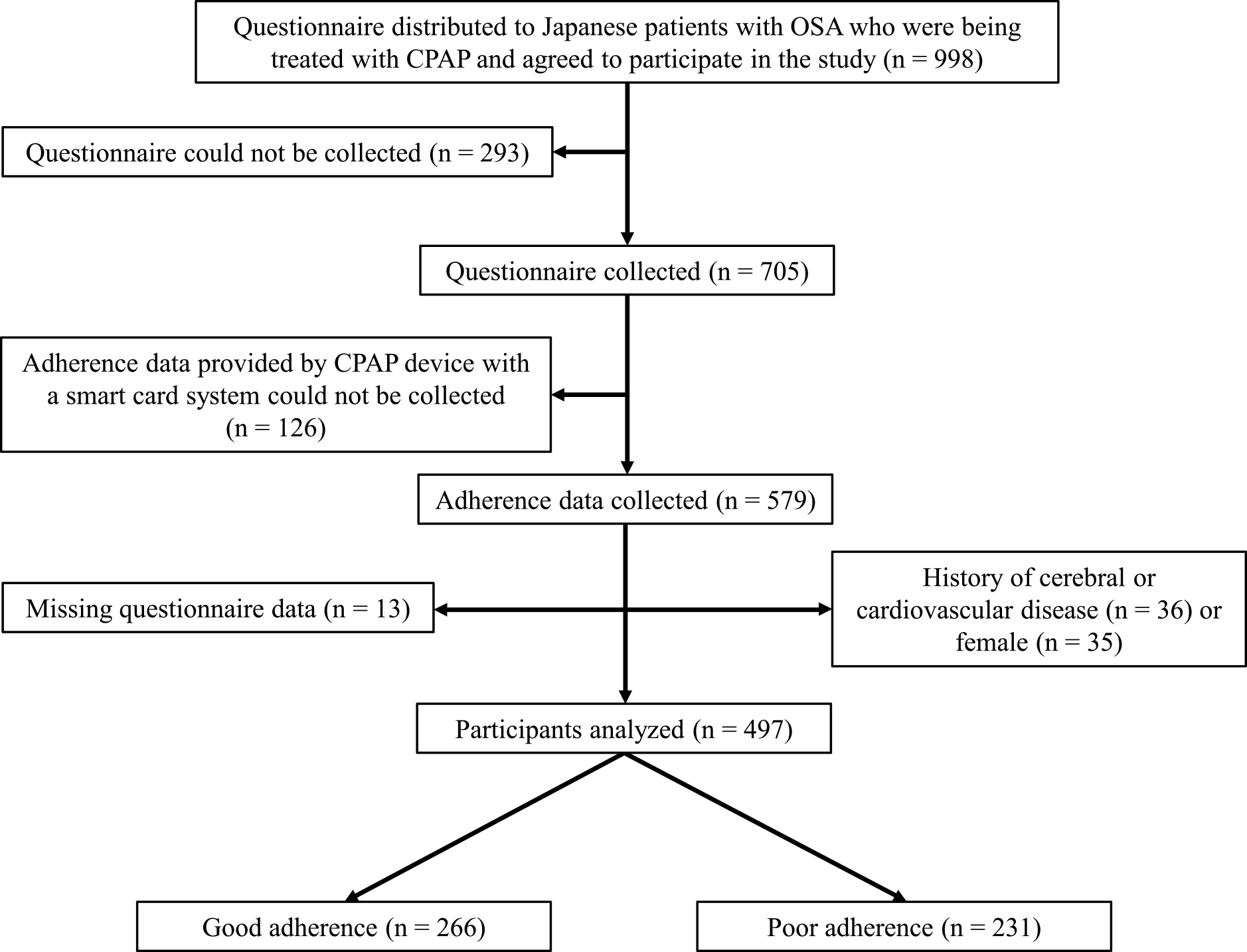
Table1
Characteristics and CSESA-J scores of Japanese men with OSA receiving CPAP therapy
|
Good adherence (n=266) |
Poor adherence (n=231) |
p-value |
| Characteristics |
| Age, years |
56.2±11.6 |
54.4±10.2 |
0.081 |
| Duration of CPAP therapy, years |
1.2 (0.5–5.9) |
1.5 (0.6–5.1) |
0.871 |
| BMI, kg/m2 |
28.4±4.9 |
28.4±5.5 |
0.898 |
| AHI, events/hour |
56.2±22.8 |
53.6±21.6 |
0.220 |
| ESS score |
8.0 (4.0–11.0) |
9.0 (6.0–13.0) |
0.110 |
| Comorbidities |
| Diabetes mellitus |
55 (44.0) |
70 (56.0) |
0.024 |
| Hypertension |
57 (55.3) |
46 (44.7) |
0.908 |
| CSESA-J |
| Self-efficacy score |
35.9±6.1 |
32.2±6.1 |
<0.001 |
| Outcome expectancy score |
22.1±3.9 |
20.6±3.9 |
<0.001 |
Data are presented as mean±standard deviation, median (interquartile range), or n (%).
