Abstract
Objective: Anastomotic leakage (AL) is one of the most devastating complications of rectal cancer surgery. Not only does AL result in reduced quality of life, extended hospitalization and impaired defecatory function, it also has a high local recurrence rate. In this study, we investigated risk factors for AL as it may help to decrease its occurrence and improve patient outcomes.
Methods: This study was a retrospective, single-institution study of rectal cancer patients who underwent elective low anterior resection between April 2002 and February 2018 at Fukushima Medical University Hospital. Patients were divided into two groups according to the presence of AL. Patient-, tumor-, and surgery-related variables were examined using univariate and multivariate analyses.
Results: One hundred sixty-one patients, average age 63.5±11.5 years, were enrolled in the study. The overall AL rate was 6.8% (11/161). In the univariate analysis, modified Glasgow Prognostic Score (mGPS)=2 (p=0.003), use of multiple staplers (≥3 firings) for rectal transection (p=0.001) and intraoperative bleeding (≥250 g) were significantly associated with AL incidence. Multivariate analysis identified that mGPS = 2 (odds ratio [OR]: 19.6, 95% confidence interval [CI]: 2.96-125.00, p=0.002) and multiple firings (OR: 18.19, CI: 2.31-111.11, p=0.002) were independent risk factors for AL.
Conclusion: Higher mGPS score and multiple firings were independent risk factors for AL.
Introduction
Anastomotic leakage (AL) is one of the most common and devastating complications of low anterior resection (LAR), a form of rectal cancer surgery. AL not only results in reduced quality of life and elongated hospital stay, but also adversely affects post-operative defecation and local recurrence
1
-
3)
. Identifying risk factors for AL may reduce its incidence and improve patient outcomes. Many studies have reported risk factor analyses for AL after LAR or laparoscopic LAR (L-LAR), but the results have not been consistent
4
-
12)
. In our hospital, we have employed L-LAR since 2005, and have expanded its applicability criteria gradually. Since 2014, we have been performing L-LAR for all rectal cancer cases except for T4b (UICC 7
th). The aim of the current study was to identify the risk factors of LAR, including L-LAR, associated with AL as treatment evolved at our institution.
Materials and Methods
Study population
Rectal cancer patients who had undergone LAR/L-LAR at Fukushima Medical University Hospital between April 2002 and February 2018 were enrolled in this study, regardless of whether preoperative treatments such as chemotherapy, irradiation, or chemoradiotherapy were performed. Rectal operations in which the anastomosis is located beyond the peritoneal reflection were regarded as LAR. Tumor location was determined by operative findings.
Analysis
Eleven patient- and tumor-related variables, and nine surgery-related variables were included in the analysis. The former included age (≥75, <75), sex, modified Glasgow prognostic score (mGPS 0+1 or 2, assigned on the first visit to our department. 0: serum albumin ≥3.5 mg/dl and C reactive protein <0.5, 1: either serum albumin ≥3.5 mg/dl or C reactive protein <0.5, 2: serum albumin <3.5 mg/dl and C reactive protein ≥0.5), preoperative ileus, diabetes, preoperative bowel preparation (magnesium citrate [MG], polyethylene glycol [PEG], others), preoperative treatment (neoadjuvant chemotherapy and chemoradiotherapy), tumor location (RS [rectosigmoid], Ra [rectum above the peritoneal reflection] + Rb [rectum below the peritoneal reflection]), pathological stage (0+1, 2+3+4>; UICC-TNM stage, 7
th edition), pathological T stage (Tis-T2, T3+T4; UICC-TMN stage, 7
th edition) and maximum tumor diameter (≥4 cm, <4 cm). The nine surgery-related variables were approach method (open, laparoscopic), inferior mesenteric ligation method (high ligation: IMA was ligated at its origin; low ligation: left colic artery preserved), lateral lymph node dissection, number of curtilages of the linear stapler used for rectal transaction (3≤[multiple firings], 1+2), placement of trans-anal tube, diverting ileostomy, diameter of circular stapler (≥29 mm, <29 mm), operating time (≥300 min, <300 min), and intraoperative bleeding amount (≥250 g, <250 g). We created ROC curves to identify cut-off values for tumor size, operation time, and bleeding amount. As for age, ROC area under the curve was less than 0.5, therefore we set 75 years old as the cut-off because it corresponds to the start of latter-stage elderly healthcare in Japan’s system of universal health insurance. The protocol for this study was approved (#29126) by the ethics committee of Fukushima Medical University, which is guided by local policy, national law, and the World Medical Association Declaration of Helsinki.
