Abstract
Emotional disturbance including depression is associated with increased mortality among dialysis patients. The Self-Rating Depression Scale (SDS) is a simple tool for assessing emotional disturbance. This study investigated the relationship between emotional conditions as assessed with the SDS test and mortality among 491 hemodialysis patients. At baseline, 183 (37.3%), 180 (36.7%), 108 (22.0%), and 20 (4.1%) were classified as normal, borderline depression, depression, and severe depression, respectively. During the two years of observation period, 57 of 491 (11.6%) died. The SDS scores in the non-survivors were significantly higher than those in the survivors (p<0.0001). Logistic analyses showed that the diagnoses made by the SDS test were associated with significantly greater risks for all-cause mortality (99%CI: 1.905-3.698 for that without adjustment, 1.999-4.382 for that with full adjustment). When the SDS score = 50 was selected as the cut off value, the test screened two-year all cause death with sensitivity = 57.9% and the specificity = 78.1%. In conclusion, hemodialysis patients had high prevalence of emotional disturbance assessed by the SDS test, and high SDS score was significantly associated with all-cause mortality. These findings underscore the importance of screening for emotional conditions using the SDS test among hemodialysis patients.
Introduction
Emotional disturbance is regarded as a risk factor for the development of cardiovascular disease1-3). Although its direct effect on mortality is still in controversy4), it shows significant association with unfavorable clinical outcomes in many disease conditions5-7). For instance, depression is associated with increased mortality8-10) and risk of hospitalization11) among patients with end-stage kidney disease. However, since it is difficult to assess a patient’s emotional condition objectively, the impact of emotional disturbance on dialysis medicine remains unclear. In addition, Japanese dialysis patients had a considerably higher rate of suicide than the general population with a standardized mortality rate of 2.9 in 200912). This rate is unacceptably high given that the suicide rate in the Japanese general population is the eighth highest in the world and the highest among developed countries.
The Self-Rating Depression Scale (SDS) test13) is a tool for assessing emotional disturbance including depression that was developed in 1955. Since the SDS is a simple tool, which can be used for assessment in a variety of patients. It is now covered by Japanese medical insurance and therefore has become the most commonly used tool to assess emotional disturbance in daily clinical practice in this country. Nevertheless, information is lacking about prevalence of emotional disturbance assessed with the SDS test among hemodialysis patients.
The aims of this study are to investigate the relationship between the emotional condition assessed by the SDS test and mortality among dialysis patients.
Patients and Methods
Emotional condition was assessed with the SDS test among adult patients undergoing stable maintenance hemodialysis therapy in Akebono Clinic, Kumamoto, Santo Clinic, Niigata, Kido Hospital, Niigata, Takeda General Hospital, Aiduwakamatsu, Niigata Rinko Hospital, Niigata, and Suibarago Hospital, Agano, in order to screen depressive patients as a part of routine clinical practice in 2007. The test was performed before a regular hemodialysis session. The standard Japanese version of the SDS test (Chiba Test, Tokyo, Japan) was used. The participants received brief instructions before the test; however, they answered the questions by themselves without any assistance once the test started. No particular time limit was set for the test. Those who answered all of the SDS questions underwent the evaluation, while those with incomplete answers were not. Patients with SDS scores less than 40 were categorized as the normal group, those with scores between 40 and 49 were considered as the border-line depressive group, those with scores between 50 and 59 were considered as the depressive group, and those with scores more than 59 fell into the severely depressive group.
The confirmation of the survival of those received the SDS test in 2007 was made at 24 months after the test. The SDS scores among two-year survivor and non-survivor were compared with an unpaired t-test. The association between diagnosis made by the SDS scores and all-cause mortality was evaluated using logistic regression models. Three models were developed. The data were assessed without any adjustment (Model 1), adjusted for age and sex (Model 2), and finally adjusted for age, sex, dialysis vintage and diabetes mellitus (Model 3). For these analyses, age was categorized into 4 groups; -54, 55-64, 65-74, 75- (yo) and dialysis vintage was categorized into 5 groups; 0, 1-2, 3-4, 5-9, 10- (y), respectively. A p value of less than 0.05 was considered significant, and all tests were two-tailed. The usefulness of the SDS test as a screening tool for two-year survival was evaluated by a receiver operated characteristic (ROC) analysis.
Patients with serious complications that could affect two-year survival such as malignancy or cardiovascular diseases were excluded from the analyses. Before the data acquisition, the patients were duly informed the study and written consents were obtained. The study protocol was approved by each hospital committee.
