Abstract
Medium-chain triacylglycerol (MCT) is a type of triacylglycerol that has six or seven to twelve carbon chains. It consists of three molecules of fatty acids attached to one molecule of glycerol. Drug delivery system (DDS) is defined as a formulation to distribute drugs into the human body. The unique properties of MCTs have garnered interest in using them as excipients in DDS. Even though there are many significant effects attributed to the use of MCTs, especially in modulating the rate of drug delivery in various DDS, they are all limited and intermittent. This warrants a detailed summary of the previous studies on the use of MCTs in various DDS. Therefore, this review focuses on presenting a systematic review of previous studies on the use of MCTs in the last six years and explores the types and effects of MCTs on DDS that employ various types of delivery routes. A systematic search through PubMed, Science Direct and Scopus was performed. Keywords like “medium-chain triglycerides”, “medium-chain fatty acids”, “medium-chain triglycerides and their fractions”, “medium-chain fatty acids and their fractions”, “MCTs”, “MCFA”, “in drug delivery”, “in drug delivery system” and their combinations were used. The synonyms of the words were also used to extend the search. A total of 17 articles that met the inclusion criteria were identified. Findings from this review have identified the several MCTs and their fractions used in DDS that employed the oral/enteral, topical, transdermal, parenteral, and pulmonary routes of drug delivery. The review also highlights that the usage of MCTs in DDS results in a better transportation of drugs into the human body.
1 Introduction
Drug delivery systems (DDS) are formulations, approaches, networks, and technologies that distribute drugs to the human body to achieve desired therapeutic effects1). An effective DDS must consider several critical parameters, such as drug effectiveness and ease of administration2). Their primary goal is to deliver the correct drug dose to the correct organs in the human body2). They also regulate the rate, timing, and location of drug release in the human body. The administration of the therapeutic product, as well as the release and transport of the active ingredient of the drug across the biological membrane to the site of action, are a part of the drug delivery process. DDS employs various types of routes which encompass mouth or oral routes, topical routes, transdermal routes, and parenteral routes such as the intravenous (IV), intramuscular (IM), subcutaneous (SC), and pulmonary routes3),4). Topical drug delivery involves the direct application of a drug to the skin surface to achieve localized therapeutic effects. Transdermal drug delivery involves administering a drug to the skin to pass through the skin layers and infiltrate the bloodstream for systemic effects throughout the body5),6).
One of the active storage forms of fatty acids (FAs) and neutral lipids is triglycerides (TG), which are formed by three fatty acids (FAs) and esterified with one glycerol molecule (GLY). It is also an example of a lipid-based formulation (LBF) that serves as an excipient to enhance drug absorption7),8). The excipients or non-drug components of a formulation play a significant role in delivering the active pharmaceutical ingredient (drug) in each dosage form. Medium-chain triglycerides (MCTs) are a type of TG with six or seven to twelve carbon chains7),8),9),10),11),12),13). Caproic acid (C6:0), enanthic acid (C7:0), caprylic acid (C8:0), capric acid (C10:0), undecylic acid (C11:0), and dodecanoic acid (C12:0) are examples of MCTs11),14),15).
The MCTs include MCT fractions with their own functions. MCT fractions are medium-chain fatty acids (MCFA) produced by the hydrolysis and breakdown of the FA. MCTs are produced by the esterification of MCFAs and GLY with or without a catalyst such as zinc (Zn) or can be found in natural sources16). There are several MCT fractions, including C6:0, C8:0, C10:0 and C12:017).
MCTs are colorless to slightly yellowish, odorless, and tasteless oily liquids. They have several advantages over topical and transdermal pharmaceutical formulations, including better skin-spreading properties, skin penetration potential, emollient characteristics, solvent properties, and stability against oxidation18). Moreover, MCTs are generally recognized as safe (GRAS) after being approved by the United States Food and Drug Administration (US FDA) in 1994, indicating that they are safe for use in food, cosmetics, nutrition products, and pharmaceuticals. They are also non-toxic, biodegradable, edible, biocompatible, and biologically safe19).