Surgical methods
Patients usually received bowel preparation with MS or PEG, although sodium picosulfate hydrate was used in some patients, and some patients did not receive any preparation, depending on the bowel obstruction or operator’s discretion. Total mesorectal excision (TME) or tumor-specific mesorectal excision (TSME) was performed depending on the tumor location. The rectum was transected using linear staplers or scissors after firing a purse string device. The choice of stapler varied depending on the time, operative approach and operator (Endocutter, Echelon, Powered Echelon, Curved Cutter: Ethicon Endo-Surgery, Cincinnati, OH, USA). Anastomosis was performed using a single or double stapling technique depending on the tumor location, rectal transaction method and operator’s discretion. A circular stapler (CDH, Ethicon Endo-Surgery or EEA: Medtronic, Minneapolis, MN, USA) was used for anastomosis, and the size of the stapler was chosen depending on the diameter of the rectum or colon. The air-tightness of the anastomosis was not tested routinely. A diverting ileostomy was made at the operator’s discretion. A pelvic drainage tube was inserted routinely through the posterior side of the anastomosis. In our hospital, a trans-anal drainage tube has been used since 2013 for LAR and L-LAR.
Definition of AL
AL was diagnosed by the following clinical findings: abdominal pain, fever, and pus or fecal discharge from the pelvic drainage tube. These clinical symptoms were confirmed by computed tomography, or water-soluble contrast enema. AL was classified into three grades: Grade A, requiring no active therapeutic intervention; Grade B, requiring active therapeutic intervention other than surgery; and Grade C, requiring re-operation
13)
. We considered cases that fell into Grades B and C as AL in this study, and included them in the primary endpoint analysis.