Results
Seven-hundred and fifteen patients underwent the SDS test; however, 209 of those 715 provided incomplete answers to the questioners, and cancer had been found at the time of the test in 15. Thus, the remaining 491 were ultimately subjected to the analyses (Figure 1). Table 1 shows the clinical features of those 491 dialysis patients stratified by four categories of the SDS score. There were no particular deviations in terms of age, gender, dialysis vintage, and prevalence of diabetes mellitus in these 491 patients from general features among Japanese dialysis patients.
The distribution of the SDS scores is shown in the Fig. 2. Overall, the average (SD) score was 42.8(9.8). Of the 491, 20 (4.1%) were classified with severe depression, 108 (22.0%) were with depression, 180 (36.7%) were as having borderline depression, and 183 (37.3%) were as normal, respectively. No significant relationship was found between the SDS score and age, vintage of dialysis therapy, sex, or complication of diabetes mellitus.
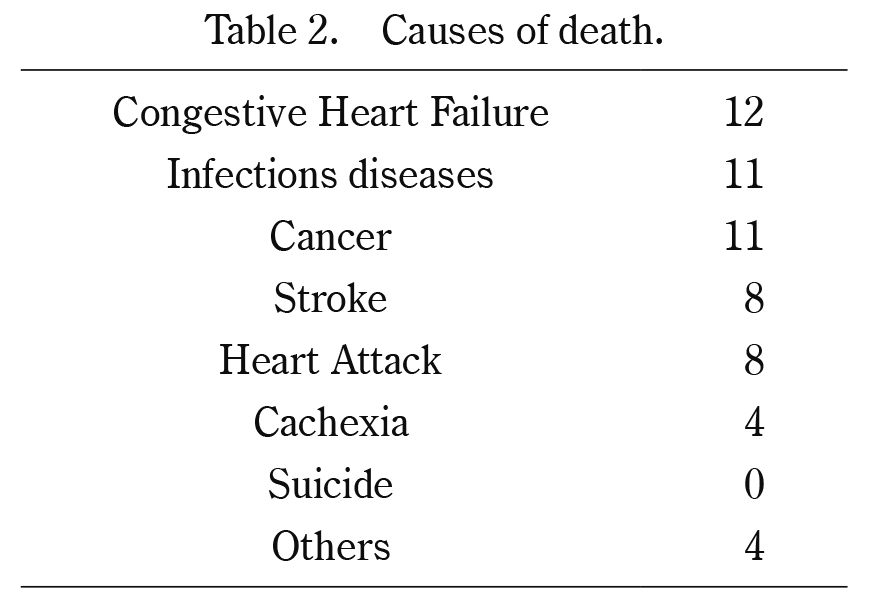
Of the 491 patients, 57 (11.6%) died during the two years of observation period due to cardiovascular disease, infection, cancer, in that order. No one died due to suicide (Table 1, 2). The SDS scores in the non-survivors were significantly higher than those in the survivors (Fig. 2). The two-year mortality in depression or severe depression groups was significantly worse than that in normal or borderline-depression groups (Table 1). However, no particular increase was noted in the cause of death.
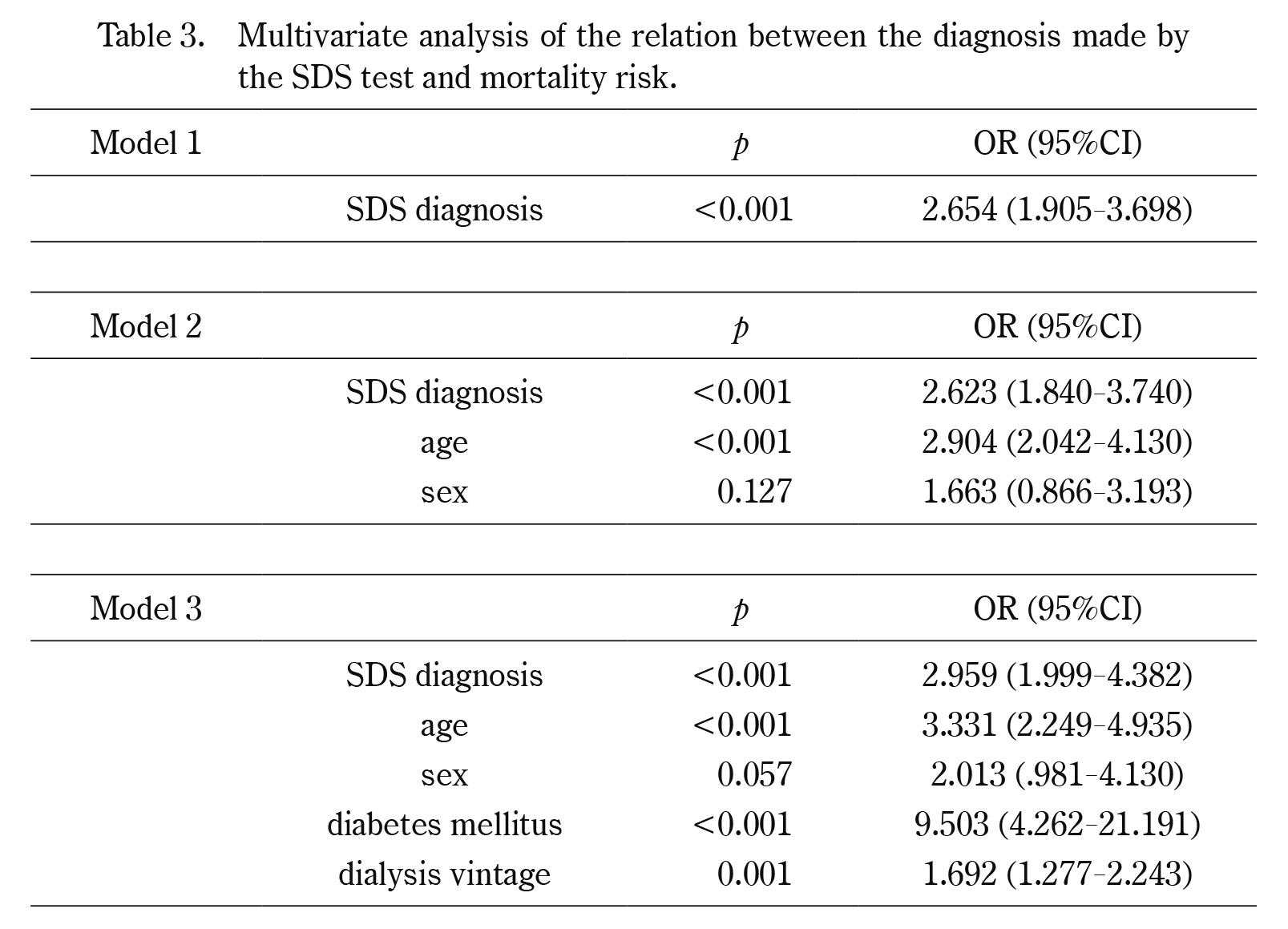
Table 3 demonstrates that the diagnosis of emotional disturbance made by the SDS test was significantly associated with two-year all cause death regardless of any adjustment models.
Figure 3 shows a ROC curve when the SDS score was applied as the screening tool for two-year survival. The amount of area under curve was 0.691. The maximum Youden Index was indicated when SDS score = 50 was selected as the cut off value (arrow), where the sensitivity =57.9% and the specificity = 78.1% were obtained, respectively.
Discussion
