Planning Analysis and Simulation
What Promotes Residents' Health?
Identifying the Direct and Indirect Impacts of Community Environment on Residents' Health

2024 年 12 巻 1 号 p. 117-134
詳細
2024 年 12 巻 1 号 p. 117-134
In fast-paced and high-pressure modern urban environments, the increase in chronic and psychological diseases significantly threatens public physical and mental health. The community environment is a basic unit of residents’ lives and has direct and indirect effects on their health. This study examined the daily activities of residents in 12 communities in Fuzhou City and analysed the influencing mechanism among the community environment, daily activities, and residents’ health by constructing a structural equation model. We identified the direct and indirect effects of the community environment on residents’ health and provided a reference for the construction of community environments to promote residents’ health. The natural environment had the greatest direct impact on residents’ health, and the physical environment had the greatest indirect and comprehensive impact. Daily activities had a mediating effect on the relationship between the community environment, particularly physical, and residents’ health.
In today’s society, chronic and psychological diseases are increasing and have become serious threats to residents’ physical and mental health. There is an urgent need to build an urban environment that promotes residents’ health (Yang, G. and D'Arcy, 2022). Chronic diseases account for more than 70% of the total number of deaths worldwide (Guthold, Stevens et al., 2018; Wanni Arachchige Dona, Angeles et al., 2021) and 88.5% of all deaths in China (The State Council lnformation Office of the People's Republic of China, 2020). Moreover, in the fast-paced and high-pressure urban environment, residents’ psychological and mental health problems, such as insomnia and depression, have gradually increased (Yue, Yang et al., 2022). One-fourth of the global population experiences mental health problems. By 2030, mental illness is expected to be one of the biggest health problems worldwide (Cusick, Adekkanattu et al., 2021). The prevalence of mental illness problems in China is 17.5%, with over 200 million people suffering from mental illness (Li, S., Yao et al., 2019). The consequences of chronic and mental diseases have become a serious threat to human existence (Song, Man et al., 2019). Modern medicine has shifted from passive treatment to active defence, and the creation of a healthy urban environment could help urban residents combat diseases in the future (Yang, C., Tan et al., 2022).
The community is the basic living unit of city residents. As of 2018, approximately 55% of the world’s population lived in communities (Xu, 2021). By 2050, approximately 68% of the population is expected to live in communities (Vargas López and Flores-García, 2023). Building a supportive environment for community health plays an important role in promoting residents’ physical and mental health and realizing healthy cities (Jiang, Ye et al., 2020; Li, Y., Huang et al., 2020). Building a supportive environment for community health and mobilizing positive factors in all aspects, with the physical environment providing lifestyle guidance, the natural environment providing psychological counselling, and the social environment caring for vulnerable groups, ensures public physical and mental health and helps residents increase physical activity, reduce mental pressure, and enhance their sense of community (Marriott and Hart, 2021). In the supportive environment of community health, the community environment, residents’ health, and daily activities are closely linked and influence each other (Zhao, Shen et al., 2021; Zhong and Lee, 2022).
Community physical environment is an important place for residents to live and is closely related to their physical and mental health (Ellina, Middleton et al., 2021; Huang, Yao et al., 2022; Yang, J., Tao et al., 2019). A good physical environment can promote residents’ health. Prosperous community streets, a convenient shopping environment, and open public space can encourage residents to go out for activities and improve their physical health (Pollack Porter, Prochnow et al., 2019; Porchezhian and Irulappan, 2022; Wang, H. and Cui, 2022). Good sanitary conditions and adequate night lighting can improve residents’ psychological comfort and promote their mental health (Liu, He et al., 2020; Wang, S., Li et al., 2021). The natural environment of a community is an important carrier for alleviating mental pressure on residents (Kruize, van Kamp et al., 2020; Zhang, Y., 2019). Good natural environment, such as community parks, plays an important role in reducing residents’ mental fatigue and ensuring emotional stability (Li, H., Ta et al., 2023; Pollack Porter, Prochnow et al., 2019). A high green shade ratio, diverse plant species, rich plant colours, and high street green view rates can improve the community’s environmental ecological benefits, increase the visual comfort of residents, and alleviate their psychological pressure. The fragrant air and peaceful community environment can stabilize the mood and promote mental health (Sallis, Cerin et al., 2020; Vlot‐van Anrooij, Koks‐Leensen et al., 2020). A community’s social environment is an important place for residents to acquire health knowledge and improve their health psychology (Ma and Wang, 2022). The rational formulation and effective implementation of community health policies and healthcare for disadvantaged groups can make residents experience care, consideration, and warmth, and increase their sense of social identity (Ellina, Middleton et al., 2021). Excellent community social security and close neighbourhood relationships can make residents feel safe and harmonious and enhance their sense of ownership and regional identity (Cheng and Li, 2022; Zou, Shen et al., 2023). Health education facilities and lectures are conducive to the dissemination of health knowledge and enhancement of residents’ health literacy (Ellina, Middleton et al., 2021; Ma and Wang, 2022).