In the 1950s, MCTs were regarded as a unique energy source in a variety of conditions, including pancreatic insufficiency, fat malabsorption, poor lymphatic chylomicron transport, severe hyperchylomicronaemia, as well as in total parenteral nutrition and premature infant formula11),14). They were initially used as a replacement for long-chain triglycerides (LCTs) to treat lipid absorption disorders19). MCTs have been increasingly used in food and nutrient applications because they have several advantages over LCTs, such as immediate provision of energy, high satiety, and fewer calories, all of which can contribute to controlling obesity16).
Palm kernel oil, coconut oil, cow milk, dairy fat, and milk products are natural sources of MCTs. An increasing number of MCTs have also been synthesized via chemical processes, such as esterification and interesterification reaction using an enzyme or chemical catalyst15),19),20). The synthetic MCTs are often composed mainly of C8 and C10. In industrial process, coconut oil or palm kernel oil is subjected to hydrolysis and fractionation, resulting in a first distillation fraction rich in C8 and C10. These components are then recombined with glycerol to produce synthetic MCTs oils for instance Capryol 90, Capmul® MCM and Miglyol 81221),22),23). MCTs have unique properties such as low density, small molecular size, low melting point, and being in a liquid state at room temperature, which enhance the DDS effects8),12),19). They are also used as emulsifiers in various human pharmaceutical formulations, veterinary settings, and the cosmetics industry. MCTs are also increasingly being used in food applications21).
MCTs as excipients are under investigation for their role in human metabolism, physiological responses, nutritional aspects, and in the application of lipid-based pharmaceutical dosage forms (LBF)7),8). For example, using MCTs as an excipient in LBF provides numerous benefits because they have distinct advantages over short-chain triglycerides (SCTs) and long-chain triglycerides (LCTs)7). They have a distinct transport system and are rapidly metabolized in the human body15). MCTs and other medium-chain lipids have gained popularity in recent years because of their higher drug solubility than that of the long-chain lipids8),24). In a recent study focusing on the formulation of a nanoemulsion containing celecoxib, it was found that MCTs oil can effectively solubilize highly lipophilic drugs such as celecoxib25). Similarly, in the study by Patil et al.26), Capmul® MCM, a mono-diglyceride of medium chain fatty acids (mainly caprylic and capric acid) was employed as a key component in a mucoadhesive gel formulation to enhance the solubility and permeability of amphotericin B; a highly lipophilic drug. These cases demonstrate the advantages of using MCTs in DDS as they can improve the solubility of drugs that might be a challenge in formulation processes. The chemical and physical properties of MCFAs influence their absorption and metabolism. They are also gaining popularity because of their unique bioactivities, which include lowering cholesterol levels, slowing the rate of weight gain, and increasing ketone excretion. MCTs as carrier lipids also significantly increase curcumin bioavailability27). They are highly valued in the pharmaceutical industry as excipients or drug carriers in DDS to promote a faster rate of digestion and ensure greater drug distribution.
Recently, the use of MCTs as excipients in DDS has received significant attention in the pharmaceutical industry. However, knowledge of the MCTs and their fractions and of their application in DDS is currently limited. Thus, the current systematic review summarizes all studies from 2017 to 2022 related to MCTs and DDS, to study the types, uses, and effects of MCTs on various DDS routes.
2.1 Search strategy
This review used a substantial literature search from 2017 to 2022 to determine the types and effects of MCTs on the efficacy of the various routes employed by the DDS. This study was conducted in accordance with the PRISMA statement criteria. A thorough examination of the studies was performed using the PubMed, Science Direct, and Scopus electronic databases to ensure a broad coverage of research studies and journals. To ensure relevance, keywords such as “medium-chain triglycerides,” “medium-chain triglycerides and their fractions,” “in drug delivery,” “in drug delivery system,” and a combination of these terms were used. To broaden the search, MeSH terms such as “medium-chain fatty acids,” “medium-chain fatty acids and their fractions,” “MCTs,” “MCFA,” “MCTs and their fractions,” “MCFA and their fractions” were used. EndNote 20 software was used to screen the related articles. Duplicate papers were discarded. The reference lists of the included papers were also screened for additional relevant studies.