The SDS test is the most commonly used self-assessing tool for emotional disturbance, today. It is a convenient test while still preserving its objectivity. Therefore, we could successfully obtain complete responses from nearly 500 patients. While many clinical studies have focused on the relationship between emotional disturbance and mortality among maintenance dialysis patients8-10,14,15), the present study involved a relatively large number of participants.
Although many clinicians have assumed that the prevalence of emotional disturbance would be high among hemodialysis patients16), the precise prevalence remains unknown17). Previous studies reported that the mean SDS score was between 36.8 and 38.7 among Japanese non-dialyzed general participants including those with emotional disturbance18-20). Majority of those participants showed SDS score less than 40, and those with scores more than 40 were concluded to have a need to receive further emotional assessments. Compared to those previous Japanese reports, the mean SDS score of 42.8 demonstrated by our dialysis patients seems extremely high. Moreover, only 37.3% of our dialysis patients displayed SDS scores less than 40, and more than a quarter of them were suspected to be in depressive or severely depressive state (Table 2). Taken together, our data supported the conventional assumption that many hemodialysis patients are under emotional disturbance.
One remarkable finding in our data was no gender difference in the SDS scores. Generally, women show a higher incidence of emotional disturbance than men. Being under maintenance hemodialysis therapy may be an overwhelming factor inducing emotional disturbance that has masked the effect of gender. The lostness of kidney function itself severely damages emotional condition among dialysis patients. Moreover, surviving under hemodialysis therapy which restricts daily living becomes another psychosomatic stress21). Such environmental factors may even affect life prognosis. However, the absence of an inter-gender difference might be specific to Japanese dialysis patients, because a previous paper reported that female dialysis patients showed severer emotional disturbance than male dialysis patients22).