Abbreviations: AHI, apnea–hypopnea index; BMI, body mass index; CPAP, continuous positive airway pressure; CSESA-J, CPAP Self-Efficacy Questionnaire for Sleep Apnea in Japanese; ESS, Epworth Sleepiness Scale; OSA, obstructive sleep apnea.
The ORs and 95% CIs for the associations of good adherence to CPAP therapy with self-efficacy and outcome expectancy scores are shown in Table 2. After adjusting for age, duration of CPAP treatment, BMI, AHI, ESS score, and comorbidities (diabetes mellitus and hypertension), there were significant associations of good adherence to CPAP therapy with self-efficacy scores (OR, 1.10; 95% CI, 1.05–1.13; p<0.001) and outcome expectancy scores (OR, 1.10; 95% CI, 1.02–1.15; p=0.007) (Table 2).
Table2
Associations of good adherence to CPAP therapy with self-efficacy and outcome expectancy in Japanese men with OSA
|
OR (95% CI) |
p-value |
Adjusted OR (95% CI) |
p-value |
| CSESA-J |
| Self-efficacy |
1.10 (1.07–1.14) |
<0.001 |
1.10 (1.05–1.13) |
<0.001 |
| Outcome expectancy |
1.10 (1.05–1.16) |
<0.001 |
1.10 (1.02–1.15) |
0.007 |
Abbreviations: CI, confidence interval; CPAP, continuous positive airway pressure; CSESA-J, CPAP Self-Efficacy Questionnaire for Sleep Apnea in Japanese; OR, odds ratio; OSA, obstructive sleep apnea.
Logistic regression models were used to calculate the OR and 95% CI for the associations of good adherence to CPAP therapy with self-efficacy and outcome expectancy scores, adjusted for age, duration of CPAP therapy, body mass index, apnea–hypopnea index, Epworth Sleepiness Scale score, and comorbidities (diabetes mellitus and hypertension).
Discussion
This is the first study to focus on the associations of self-efficacy and outcome expectancy with adherence to CPAP therapy based on objective adherence data among Asian patients with OSA. We found that self-efficacy was significantly associated with good adherence to CPAP therapy among Japanese men with OSA. Our finding is consistent with the results of most previous studies.13,15–20 These previous studies targeted different populations in Australia,13 the United States (Whites, Blacks, and Hispanics),15,16,19,20 Finland,18 and China.17 These studies used two scales to measure self-efficacy and outcome expectancy: the Social Cognitive Theory (SCT) scale and the Self-Efficacy Measure for Sleep Apnea questionnaire (SEMSA).26,27 These two scales were designed for Western patients. The CSESA-J22 used in the present study was developed for Japanese patients. All three scales are based on Bandura’s social cognitive theory. The present study confirmed the positive association between self-efficacy and good adherence to CPAP therapy using the CSESA-J among Japanese patients.