Statistical analysis
All statistical analyses were performed using IBM SPSS statistics software, version 24 (IBM, Armonk, NY, USA). A chi-square test, Fisher’s exact test, the Mann-Whitney U test, and Student’s
t-test were used for variable comparisons and analysis. A
P value of < 0.05 was considered statistically significant. To determine the factors associated with AL, multivariate logistic regression analysis was used and factors with
P values of <0.05 in the univariate analyses were included in the model.
Results
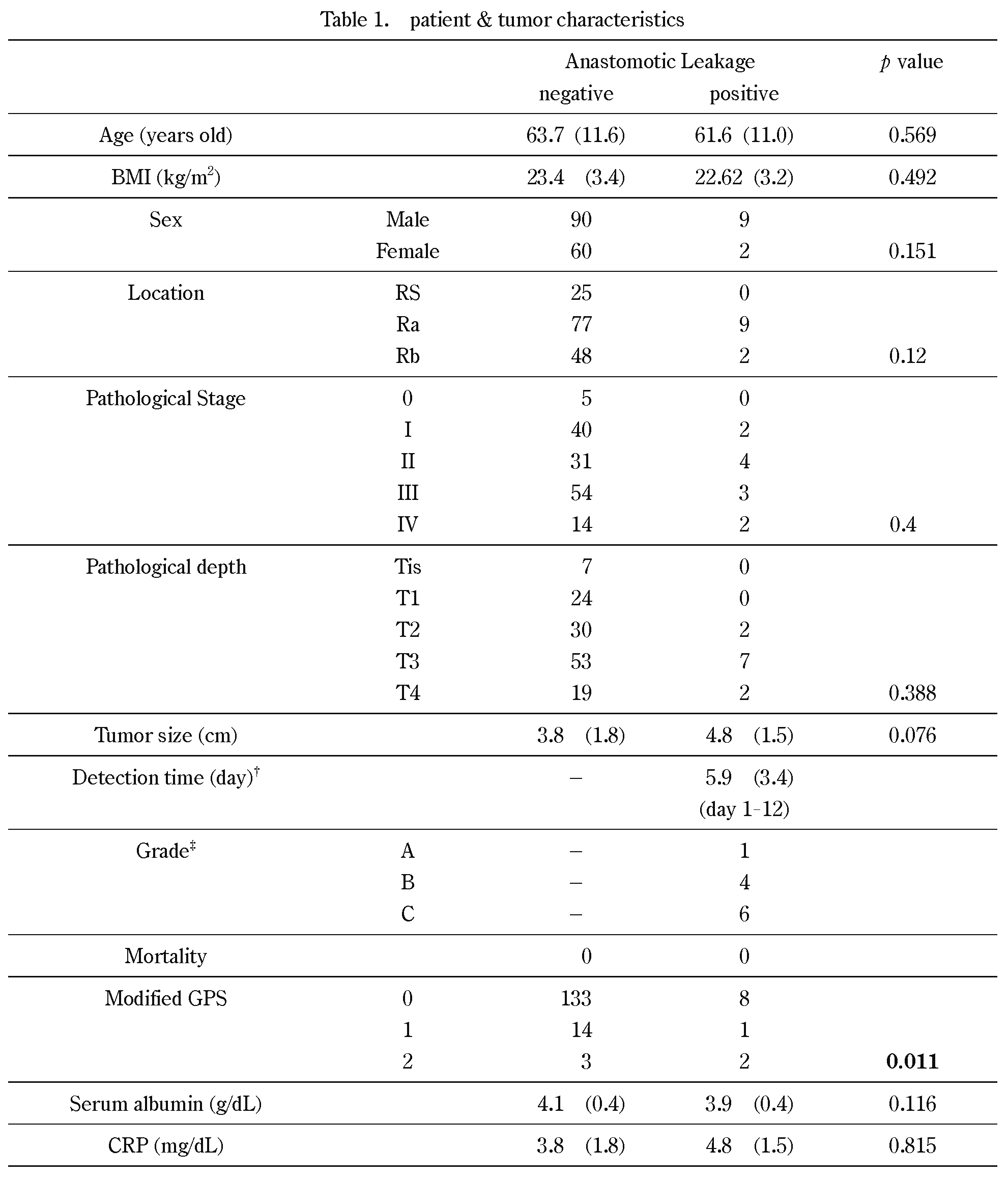
Among 161 consecutive patients enrolled in this study, 99 (61.4%) were male and 62 (38.5%) were female. The average age was 63.5±11.5 years old (range 33-88). Their average BMI was 23.3±3.3 (range 16.6-39.7). Twenty-five patients (15.5%) had RS, 86 patients (53.4%) had Ra and 50 patients (31.1%) had Rb cancer. Preoperative interventions such as chemotherapy, radiotherapy, or chemoradiotherapy, were performed in 34 patients (21.1%).
The patients and their tumor characteristics are listed in Table 1. Among the 161 patients, AL occurred in 11 patients (6.8%), nine (81.8%) of whom were male and two (18.1%) were female. AL-Grade C occurred in six cases, all of which had a diverting ileostomy. AL-Grade B occurred in five cases, all of which were cured using conservative therapy. The average time point at which AL was confirmed was postoperative day 6 (range 1-12). There were no deaths related to AL.
Patients were divided into two groups: those without AL (n=150) and those with AL (n=11). By univariate analysis, AL was significantly associated with preoperative mGPS=2 (p=0.003), operative bleeding >250 ml (p=0.001) and multiple firings (p=0.001, Tables 2 & 3). No significant associations were found with the other variables (Tables 2 & 3).