Daily activities have a direct positive impact on residents’ health. Studies have shown that physically active people have lower rates, lesser severity, and later onset of cardiovascular disease (Myers, Kokkinos et al., 2021). Physical activities play a positive role in improving health and preventing disease (Zhang, Q., Gao et al., 2020). People who exercised more than four hours per week were shown to have a 69% lower risk of cardiovascular disease and a 73% lower risk of death than those who walked less than an hour per week (Bull, Al-Ansari et al., 2020). People who did moderate amounts of exercise every day had a 25% lower risk of dying than those who were sedentary (Dimitri, Joshi et al., 2020). As residents’ physical activity increases, their bodies become lighter, and their sleep quality improves (Canhin, Tebar et al., 2021; Yun, Han et al., 2021).
A good community environment, such as a community with high accessibility, comfort, complete facilities, and sufficient vitality, is conducive to the occurrence of residents’ physical activities and has a greater probability of triggering walking and communication activities. A high degree of mixed land use and street connectivity can enhance residents’ willingness to travel and provide choices for walking. Convenient walkways and fitness facilities provide the necessary conditions for community residents to engage in physical activity. Good greenery and fresh air also entice residents to walk outside.
Consequently, a good community environment can promote residents’ health. Appropriate daily activities can enhance the health of residents, and a good community environment can promote daily activities. This study examined the relationship between the community environment, physical activity, and residents’ health. Moreover, this study provides suggestions for constructing community environments to support residents’ health. We examined 12 communities in Fuzhou, China, and used a structural equation model to conduct a quantitative analysis of the community environment, daily activities, and residents’ health. We aimed to identify the influencing path and action mechanism among these relationships to provide planning strategies for community construction and renewal.
Three hypotheses were proposed based on the existing literature (Figure 1).
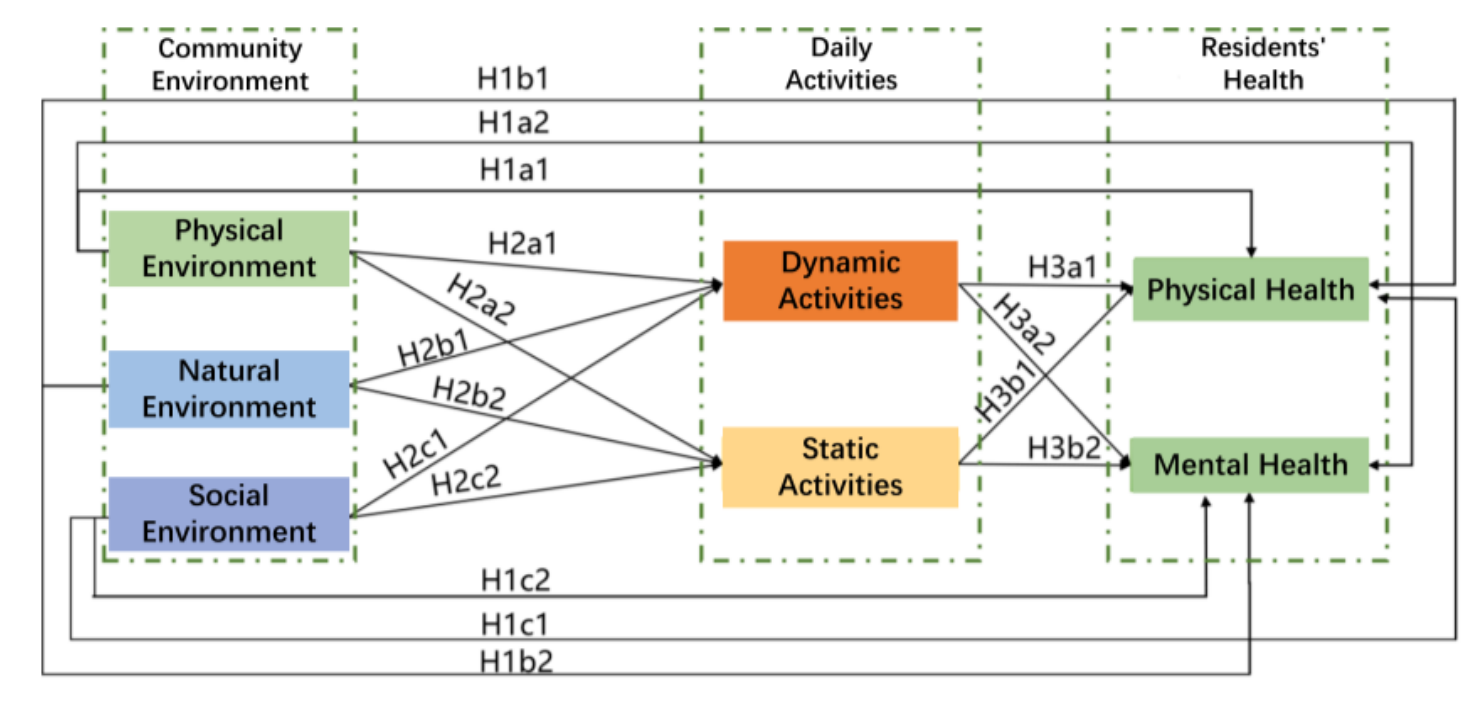
H1: Community environment has a significant direct positive influence on residents’ health. H1a1 refers to the positive influence of the physical environment on physical health; H1a2 refers to the positive influence of the physical environment on mental health; H1b1 refers to the positive influence of the natural environment on physical health; H1b2 refers to the positive influence of the natural environment on mental health; H1c1 refers to the positive influence of the social environment on physical health; and H1c2 refers to the positive influence of the social environment on mental health.