Our study also indicated that outcome expectancy was significantly associated with good adherence to CPAP therapy. Two previous studies conducted in China17 and Australia14 showed a positive association similar to that in our study, whereas three studies conducted in Australia13 and the United States15,16 showed no such association. Outcome expectancy may only be a cognitive factor in patients with OSA who have used CPAP treatment for a relatively long time because it reflects the self-perceived expectation of benefiting from CPAP treatment. Although there were many differences between those studies, including the present study, the mean duration of CPAP use per night in the two previous studies14,17 and the present study showing a positive association was 4.6 to 5.3 hours/night, which tended to be longer than in the three studies showing no association13,15,16 (2.5–3.2 hours/night). This suggests that there may be a positive association between outcome expectancy and adherence to CPAP therapy in a population with a relatively high adherence rate to CPAP therapy. If true, this finding will be helpful to determine the content of education that is needed for patients to improve their adherence to CPAP therapy. When directed toward altering patients’ views about CPAP, behavioral interventions such as cognitive behavioral therapy and motivational enhancement therapy appeared to be effective in promoting adherence.12 Further research is needed to clarify the relationship between adherence to CPAP therapy and outcome expectancy in patients with OSA.
This study had several limitations. First, no unified definition of adherence is available, and previous studies have shown that the prevalence of good adherence among people being treated with CPAP ranges from 30% to 60%.8 We used a common definition of good adherence as the use of CPAP for ≥4 hours per night for ≥70% of nights.24 Second, our study was retrospective in nature and conducted at a single clinic for sleep-disordered breathing. Third, our participants were patients who continued medical treatment for OSA and did not include those who discontinued treatment. We were not able to examine the status of CPAP treatment discontinuation. Two previous studies from the United States16,19 also included patients with OSA who were receiving CPAP therapy and were already being followed up. Fourth, the collection rate in this study was not high, but the mean age and AHI were similar between the 705 participants who completed the questionnaire and the 579 participants with valid data on CPAP therapy adherence. Fifth, all participants in this study were male because there were few female patients at the studied clinic. A previous study showed that sex may be associated with CPAP adherence.9 Although the percentage of female patients with OSA is not high, a further study with data obtained from more female subjects would provide important information. The final limitation is that the adjustment factors were selected based on previous studies; these factors included age, duration of CPAP therapy, BMI, AHI, ESS score, and comorbidities (diabetes mellitus and hypertension).9,10,25 It could have been helpful to include other factors that might have influenced our results (e.g., insomnia, subjective symptoms, socioeconomic status, and education level).9 Although it would have been useful to include these factors in the analyses, this information was not available in our study.
In conclusion, our results indicate that self-efficacy and outcome expectancy are significantly associated with good adherence to CPAP therapy in Japanese men with OSA.
Acknowledgments
The authors would like to acknowledge the support of the staff and polysomnography technologists at SDB Research Laboratory, Takaoka Clinic. This study was conducted at SDB Research Laboratory, Takaoka Clinic, Nagoya, Japan.
Notes
Disclosure Statement
The authors declare that there are no financial conflicts of interest.
References
- 1. Sleep–related breathing disorders in adults: Recommendations for syndrome definition and measurement techniques in clinical research. The Report of an American Academy of Sleep Medicine Task Force. Sleep 1999; 22: 667–689.
- 2. Sánchez-de-la-Torre M, Campos-Rodriguez F, Barbé F. Obstructive sleep apnoea and cardiovascular disease. Lancet Respir Med 2013; 1: 61–72.
- 3. Hou H, Zhao Y, Yu W, Dong H, Xue X, Ding J, Xing W, Wang W. Association of obstructive sleep apnea with hypertension: A systematic review and meta-analysis. J Glob Health 2018; 8: 010405.
- 4. Reutrakul S, Mokhlesi B. Obstructive sleep apnea and diabetes: A state of the art review. Chest 2017; 152: 1070–1086.
- 5. Muraki I, Wada H, Tanigawa T. Sleep apnea and type 2 diabetes. J Diabetes Investig 2018; 9: 991–997.
- 6. Yaggi HK, Concato J, Kernan WN, Lichtman JH, Brass LM, Mohsenin V. Obstructive sleep apnea as a risk factor for stroke and death. N Engl J Med 2005; 353: 2034–2041.
- 7. Benjafield AV, Ayas NT, Eastwood PR, Heinzer R, Ip MSM, Morrell MJ, Nunez CM, Patel SR, Penzel T, Pepin JLD, Peppard PE, Sinha S, Tufik S, Valentine K, Malhotra A. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respir Med 2019; 7: 687–698.
- 8. Rotenberg BW, Murariu D, Pang KP. Trends in CPAP adherence over twenty years of data collection: a flattened curve. J Otolaryngol Head Neck Surg 2016; 45: 43.