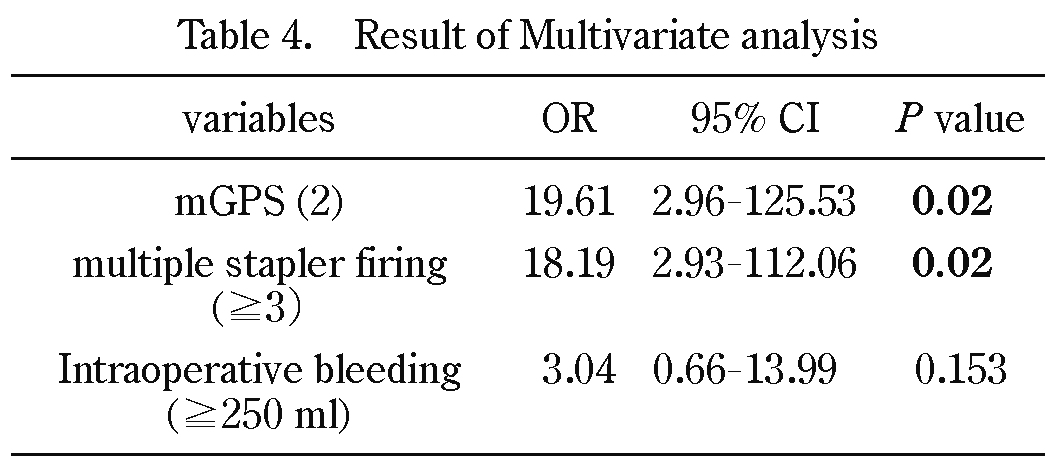
In the multivariate analysis including factors with a p value of ≤0.05 in the univariate analysis, preoperative mGPS=2 and multiple firings were significantly correlated with AL (respectively: odds ratio [OR] 19.61, 95% confidence interval [CI] 2.96-125.00, p=0.02; and OR 18.19, CI 2.31-111.11,
p=0.02, Table 4).
Discussion
This was a single institution, retrospective observation study to determine risk factors of AL after low anterior resection. The observation period of the study spanned 16 years. Even as a single institution study, many surgeons were involved; surgical devices, such as circular staplers, linear staplers, and ultrasonic scissors varied; and even the main surgical approach changed from open to laparoscopic. Even so, multivariate analysis clearly showed that mGPS and multiple firings were risk factors for AL.
In general, the rate of AL occurrence following LAR has been reported to be between 3.6 and 15.3% worldwide
14)
. Specifically, Matsubara
et al. reported an AL incidence in Japan of 9.7% by analyzing our National Clinical Database
15)
. Thus, it seems likely that our surgical quality for anastomosis, with AL=6.8% during LAR and L-LAR, is adequate. Previous studies reported risk factors for AL such as anastomosis level
4)
, tumor location
5
-
8,
16)
, tumor size
9)
, multiple stapler firings
4,
8,
10,
16)
, operation time
6,
8)
, intraoperative blood loss
11,
12)
, body mass index
7)
, male gender
8,
14)
, and preoperative chemoradiotherapy
16)
.
In the present study, risk factors for AL were identified as intraoperative bleeding, mGPS=2, and multiple firings by univariate analysis, and as mGPS=2 and multiple firings by multivariate analysis. The mGPS score is a representative inflammation-based score, combining indicators of decreased plasma albumin and elevated C-reactive protein (CRP). Many studies have revealed associations between elevated GPS/mGPS and poor prognosis in a number of malignancies, including colorectal cancer
17,
18)
. Recently, inflammatory markers, including GPS/mGPS, have also been characterized as risk factors for postoperative complications
19,
20)
. In the current study, we confirmed that mGPS=2 was a risk factor for AL. To our knowledge, this is the first report to identify high mGPS as risk factor for AL.
Elsewhere, multiple firings have been reported as a risk factor for AL
4,
8,
16)
, consistent with our analysis. Kawada
et al. posited that an increased number of stapler firings could result in small defects between the staple lines, leading to AL
14)
. The number of stapler firings for rectal transection is likely to be affected by several factors, including narrow pelvis, obesity, bleeding, and inadequate port placement. Although we evaluated intraoperative bleeding, BMI, and sex as risk factors in the present study, there were no significant associations between these factors and AL. In addition, in order to prevent multiple firings, Ito
et al. emphasized the efficacy of additional medial-suprapubic ports for transection of the rectum
4)
, and Kuroyanagi
et al. emphasized the efficacy of planned rectal transection by using two endostaplers and punching out the point at which they crossed using a circular stapler
21)
. In addition, there is a possibility that the surgical approach (open or laparoscopic) may affect the risk of AL. However, in the present study, we found that laparoscopic surgery was not a significant risk factor for AL. Potentially, robotic surgery may reduce the risk of multiple firings by stabilizing the operative field and by using a well articulating endostapler for transection of the rectum; however, to our knowledge, no study has yet been reported comparing the number of firings between robotic and endoscopic surgery.