H2: The community environment has a significant positive influence on daily activities. H2a1 refers to the positive influence of the physical environment on dynamic activities; H2a2 refers to the positive influence of the physical environment on static activities; H2b1 refers to the positive influence of the natural environment on dynamic activities; H2b2 refers to the positive influence of the natural environment on static activities; H2c1 refers to the positive influence of the social environment on dynamic activities; and H2c2 refers to the positive influence of the social environment on static activities.
H3: Daily activities have a significant positive effect on residents’ health. H3a1 refers to the positive influence of dynamic activities on physical health; H3a2 refers to the positive influence of dynamic activities on mental health; H3b1 refers to the positive influence of static activities on physical health; and H3b2 refers to the positive effect of static activities on mental health.
Research sitesFuzhou was selected as the study area. First, there is a clear contradiction between the high-density development of the urban environment in Fuzhou City and the demand for a healthy living environment for the community residents, which is of practical significance in choosing this case study area. Fuzhou is characterized by a spatial pattern surrounded by mountains on three sides and facing the sea on the other side. While mountains serve as natural barriers for Fuzhou, they also hinder the city’s expansion. The entire city is experiencing a trend of cohesive development, which has led to a shortage of land for urban development and compression of living spaces for residents. Second, in recent years, Fuzhou’s municipal government has actively promoted the development of slow-moving urban systems and healthy sports venues for residents. This includes the establishment of urban ecological recreational trails, such as the Jinniu Mountain Fudao, which not only provides policy support but also creates a supportive environment for community health.
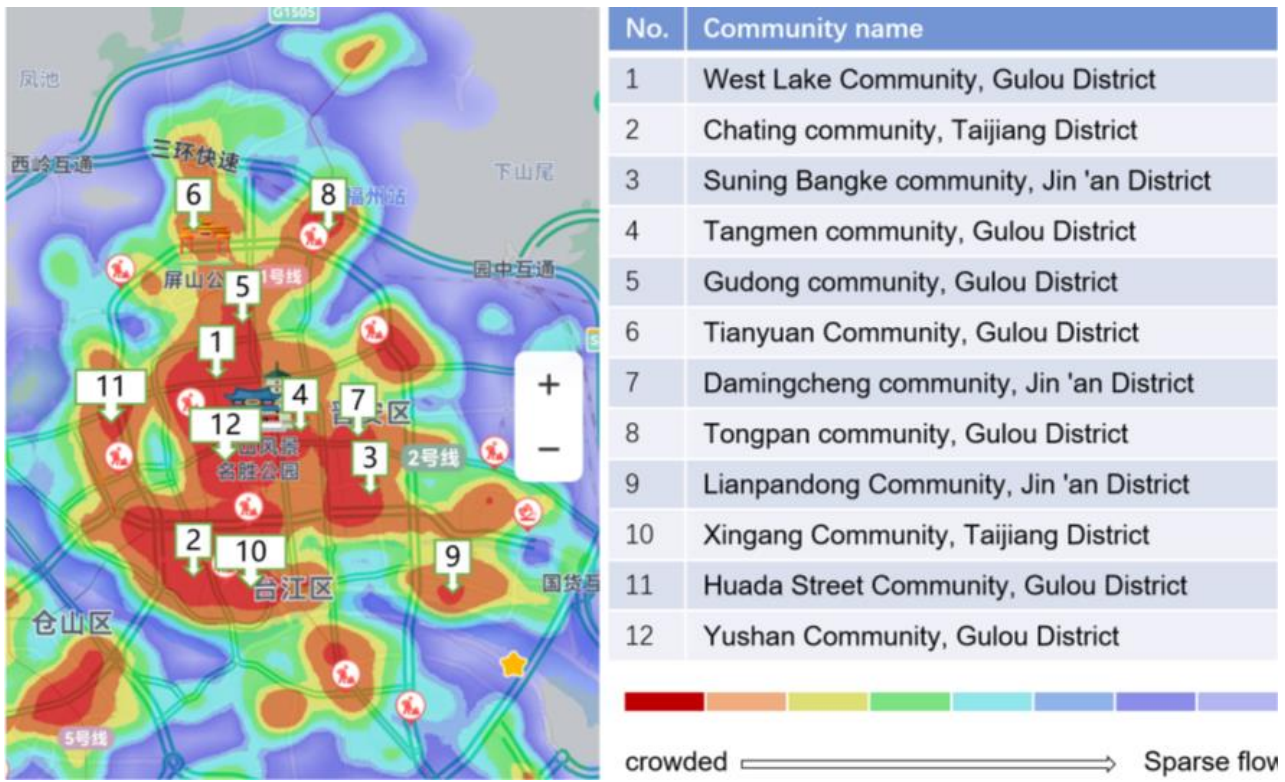
Therefore, three urban districts in Fuzhou were selected as the study areas: Gulou, Taijiang, and Jin’an Districts. At the sample community selection level, communities that simultaneously met the three conditions were selected as the initial selection (n=22). These conditions included having an occupancy rate of more than 90%, having a supporting kindergarten and elementary school in the community, and having at least one park within 500 m of the community. The selection was based on factors such as the payment for water, electricity, gas, and community support provided by the community committee. Using Baidu heat maps and on-site verification, 12 communities with high pedestrian flows were selected as sample communities (Figure 2).