- 9. Mehrtash M, Bakker JP, Ayas N. Predictors of continuous positive airway pressure adherence in patients with obstructive sleep apnea. Lung 2019; 197: 115–121.
- 10. Tsuyumu M, Tsurumoto T, Iimura J, Nakakjima T, Kojima H. Ten-year adherence to continuous positive airway pressure treatment in patients with moderate-to-severe obstructive sleep apnea. Sleep Breath 2020; 24: 1565–1571.
- 11. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev 1977; 84: 191–215.
- 12. Weaver TE. Novel aspects of CPAP treatment and interventions to improve CPAP adherence. J Clin Med 2019; 8: 2220.
- 13. Richards D, Bartlett DJ, Wong K, Malouff J, Grunstein RR. Increased adherence to CPAP with a group cognitive behavioral treatment intervention: a randomized trial. Sleep 2007; 30: 635–640.
- 14. Olsen S, Smith S, Oei T, Douglas J. Health belief model predicts adherence to CPAP before experience with CPAP. Eur Respir J 2008; 32: 710–717.
- 15. Sawyer AM, Canamucio A, Moriarty H, Weaver TE, Richards K, Kuna ST. Do cognitive perceptions influence CPAP use? Patient Educ Couns 2011; 85: 85–91.
- 16. Wallace DM, Shafazand S, Aloia MS, Wohlgemuth WK. The association of age, insomnia, and self-efficacy with continuous positive airway pressure adherence in black, white, and Hispanic US veterans. J Clin Sleep Med 2013; 9: 885–895.
- 17. Deng T, Wang Y, Sun M, Chen B. Stage-matched intervention for adherence to CPAP in patients with obstructive sleep apnea: a randomized controlled trial. Sleep Breath 2013; 17: 791–801.
- 18. Kreivi HR, Maasilta P, Bachour A. Willingness score obtained after a short CPAP trial predicts CPAP use at 1 year. Sleep Breath 2014; 18: 207–213.
- 19. Dzierzewski JM, Wallace DM, Wohlgemuth WK. Adherence to continuous positive airway pressure in existing users: Self-efficacy enhances the association between continuous positive airway pressure and adherence. J Clin Sleep Med 2016; 12: 169–176.
- 20. Saconi B, Yang H, Watach AJ, Sawyer AM. Coping processes, self-efficacy, and CPAP use in adults with obstructive sleep apnea. Behav Sleep Med 2020; 18: 68–80.
- 21. Shiomi T, Sasanabe R. Advances in diagnosis and treatment of sleep apnea syndrome in Japan. JMAJ 2009; 52: 224–230.
- 22. Saito A, Kojima S, Sasaki F, Hayashi M, Mieno Y, Sakakibara H, Hashimoto S. Development and evaluation of a self-efficacy instrument for Japanese sleep apnea patients receiving continuous positive airway pressure treatment. Nat Sci Sleep 2015; 7: 25–31.
- 23. Johns MW. A new method for measuring daytime sleepiness: The Epworth Sleepiness Scale. Sleep 1991; 14: 540–545.
- 24. Kribbs NB, Pack AI, Kline LR, Smith PL, Schwartz AR, Schubert NM, Redline S, Henry JN, Getsy JE, Dinges DF. Objective measurement of patterns of nasal CPAP use by patients with obstructive sleep apnea. Am Rev Respir Dis 1993; 147: 887–895.
- 25. Kojima S, Saito A, Sasaki F, Hayashi M, Mieno Y, Sakakibara H, Hashimoto S. Associations of diabetes mellitus and hypertension with adherence to continuous positive airway pressure therapy in male patients with obstructive sleep apnea. Fujita Med J 2022; 8: 37–41.
- 26. Weaver TE, Maislin G, Dinges DF, Younger J, Cantor C, McCloskey S, Pack AI. Self-efficacy in sleep apnea: Instrument development and patient perceptions of obstructive sleep apnea risk, treatment benefit, and volition to use continuous positive airway pressure. Sleep 2003; 26: 727–732.
- 27. Stepnowsky CJ, Marler MR, Ancoli-Israel S. Determinants of nasal CPAP compliance. Sleep Med 2002; 3: 239–247.