2.2 Inclusion and exclusion criteria
Articles were screened using the inclusion and the exclusion criteria. The inclusion criteria included: i) English language papers published between January 2017 and December 2022, ii) original articles containing MCT-related information, and iii) research on MCTs and their fractions and their relationship with DDS. The exclusion criteria included: i) articles unrelated to MCTs and DDS, ii) non-English articles, and iii) review papers.
2.3 Study selection
The search was conducted using keywords and databases. As a preliminary measure, the inclusion and exclusion criteria were applied to the titles and abstracts of the search results. Thereafter, complete text of the papers that satisfied the inclusion criteria was evaluated to determine its suitability for this review.
2.4 Data extraction
The data from the included articles were extracted and summarized in four tables according to the various routes employed by the DDS. The tables mainly comprised: i) the author and the year of publication, ii) the types of MCTs used, iii) the technique/method, iv) the formulation, v) the outcome measures, and vi) the results.
3.1 Search results
A total of 409 potentially relevant articles were identified through a thorough search of electronic resources. Subsequently, 63 duplicate articles were excluded from the review. The titles and abstracts of the remaining 346 papers were evaluated, and 190 papers were excluded based on the exclusion criteria. Seventeen articles met the inclusion criteria and were included in the final analyses. Nine of the 17 selected publications referred to the oral/enteral route, two to the topical route, three to the transdermal route, two to the parenteral route, and one to the pulmonary route. These are presented in Tables 1, 5, 7, 8, and 9, respectively.
3.2 Identification of the MCTs and MCT fractions used in the DDS
A total of 17 articles summarized the types of MCTs and MCT fractions in DDS. MCTs that were identified are Captex® 8000 (C8T), Miglyol 812N, Captex 300, Capmul® MCM C8 EP, Neobee@1053, Capryol® 90, capric/caprylic triglycerides and trilaurin. Several of these MCTs structure are shown in Fig. 1. MCT fractions that were utilized in this study were caprylic acid (C8:0), capric acid (C10:0), sodium (Na) decanoate (fatty acid anion C10:0), and lauric acid (C12:0).
3.3 Effect of the MCTs on the DDS
A total of 17 articles were included in this study and the effects of MCTs on the DDS employing different types of routes were summarized. Nine articles discussed the effects of the MCTs on the oral/enteral route (Table 1). A study conducted by Garcia et al.28) showed that the use of MCFAs to temporally disrupt the tight junctions of the gastrointestinal tract (GIT) allowed a better drug transport. An in vitro study using an intestinal cell-based model, Caco-2/HT-29, evaluated the complexation of insulin glulisine, an insulin analog administered subcutaneously (SC) or intravenously (IV) in clinical practice. Lauric acid (C12) was used as an MCT to modify the cell-penetrating peptides (CPPs). Four complexes were formed with the amphiphilic lipopeptides: C12-r4 (n=1), C12-r6 (n=2), C12-r8 (n=3), and C12-r12 (n=5) (Fig. 2). The numbers in parentheses (n) represented the number of repeats, whereas r4, r6, etc. represent repeats of a certain structural unit. As an outcome measure, transepithelial electrical resistance (TEER) is evaluated as a quality indicator of cell monolayer integrity. In this study, TEER values were measured at 0, 2, and 24 h to monitor the membrane disruption. The complexes formed with the four lipopeptides had different effects on Caco-2/HT-29 cell monolayers. For the complex formed with C12-r12, the TEER decreased from 100% to 53 and 42% at 2 h, and to 32 and 30% after 24 h for molar ratios of 4:1 and 8:1, respectively. Next, for the complex C12-r8, the TEER reduced from 100 to 97 and 74% in 2 h and decreased to 67 and 49% in 24 h for the 4:1 and 8:1 molar ratios, respectively. Meanwhile, the complex formed with C12-r6 decreased the TEER after 2 h at the higher molar ratios tested; however, none of the values fell below 75%. At 24 h, only the molar ratio of 4:1 maintained TEER at approximately 100%, whereas the remaining formulations maintained a decreased TEER. Complex C12-r4 with molar ratios of 32:1 and 1:1, registered a notable reduction in TEER after 2 h, followed by a recovery of this parameter at 24 h, whereas the molar ratios of 8:1 and 4:1 showed a gradual increase in TEER over 24 h, up to 110 and 120%, respectively. From these results, it can be deduced that complexes formed with longer oligoarginines, such as C12-r12 and C12-r8, have a more pronounced effect on TEER than that by the others. Complexes C12-r4 and C12-r6 markedly increased the glulisine transport across the Caco-2/HT-29 monolayer at molar ratios of 1:1 and 4:1, respectively. This was because the effects of C12-r6 and C12-r4 on the cell monolayer were not as harmful as those of the arginine-rich peptides. This observation was reflected in the reduction in TEER, which was not below 75% in any case and was recovered or maintained in most cases.