The data obtained in this study were combined with data from preliminary research conducted for a settlement planning course in the urban and rural planning program at the College of Architecture and Urban Planning, Fujian University of Technology. The participants in the questionnaire survey were second-year undergraduate students (n=24) of urban and rural planning. The trainers were members of the Fujian Provincial Natural Science Foundation (grant number 2022J05192) and teachers of the settlement planning course in the College of Architecture and Urban Planning, Fujian University of Technology. The trainers provided formal training to the data collectors consisting of three parts (Table 1). Twenty-four trained data collectors were divided into 12 groups to administer the questionnaire to residents of the 12 sample communities.
| Training Steps | Training Contents |
|---|---|
| Step 1 | Detailed explanation of each questionnaire question, including examples and photos, and in-depth explanation of questions that were not common or difficult to answer |
| Step 2 | Data collection conducted pre-research in the sample community to screen out difficult questions |
| Step 3 | Comparative analysis of difficult questions to unify the calibre of the answers and improve data collection accuracy |
The study data were divided into three categories: community environment, daily activities, and residents’ health. Data were collected using a combination of online and offline questionnaires. A preliminary draft of the questionnaire was designed, and pre-research was conducted in March 2021. Ten questionnaires were distributed to each community in the sample, for a total of 120 questionnaires. Of these, 115 were returned, of which 112 were valid. Based on the results of the preliminary research, the questionnaire questions were revised to create community environment, daily activities, and residents’ health questionnaires.
The formal questionnaire survey started on September 1, 2021, and was distributed in 12 sample communities using both online and offline methods. Residents of our community who were willing to complete the questionnaire will be recruited by offering electric fans (worth RMB 3) as an incentive. Upon completing the questionnaire, residents immediately received vouchers. The online survey was conducted using Questionnaire Star (www.wjx.cn). Questionnaire Star provided a user-friendly web interface with detailed explanations of each question option. Offline surveys were conducted in high-traffic areas within the community. Data collectors were responsible for explaining the meaning of the question options either online or face-to-face. They provided examples of photographs to help the respondents understand the questions and fill out the questionnaire accurately. A total of 1209 questionnaires were distributed, with 831 online and 378 offline. Of these, 1016 valid questionnaires were collected, of which 697 were collected online and 319 offline. The efficiency rate of collecting valid questionnaires was 84.04%, with an online efficiency rate of 83.87% and an offline efficiency rate of 84.39%.
The statistical data were as follows:
Gender: Female (57%) and Male (43%).
Age distribution: 7–17 years (9.1%), 18–40 years (42.5%), 41–65 years (40.3%), and > 66 years (8.1%).