Blood supply to the anastomosis is also thought to be an important factor for AL, and decreased blood flow is a risk factor
22,
23)
. Since it has been reported that real-time assessment of blood flow around an anastomosis with indocyanine green is acceptable
24)
, further study to objectively evaluate the blood flow is necessary.
This study has several limitations. First, the observation period of the study extended to 16 years, from 2002 to 2018. Within that period, we have introduced laparoscope-assisted surgery, anastomotic devices have evolved, and the members of our surgical team have changed several times, during which learning curves could have influenced outcomes. Even with these limitations, mGPS and multiple firings still emerged as risk factors of AL; therefore, these two may persists as risks of LAR in the future. Second, the AL cohort was relatively number (n=11). This may be a reason why other risk factors that emerged in previous reports were not extracted in this study.
In conclusion, higher mGPS score and multiple stapler firings were independent risk factors for AL. It has been suggested that improvement of mGPS score by preoperative strategies such as nutrition support team intervention and infection control, as well as single or double use of staplers for rectal transection, may reduce the AL occurrence rate.
Acknowledgements
We would like to express our gratitude to successive surgical teams, including 1st Department of Surgery, 2nd Department of Surgery, Department of Regenerative Surgery, and Department of Organ Regulatory Surgery, Fukushima Medical University for their dedicated efforts.
Conflict of Interest Disclosure
The authors declare no conflicts of interest.
References
- 1. Branagan G, Finnis D, Group WCCAW. Prognosis after anastomotic leakage in colorectal surgery. Dis Colon Rectum, 48(5): 1021-1026, 2005
- 2. Mirnezami A, Mirnezami R, Chandrakumaran K, Sasapu K, Sagar P, Finan P. Increased local recurrence and reduced survival from colorectal cancer following anastomotic leak: systematic review and meta-analysis. Ann Surg, 253(5): 890-899, 2011.
- 3. Ha GW, Kim JH, Lee MR. Oncologic Impact of Anastomotic Leakage Following Colorectal Cancer Surgery: A Systematic Review and Meta-Analysis. Ann Surg Oncol, 24(11): 3289-3299, 2017.
- 4. Ito M, Sugito M, Kobayashi A, Nishizawa Y, Tsunoda Y, Saito N. Relationship between multiple numbers of stapler firings during rectal division and anastomotic leakage after laparoscopic rectal resection. Int J Colorectal Dis, 23(7): 703-707, 2008.
- 5. Kim JS, Cho SY, Min BS, Kim NK. Risk factors for anastomotic leakage after laparoscopic intracorporeal colorectal anastomosis with a double stapling technique. J Am Coll Surg, 209(6): 694-701, 2009.
- 6. Huh JW, Kim HR, Kim YJ. Anastomotic leakage after laparoscopic resection of rectal cancer: the impact of fibrin glue. Am J Surg, 199(4): 435-441, 2010.
- 7. Akiyoshi T, Ueno M, Fukunaga Y, Nagayama S, Fujimoto Y, Konishi T, et al. Incidence of and risk factors for anastomotic leakage after laparoscopic anterior resection with intracorporeal rectal transection and double-stapling technique anastomosis for rectal cancer. Am J Surg, 202(3): 259-264, 2011.
- 8. Kim CW, Baek SJ, Hur H, Min BS, Baik SH, Kim NK. Anastomotic Leakage After Low Anterior Resection for Rectal Cancer Is Different Between Minimally Invasive Surgery and Open Surgery. Ann Surg, 263(1): 130-137, 2016.
- 9. Yasui M, Takemasa I, Miyake Y, Hata T, Ikeda M, Hasegawa J, et al. Tumor Size as an Independent Risk Factor for Postoperative Complications in Laparoscopic Low Anterior Resection for Advanced Rectal Cancer: A Multicenter Japanese Study. Surg Laparosc Endosc Percutan Tech, 27(2): 98-103, 2017.