Our results demonstrated a significant association between the severity of emotional disturbance as assessed by the SDS score and mortality. In particular, less than half of cases with severe depression, i.e. with an SDS score no less than 60, survived the 48-month of observation period, indicating that severe depression was a critically strong prognosis-predicting factor. The results appear to be in accordance with previous reports8-10,14,15). We do not have clear explanation for this result, because no particular cause of death was noted among the non-survivors with high SDS scores. Emotional disturbance may not be the direct cause of death, but possibly harms through modifying other somatic conditions such as blood pressure, appetite or so on. Moreover, their emotional disturbance may not be a causative factor of fatal disease, but possibly is a consequence of occult disease. In this regard, aggressive screening of occult disease among severely depressed patients is one possible application to make use of the SDS test among dialysis patients. However, the SDS test did not show enough accuracy to screen mortality among dialysis patients by itself (Fig. 3).
The present study has some limitations to be noted. First, this is not a prospective clinical trial but a mere retrospective observation study. Therefore, the SDS test was performed only once and the survival was confirmed 24 months later. Emotional conditions might change or fluctuate during the 24 months, but such changes were not taken into consideration in this study. We could not obtain full clinical information including medication from the patients, either. Since the SDS test was performed for the purpose of screening depressive patients as a part of routine clinical practice, those with higher SDS scores had more chance of anti-depressants prescription after the test, which has potentially affected their study result. However, we should note that very few hemodialysis patients were given anti-depressants in Japan, and the present study period was soon after the publication of the paper23).
Finally, we applied the SDS test to assess each patient’s emotional condition. The gold standard for a diagnosis of depression is a clinical interview that based on the Diagnostic and Statistical Manual of Mental Disorders 5th edition (DSM-5). However, because of the time and expense required to administer a clinical interview, epidemiologic type studies often use self-report questionnaires. Among many self-assessment systems for determining emotional conditions, the SDS test tends to judge the patient’s emotional condition to be severer in those with somatic complications, because there are many questions about physical activity such as sexual activity. Therefore, other methods have been preferred to be applied for emotional assessment among dialysis patients24). However, all dialysis patients are associated with obvious severe somatic complications. If such conditions including sexual dysfunction25,26) affect emotional disturbance, the SDS score may rather reflect the patient’s true emotional condition. Note that the association between emotional disturbance assessed by the SDS test and mortality was extremely strong. The reason might be that the scores not only reflected the emotional conditions but were also affected by somatic conditions. However, we have to admit that the SDS test looks inferior in terms of objectivity when compared with modern comprehensive evaluating procedures such as Montgomery- Åsberg Depression Rating Scale or Hamilton Rating Scale for Depression.
Despite these limitations, this study also has several strengths. First, the present study involved a large number of participants. Many previous studies have focused on the relationship between emotional disturbance and mortality among maintenance dialysis patients8-10,14,15), however, these studies included small sample. Second, similar trials could be performed in any Japanese dialysis unit because the assessment of emotional condition with the SDS test is covered by medical insurance.
In conclusion, Japanese hemodialysis patients had a high prevalence of emotional disturbance and severely disturbed emotional condition was associated with poor two-year life prognosis. The SDS test is a practical and useful tool for a screening of emotional conditions among hemodialysis patients.
Conflict of Interests: none
References
- 1. Grippo AJ, Johnson AK. Stress, depression and cardiovascular dysregulation: a review of neurobiological mechanisms and the integration of research from preclinical disease models. Stress, 12: 1-21, 2009.
- 2. Rutledge T, Linke SE, Krantz DS et al. Comorbid depression and anxiety symptoms as predictors of cardiovascular events: results from the NHLBI-sponsored Women’s Ischemia Syndrome Evaluation (WISE) study. Psychosom Med, 71: 958-964, 2009.
- 3. Ariyo AA, Haan M, Tangen CM et al. Depressive symptoms and risks of coronary heart disease and mortality in elderly Americans. Cardiovascular Health Study Collaborative Research Group. Circulation, 102: 1773-1779, 2000.
- 4. Everson-Rose SA, House JS, Mero RP. Depressive symptoms and mortality risk in a national sample: confounding effects of health status. Psychosom Med, 66: 823-830, 2004.
- 5. Sullivan MD, O’Connor P, Feeney P et al. Depression predicts all-cause mortality: epidemiological evaluation from the ACCORD HRQL substudy. Diabetes Care, 35: 1708-1715, 2012.