Educational background: Junior high school (15.1%), senior high school (35.2%), junior college (21.8%), undergraduate university (23.4%), and postgraduate or above (4.5%).
Occupation: students (8.5%), full-time workers (43.2%), part-time workers (15.8%), unemployed individuals (17.2%), and retirees (15.3%).
Positions: ordinary staff (65.1%), middle managers (16.4%), senior managers (3.8%), self-employed (7.6%), and other (7.1%).
The data indicated a relatively equal ratio of men to women (43:57). The majority of the participants were young and middle-aged (83%). Their educational background was primarily high school (35%), whereas the occupational group consisted mainly of full-time workers (43%). In addition, the job position was predominantly that of ordinary staff (65%).
Community environmental data collectionCommunity environmental data collection was conducted based on three main aspects (Table 2). Respondents were asked to evaluate the strengths and weaknesses of each factor on five levels (1 = very poor, 2 = poor, 3 = normal, 4 = good, 5 = very good).
| Community Environment | Corresponding Factors |
|---|---|
| Physical Environment | Travel convenience, Richness of surrounding formats, Convenience of surrounding public space, Convenience of rest facilities, Shopping convenience, Convenience of leisure and entertainment, Convenience of fitness facilities, Open degree of street building, Street environmental sanitation level, Night lighting brightness, Convenience of health cabin |
| Natural Environment | Convenience of parks, Shade degree of trees, Road greening degree, Roof greening degree, Vertical greening degree, Hydrophilicity degree, Plant species richness, Plant colour richness, Ornamental degree of water landscape, Air fragrance degree |
| Social Environment | Degree of social security, Intimacy of neighbourhood relationship, Education/ publicity efforts, Community health education popularization efforts, Community health activities to carry out efforts, Degree of implementation of health policies, Health care for vulnerable groups |
Daily activities were mainly measured from two perspectives: dynamic and static (Table 3). Respondents were asked to select their participation time (1 = 0–5 min/day, 2 = 5–15 min/day, 3 = 15–30 min/day, 4 = 30–60 min/day, 5 = 60 min/day and above).
| Daily Activities | Corresponding Factors |
|---|---|
| Dynamic Activities | Walking to and from work, Running exercise, Square exercise, Equipment exercise, Ball sports |
| Static Activities | Relaxing meditation (such as reading books and newspapers, closing one's eyes to rest one's mind), Contact with nature (such as admiring flowers, watching fish, fishing), Social activities (such as singing, opera, musical instrument performance, playing chess, playing cards) |
According to the 10 health standards of the World Health Organization, residents’ health was classified into two aspects: physical and mental (Table 4). Respondents were asked to rate their physical (1 = very poor, 2 = poor, 3 = normal, 4 = good, 5 = very good) and mental states (1 = very weak, 2 = weak, 3 = average, 4 = strong, 5 = very strong).
| Resident Health | Corresponding Factors |
|---|---|
| Physical Health | Weight, Physical and mental strength, Disease resistance, Sleep quality, Eyes, Hair, Teeth, Muscle and skin, Cardiopulmonary function |
| Mental Health | Happiness index, Psychological security, Degree of optimism in dealing with things, Mental resilience, Psychological resilience, Psychological creativity |
A five-point Likert scale was used to evaluate the data. Physical, natural, and social environments; dynamic and static activities; and physical and mental health were set as latent variables, and their corresponding factors were considered observed variables (Table 5). These variables were input into SPSS 26.0 and AMOS 21.0 statistical software for structural equation model analysis.