Table 1
Overview of included studies (oral/enteral route).

Table 1
Continued.


A study by Bunchongprasert et al.22) investigated the cytotoxicity effect of Capmul® MCM which is a C8/10 mixture of medium-chain mono- and di-glycerides (MD) in a self-emulsified nanoemulsion (SENs). This study used Captex®8000 (C8T) as the MCTs. The SEN composition consists of lipid mixtures such as C8T or soybean oil (C18T) with Kolliphor®RH40 at different ratios producing SEN1, SEN2, SEN3, SEN4, and SEN5. The composition of each SEN is presented in Table 2. A comparison of SEN1 and 2 with SEN5 and 6 was performed to investigate the effects of both C18T and C8T on the toxicity of C8/10 MD. As an outcome measure, cell viability (%) was determined to detect cytotoxicity. The results showed that SEN2 had a higher viability of 147.57±34.42% than SEN1 with 104.00±23.56%. Meanwhile, SEN5 and SEN6 has a lower viability (58.58±21.70% and 48.43±17.67%) than that of SEN1 and SEN2. Thus, this study proved that presence of triglycerides (mainly MCTs C8) in nanoformulations has the potential to reduce the toxicity effects of Capmul® MCM (C8/10MD).
Table 2
SEN composition SEN 1 and 2 has triacylglycerols in it while there is no inclusion of triacylglycerols in SEN 5 and 6.

Another study carried out by Liu et al.29) deduced that the nanoemulsions fabricated using MCTs as carrier lipids were more appropriate for delivering pterostilbene than that by the LCTs. In this study, nanoemulsions were subjected to in vitro digestion using a model simulating the GIT. Mixed micelles were obtained and analyzed for intestinal epithelial permeability using a Caco-2 cell monolayer model. In this study, MCTs, such as caprylic acid (C8:0), capric acid (C10:0), sunflower oil (C18:1), and olive oil (C18:2), were used as carrier lipids to fabricate nanoemulsions for the delivery of pterostilbene. Various outcomes satisfied the proposed objective of this study. The in vitro digestion of pterostilbene-loaded nanoemulsion showed a higher FA release of MCTs (96.0±1.1%) than that of sunflower oil (33.8±1.9%) and olive oil (30.4±0.7%). Besides that, the bioaccessibility of pterostilbene in MCTs micelles was appreciably higher (98.7±3.9%) than that in sunflower oil (41.3±0.4%) and olive oil (32.9±1.9%). Moreover, the apparent permeability coefficients (Papp) were determined to assess the Caco-2 cell monolayer permeability of the pterostilbene-loaded nanoemulsions. The findings showed that pterostilbene in micelles obtained by the digestion of MCTs had the highest Papp (8.21±2.09*10–6 cm s–1), followed by sunflower oil (5.34±0.81*10–6 cm s–1) and olive oil (5.06±1.25*10–6 cm s–1). These results can be attributed to the higher solubility of pterostilbene in MCTs than that in the LCT. Finally, the saturation concentration of pterostilbene in different lipids was also studied and showed a higher saturation solubility of pterostilbene in MCTs (242.4±10.1 mg g–1) than in the other lipids like sunflower oil (100.4±3.2 mg g–1) and olive oil (98.5±3.7 mg g–1). Therefore, it can be concluded that MCTs as carriers are more effective in pterostilbene delivery than the LCTs.