- 6. Givens JL, Sanft TB, Marcantonio ER. Functional recovery after hip fracture: the combined effects of depressive symptoms, cognitive impairment, and delirium. J Am Geriatr Soc, 56: 1075-1079, 2008.
- 7. Pohjasvaara T, Vataja R, Leppävuori A et al. Depression is an independent predictor of poor long-term functional outcome post-stroke. Eur J Neurol, 8: 315-319, 2001.
- 8. Kimmel PL, Peterson RA, Weihs KL et al. Multiple measurements of depression predict mortality in a longitudinal study of chronic hemodialysis outpatients. Kidney Int, 57: 2093-2098, 2000.
- 9. Lopes AA, Bragg J, Young E et al. Depression as a predictor of mortality and hospitalization among hemodialysis patients in the United States and Europe. Kidney Int, 62: 199-207, 2002.
- 10. Kojima M, Hayano J, Suzuki S et al. Depression, alexithymia and long-term mortality in chronic hemodialysis patients. Psychother Psychosom, 79: 303-311, 2010.
- 11. Lacson E Jr, Bruce L, Li NC, et al. Depressive affect and hospitalization risk in incident hemodialysis patients. Clin J Am Soc Nephrol, 9: 1713-1719, 2014.
- 12. Wakasugi M, Kazama JJ, Yamamoto S et al.MCause-specific excess mortality among dialysis patients: A comparison with the general population in Japan. Ther Aphe Dial, 17: 298-304, 2013.
- 13. Zung WW, Richards CB, Short MJ. Self-rating depression scale in an outpatient clinic. Further validation of the SDS. Arch Gen Psychiatry, 13: 508-515, 1965.
- 14. Hedayati SS, Bosworth HB, Briley LP et al. Death or hospitalization of patients on chronic hemodialysis is associated with a physician-based diagnosis of depression. Kidney Int, 74: 930-936, 2008.
- 15. Rosenthal Asher D, Ver Halen N, Cukor D. Depression and nonadherence predict mortality in hemodialysis treated end-stage renal disease patients. Hemodial Int, 16: 387-393, 2012.
- 16. Ng HJ, Tan WJ, Mooppil N, et al. Prevalence and patterns of depression and anxiety in hemodialysis patients: a 12-month prospective study on incident and prevalent populations. Br J Health Psychol, 20: 374-395, 2015.
- 17. Cukor D, Peterson RA, Cohen SD, Kimmel PL. Depression in end-stage renal disease hemodialysis patients. Nat Clin Pract Nephrol, 2: 678-687, 2006.
- 18. Ogawa M, Takamatsu K, Horiguchi F. Evaluation of factors associated with the anxiety and depression of female infertility patients. Biopsychosoc Med, 5: 15, 2011.
- 19. Sawa M, Yamashita H, Fujimaki K et al. Depressive symptoms and apathy are associated with psychomotor slowness and frontal activation. Eur Arch Psychiatry Clin Neurosci, 262: 493-499, 2012.
- 20. Demura S, Sato S, Tada N et al. Agreement in depression determination among four self-rating depression scales applied to Japanese community-dwelling elderly. Environ Health Prev Med, 11: 177-183, 2006.
- 21. Cohen SD, Norris L, Acquaviva K, et al. Screening, diagnosis, and treatment of depression in patients with end-stage renal disease. Clin J Am Soc Nephrol, 2: 1332-1342, 2007.
- 22. Lopes GB, Matos CM, Leite EB et al. Depression as a potential explanation for gender differences in health-related quality of life among patients on maintenance hemodialysis. Nephron Clin Pract, 115: c35-40, 2010.
- 23. Fukuhara S, Green J, Albert J et al. Symptoms of depression, prescription of benzodiazepines, and the risk of death in hemodialysis patients in Japan Kidney Int, 70: 1866-1872, 2006.
- 24. Kimmel PL, Peterson RA. Depression in end-stage renal disease patients treated with hemodialysis: tools, correlates, outcomes, and needs. Semin Dial, 18: 91-97, 2005.
- 25. Santoro A, Zucchelli A, Triolo G et al. Prevalence and correlates of erectile dysfunction in men on chronic haemodialysis: a multinational cross-sectional study. Nephrol Dial Transplant, 27: 2479-2488, 2012.
- 26. Strippoli GF, Vecchio M, Palmer S et al. Sexual dysfunction in women with ESRD requiring hemodialysis. Clin J Am Soc Nephrol, 7: 974-981, 2012.