| Latent Variable (F) | Observational Variable (y) |
|---|---|
| Physical Environment (F1) | Travel convenience (y1), richness of surrounding formats (y2), convenience of surrounding public space (y3), convenience of rest facilities (y4), shopping convenience (y5), convenience of leisure and entertainment (y6), convenience of fitness facilities (y7), open degree of street building (y8), street environmental sanitation level (y9), night lighting brightness (y10), convenience of health cabin (y11). |
| Natural Environment (F2) | Convenience of parks (y12), shade degree of trees (y13), road greening degree (y14), roof greening degree (y15), vertical greening degree (y16), hydrophilicity degree (y17), plant species richness (y18), plant colour richness (y19), ornamental degree of water landscape (y20), air fragrance degree (y21). |
|
Social Environment (F3) |
Degree of social security (y22), intimacy of neighbourhood relationship (y23), education publicity column publicity efforts (y24), community health education popularization efforts (y25), community health activities to carry out efforts (y26), degree of implementation of health policies (y27), health care for vulnerable groups (y28). |
|
Dynamic Activities (F4) |
Walking to and from work (y29), running exercise (y30), square exercise (y31), equipment exercise (y32), ball sports (y33). |
|
Static Activities (F5) |
Relaxation meditation (y34), exposure to nature (y35), social activities (y36). |
|
Physical Health (F6) |
Weight (y37), physical and mental strength (y38), disease resistance (y39), sleep quality (y40), eyes (y41), hair (y42), teeth (y43), muscle and skin (y44), cardiopulmonary function (y45). |
|
Mental Health (F7) |
Happiness index (y46), psychological security (y47), degree of optimism in dealing with things (y48), mental resilience (y49), psychological resilience (y50), psychological creativity (y51). |
First, the reliability and validity of the data were analysed using SPSS version 26.0. The reliability and validity of the grade variable data from the questionnaire survey were analysed. The reliability of the data was tested using Cronbach’s α analysis and Corrected Item-Total Correlation (CITC) analysis. The results showed that the Cronbach’s α coefficient of the overall data was 0.812, and the Cronbach’s α coefficients of the latent and observed variables were above 0.8. The overall correlation coefficient for the project was greater than 0.5, indicating a strong correlation. Moreover, the data demonstrated high reliability. Data validity was tested using the KMO (Kaiser-Meyer-Olkin) test and Bartlett’s test of sphericity. The results showed a KMO value of 0.843. The data passed Bartlett’s sphericity test at a significance level of 0.001, indicating that they met the validity assumptions.
Next, model tests and analyses were conducted. The research data were analysed using AMOS software, and the model test utilized the maximum likelihood estimation (MLE) method to estimate the parameters of the model. The chi-square degree of freedom ratio (χ²/df), Goodness-of-Fit Index (GFI), Root Mean Square Error of Approximation (RMSEA), Comparative Fit Index (CFI), Normal Fit Index (NFI), and Adjusted GFI (AGFI) were used to determine the model fit (Table 6). The results showed that all indices were within the criteria, the degree of fit was good, and the model was ideal.
| Common Index | Criterion | Parameter Value |
|---|---|---|
| x2/df | < 3 | 1.099 |
| GFI | > 0.900 | 0.902 |
| RMSEA | < 0.050 | 0.032 |
| CFI | > 0.950 | 0.991 |
| NFI | > 0.900 | 0.972 |
| AGFI | > 0.900 | 0.935 |
Finally, a standardized path coefficient analysis of the observed and latent variables in the community health-supportive environment was conducted. The standardized path coefficient indicates the strength of the relationship and level of influence between the observed and latent variables. The T-test and P-values were used to determine whether the path coefficient between variables was significant (T > 1.96 or P < 0.05 could determine whether the path coefficient was significant).
The results of structural equation model analysis showed that the hypothesis model H2b1 (the positive impact of the natural environment on dynamic activities) (Figure 1) was not accepted, and the remaining hypothesis models were accepted (Figure 3).

Research hypothesis models H1a1, H1a2, H1b1, H1c1, and H1c2 (Figure 1 and Figure 3) were supported. The physical, natural, and social environments had significant direct positive impacts on residents’ physical and mental health (Table 7).
| Direct Influence Coefficient | Physical Health(F6) | Mental Health(F7) | Residents' Health |
|---|---|---|---|
| Physical Environment(F1) | 0.373 | 0.225 | 0.598 |
| Natural Environment(F2) | 0.239 | 0.524 | 0.763 |
| Social Environment(F3) | 0.208 | 0.222 | 0.430 |
The natural environment had the greatest direct impact on residents’ health. The physical environment had the greatest direct impact on physical health. Moreover, the natural environment had the greatest direct impact on mental health.
Community environment most important for community-based daily activitiesHypothesis model H2b1 (positive impact of the natural environment on dynamic activities) was rejected, and hypothesis models H2a1, H2a2, H2b2, H2c1, and H1c2 were supported (Figure 1 and Figure 3). The physical and social environments had a significant positive impact on dynamic and static activities, the natural environment had a significant positive impact on static activities, and the natural environment had no impact on dynamic activities (Table 8).
| Influence Coefficient | Dynamic activities (F4) | Static activities (F5) | Daily Activities |
|---|---|---|---|
| Physical Environment (F1) | 0.523 | 0.568 | 1.091 |
| Natural Environment (F2) | - | 0.572 | 0.572 |
| Social Environment (F3) | 0.437 | 0.591 | 1.028 |
The physical environment had the greatest influence on daily activities. The physical environment had the greatest influence on dynamic activities. Moreover, the social environment had the greatest influence on static activities.