- 10. Lee S, Ahn B. The Relationship Between the Number of Intersections of Staple Lines and Anastomotic Leakage After the Use of a Double Stapling Technique in Laparoscopic Colorectal Surgery. Surg Laparosc Endosc Percutan Tech, 27(4): 273-281, 2017.
- 11. Mäkelä JT, Kiviniemi H, Laitinen S. Risk factors for anastomotic leakage after left-sided colorectal resection with rectal anastomosis. Dis Colon Rectum, 46(5): 653-660, 2003.
- 12. Leichtle SW, Mouawad NJ, Welch KB, Lampman RM, Cleary RK. Risk factors for anastomotic leakage after colectomy. Dis Colon Rectum, 55(5): 569-575, 2012.
- 13. Rahbari NN, Weitz J, Hohenberger W, Heald RJ, Moran B, Ulrich A, et al. Definition and grading of anastomotic leakage following anterior resection of the rectum: a proposal by the International Study Group of Rectal Cancer. Surgery, 147(3): 339-351, 2010.
- 14. Kawada K, Hasegawa S, Hida K, Hirai K, Okoshi K, Nomura A, et al. Risk factors for anastomotic leakage after laparoscopic low anterior resection with DST anastomosis. Surg Endosc, 28(10): 2988-2995, 2014.
- 15. Matsubara N, Miyata H, Gotoh M, Tomita N, Baba H, Kimura W, et al. Mortality after common rectal surgery in Japan: a study on low anterior resection from a newly established nationwide large-scale clinical database. Dis Colon Rectum, 57(9): 1075-1081, 2014.
- 16. Park JS, Choi GS, Kim SH, Kim HR, Kim NK, Lee KY, et al. Multicenter analysis of risk factors for anastomotic leakage after laparoscopic rectal cancer excision: the Korean laparoscopic colorectal surgery study group. Ann Surg, 257(4): 665-671, 2013.
- 17. Wang F, He W, Jiang C, Guo G, Ke B, Dai Q, et al. Prognostic value of inflammation-based scores in patients receiving radical resection for colorectal cancer. BMC Cancer, 18(1): 1102, 2018.
- 18. Richards CH, Leitch EF, Horgan PG, Anderson JH, McKee RF, McMillan DC. The relationship between patient physiology, the systemic inflammatory response and survival in patients undergoing curative resection of colorectal cancer. Br J Cancer, 103(9): 1356-1361, 2010.
- 19. Bailon-Cuadrado M, Perez-Saborido B, Sanchez-Gonzalez J, Rodriguez-Lopez M, Mayo-Iscar A, Pacheco-Sanchez D. A new dimensional-reducing variable obtained from original inflammatory scores is highly associated to morbidity after curative surgery for colorectal cancer. Int J Colorectal Dis, 2018.
- 20. Josse JM, Cleghorn MC, Ramji KM, Jiang H, Elnahas A, Jackson TD, et al. The neutrophil-to-lymphocyte ratio predicts major perioperative complications in patients undergoing colorectal surgery. Colorectal Dis, 18(7): O236-242, 2016.
- 21. Kuroyanagi H, Oya M, Ueno M, Fujimoto Y, Yamaguchi T, Muto T. Standardized technique of laparoscopic intracorporeal rectal transection and anastomosis for low anterior resection. Surg Endosc, 22(2): 557-561, 2008.
- 22. Kawada K, Hasegawa S, Wada T, Takahashi R, Hisamori S, Hida K, et al. Evaluation of intestinal perfusion by ICG fluorescence imaging in laparoscopic colorectal surgery with DST anastomosis. Surg Endosc, 31(3): 1061-1069, 2017.
- 23. Ris F, Liot E, Buchs NC, Kraus R, Ismael G, Belfontali V, et al. Multicentre phase II trial of near-infrared imaging in elective colorectal surgery. Br J Surg, 105(10): 1359-1367, 2018.
- 24. Cahill RA, Ris F, Mortensen NJ. Near-infrared laparoscopy for real-time intra-operative arterial and lymphatic perfusion imaging. Colorectal Dis, 13 Suppl 7: 12-17, 2011.