Community-based daily activities most important for residents' healthThe hypothesis models H3a1, H3a2, H3b2, and H3b2 were supported (Figure 1 and Figure 3). Dynamic and static activities had a significant positive impact on residents’ physical and mental health (Table 9).
| Influence Coefficient | Physical Health(F6) | Mental Health(F7) | Residents' Health |
|---|---|---|---|
| Dynamic Activities(F4) | 0.413 | 0.318 | 0.731 |
| Static Activities(F5) | 0.324 | 0.416 | 0.740 |
Static activities had the greatest impact on residents’ health. Dynamic activities had the greatest impact on physical health. Moreover, static activities had the greatest impact on mental health.
The mediating role of daily activitiesCommunity environment indirectly impacted residents’ health through daily activities (Figure 4). Daily activities played a significant mediating role in the effect of the community environment on residents’ health.

First, the physical environment indirectly affected residents’ health through daily activities. The physical environment indirectly influenced physical (0.400[0.523*0.413+0.568*0.324]) and mental health (0.403 [0.523*0.318+0.568*0.416]) through dynamic and static activities (Figure 4).
Second, the natural environment had an indirect impact on residents’ health through daily activities. The natural environment had no impact on dynamic activities and indirectly influenced physical (0.185[0.572 × 0.324)) and mental health (0.238[0.572 × 0.416]) through static activities (Figure 4).
Third, the social environment indirectly affected residents’ health through daily activities. The social environment had an indirect influence on physical (0.372[0.437*0.413+0.591*0.324]) and mental health (0.385[0.437*0.318+0.591*0.416]) through dynamic and static activities (Figure 4).
Finally, daily activities had the greatest mediating effect when the physical environment affected residents’ health. Daily activities had the greatest mediating effect when the physical environment affected residents’ health. Daily activities were classified as dynamic and static. Among the five observed variables of dynamic activity, equipment exercise (y32), square exercise (y31), and running exercise (y30) had the largest impact. In community planning, appropriate sports venues and equipment should be arranged, and attention should be paid to the construction of community walking paths to improve the walking environment (Figure 5). Of the three observed static activity variables, the impact of exposure to nature (y35) was the greatest. In community planning, the quality of the natural environment should be improved as much as possible, including increasing the green area and species and improving the quality of the waterscape (Figure 6).


The community environment not only had a direct impact on residents’ health but also led to dynamic or static activities of residents, indirectly affecting residents’ health. Therefore, the direct and indirect effects constituted a comprehensive impact of the community environment on residents’ health (Figure 7).

Note: Direct influence coefficient = direct influence coefficient of the community environment on residents’ health (Table 7). Indirect influence coefficient = indirect influence coefficient of the community environment on residents’ health through the intermediary role of daily activities (Table 9). Comprehensive influence coefficient = direct influence coefficient + indirect influence coefficient.
The comprehensive influence coefficient of the physical environment on residents’ health was 1.401, including that of the physical environment on physical (0.773) and mental health (0.628). A change in the physical environment for one unit caused a change of 1.401 units in residents’ health. The comprehensive influence coefficient of the natural environment on residents’ health was 1.186, including that of the natural environment on physical (0.424) and mental health (0.762). A change in the natural environment by one unit caused a change of 1.186 units in residents’ health. The comprehensive influence coefficient of the social environment on residents’ health was 1.187, including that of the social environment on physical (0.580) and mental health (0.607). A change in the social environment representing one unit caused a change of 1.187 units in residents’ health (Figure 8).

The physical environment has the greatest comprehensive impact on residents’ health, which is consistent with previous findings that improving the community walking environment can promote residents’ health (Chen, Fang et al., 2017; Yuan, Wang et al., 2020). The comprehensive effects of the physical environment on physical health (0.773), social environment on physical health (0.580), and natural environment on physical health (0.424) were observed (Figure 8). The physical environment had the greatest comprehensive impact on physical health, aligning with the findings of Wang, H. and Cui (2022) that a positive physical environment can improve the walking time and frequency of residents, thus improving their health (Sallis, Cerin et al., 2020). The physical environment contained 11 observed variables, including the largest influence of street environmental sanitation level (y9), convenience of health cabins (y11), and shopping convenience (y5). Community planning should strengthen the construction of sanitation facilities, pay attention to the cleanliness of community public spaces, and enhance residents’ health awareness through health knowledge slogans to ensure that communities are equipped with at least one health cabin. Positive communities can configure multiple health cabins and increase the proportion of community commercial spaces and commercial configurations, particularly street commerce (Figure 9).

The natural environment had the greatest comprehensive impact on mental health, which was consistent with previous findings indicating that the natural environment had a positive effect on residents’ psychological rehabilitation (Shen, Ma et al., 2022). The community physical environment contained 10 observed variables, with air fragrance degree (y21), ornamental degree of the water landscape (y20), and plant species richness (y18) having the greatest influence. In community planning, air freshness can be increased by installing aromatic plants. Water landscape designs should consider not only the accessibility of the water landscape but also the self-purification function of the water body, landscape design of the water shoreline, and overall aesthetics. In landscape design, plant species should be increased based on regional characteristics and plant combination aesthetics to enhance the sense of landscape hierarchy and greenery (Figure 10).

In this study, data were obtained using a questionnaire survey, which has some limitations. First, the sample size of the questionnaire survey was limited. This study included 12 communities in Fuzhou City District. The results cannot be generalized, and further empirical studies are required to confirm the accuracy of the findings. Second, the accuracy of the research data must be improved. Uncertainties that exist in single-source data can be reduced in the future through multi-sectoral coordination and implementation of multi-data collection methods. We used cross-modal data integration technology and collaboration with public transport departments, social networking sites, community hospitals, and other platforms and integrated various types and accuracies of data related to the community environment, travel, and residents’ health. This included social media text, time series data with geo-tagging, street view images, residents’ activity trajectories, remote sensing, hospital patient information, and personal health reports. We extracted and analysed data to gain insights into the community environment, travel patterns, and health status to improve data accuracy.
Special research for specific populationThis study did not consider the differences in community residents by age. By approximately 2035, China is expected to become a society with a significantly aging population and remain in this state for an extended period. Therefore, there is an urgent need to assist older individuals in achieving healthy aging. Research on older individuals should be conducted in the following steps:
Subjective evaluations of the built environment will provide data on the level of appeal of the community environment for older individuals. This would allow for a more comprehensive analysis of the diverse health needs of older adults in relation to their community environments.
Strengthen sample practice researchThis study lacks the integration of community renewal practices based on the research results. In the future, collaboration with community management agencies should be considered when applying the analysis results to update sample communities. Firstly, to create comprehensive and multifunctional health spaces, including leisure and recreational areas, social and activity spaces, and exercise areas. Secondly, to improve health infrastructure, it is important to carefully plan the types and quantities of facilities. These facilities should be strategically arranged in layers, ensuring they are within a 5-, 10-, or 15-minute walking distance from homes. Additionally, these facilities should be designed to be friendly, safe, and conducive to good health. Finally, a variety of community health activities, such as expert consultations and health and wellness events, should be organized to effectively encourage people to engage in long-term health activities and promote a healthy lifestyle. Continuous project feedback could strengthen the optimization and correction of the community environment, promoting residents’ health and enhancing the adoption and feasibility of the research results.
Additional comparative studyCommunity residents from different regions have different health needs. The study area was limited to Fuzhou City. Further research, differentiation analysis, and comparative studies should be conducted with communities in various cities, regions, or countries.
A good community environment can promote the physical and mental health of residents, positively impacting physical activity, reducing mental stress, alleviating fatigue, and enhancing the sense of community belonging. This study takes residents' daily activities as the starting point to explore the relationship and influence pathways among the community environment, daily activities, and residents' health.
Research shows that the community environment has a direct or indirect promoting influence on residents' health. Firstly, the community environment can directly contribute to residents' health, with the natural environment having the greatest direct impact. Secondly, the community environment can indirectly affect residents' health by encouraging daily activities within the community, with the physical environment having the greatest indirect influence. Thirdly, daily activities play a mediating role between the community environment and residents' health. The mediating effect of daily activities is most pronounced when the physical environment impacts residents' health. Finally, the physical environment has the greatest comprehensive influence on residents' health.
Therefore, in the process of community planning and construction, more attention should be paid to the construction of the natural environment, such as green spaces and water systems, to enhance the ecological impact of the community environment and improve residents’ well-being. At the same time, community sports venues and walking routes should be designed in a way that attracts residents to engage in daily physical activities. The above research provides a reasonable approach to enhancing residents' health and offers practical programs and strategies for creating health-supportive environments.
Conceptualization, F.C. and J.Y.; methodology, F.C. and J.Y.; investigation, F.C. and J.Y.; data curation, F.C. and J.Y.; writing—original draft preparation, J.Y. and Y.Z.; writing—review and editing, J.Y. and Y.Z. All authors have read and agreed to the published version of the manuscript.
The authors declare that they have no conflicts of interest regarding the publication of this paper.
This research was funded by the Natural Science Foundation of Fujian Province (Nos. 2022J05192 and 2022J01937) and the Talent Construction Foundation of Fujian University of Technology (Nos. GY-Z21178 and GY-Z21177).