Additionally, Luo et al.30) affirmed that the MCTs incorporation could be promising in liposome production to achieve a stable drug loading. The study uses multiple methods to assess the MCTs effects such as in vivo design for pharmacokinetics study and MTT assay to assess cytotoxicity. A model drug clarithromycin (CLA) was loaded into lipid dispersions with MCT/phospholipid ratios of RM/P=0, 0.5, 1.75, and 7.5 w/w. The purpose of this investigation was satisfied through several findings. First, the characterization of dispersions with different RM/P was measured under several conditions, such as particle size and distribution (PSD), polydispersity index (PDI), and zeta potential (ZP). Table 3 presents the results of the study. From the table, it can be seen that the higher incorporation of MCTs gradually increased PSD and significantly decreased the PDI and ZP values. This indicates that the MCTs produce a homogenizing effect on the particle size (PS) and mask the negative charges on the surface of the particles. Moreover, the incorporation of MCTs also allows for a better tolerance to thermal sterilization to effectively improve the physicochemical stability, particularly when RM/P=1.75 w/w. No changes were detected in the PSD or ZP values of the MCT-containing particles. Moreover, the inclusion also led to multiple benefits for drug loading. In the high-temperature test, due to the incorporation of high MCTs (RM/Pabove 1.75 w/w), the degradation and separation of the phospholipids from lipid particles was inhibited to maintain the intact liposomal structure at high temperatures and substantially improve freeze-thaw stability. The area under the curve (AUC) and half-life (t1/2) decreased, while the total body clearance of CLA increased. In addition, no significant cytotoxicity or biocompatibility was observed. Thus, it can be deduced that the MCTs incorporation could offer promising benefits in the process of liposome production to achieve stable drug loading.
Table 3
Colloidal properties of different dispersions.

In another study, Liu et al.31) proposed that monoacyl phosphatidylcholine (MAPC) in combination with MCTs could effectively deliver oral insulin. In this simulation, MCTs such as Miglyol 812N (glyceryl tricaprylate/tricaprate), Captex 300 (glyceryl tricaprylate/tricaprate), and Capmul® MCM C8 EP (glyceryl monocaprylate) were used as a permeation enhancer (PE) in self-emulsifying drug delivery systems (SEDDS) in combination with other PEs. The SEDDSs used in this study are listed in Table 4. Several characteristics were assessed to determine the effectiveness of PE formulations. These methods include in vitro lipolysis for intestinal digestion of MCTs (MAPC) emulsion using Caco-2/HT29 and Caco-2 monolayers, and an in vivo study design using Sprague Dawley (SD) rat models. Consequently, the MCTs (MAPC) generated larger emulsion droplets approximately 200–470 nm compared to those by the MCTs (RH40) formulation which were approximately 50–150 nm in size. A higher PDI of 0.5, lower ZP value of –8 mV, and TEER value of >80% were also detected. Ins-SPC loaded MCTs (RH40) and MCTs (MAPC) formulation induced a significant reduction of blood glucose level by 17±3% and 24±11%, respectively at 0.5 hours (p<0.05). Thus, these results satisfied the proposed aim that the formulation containing MCTs in combination with natural PE, such as MAPC and synthetic PEs, can be considered a potential candidate for effective oral insulin delivery.
Table 4
SEDDS composition. The first two formulations contain MCTs and the last formulation contains LCT. All these formulations were loaded with insulin and 4% or 8% w/w of phosphatidylcholine (SPC), producing insulin-phosphatidylcholine (ins-SPC).

Three studies explored the effects of MCTs on the DDS. Firstly, a study by Grüne et al.23) evaluated whether phosphatidylcholine-based formulations have suitable properties for liquid filling in hard capsules. The suitability of phosphatidylcholine was tested using ethanol evaporation and dual centrifugation. Phosphatidylcholine-based formulations were blended with liquid formulations containing MCTs, such as Miglyol 812 (glyceryl tricaprylate/tricaprate), and binary and ternary formulations. By conducting various tests like viscosity, stringing, brittleness, integrity, and oxidative stability tests, the results favored the purpose of this research that phosphatidylcholine-based formulations containing MCTs are advantageous.
In addition, another study by Hossain et al.32) was conducted to examine the impact of bile compositions on the membrane incorporation ability of three PEs such as MCTs like caprylate (C8), caprate (C10), and salcaprozate sodium (SNAC) using coarse-grained molecular dynamics (CG-MD). An in silico study was conducted using quartz crystal microbalance with dissipation (QCM-D) and total internal reflection fluorescence (TIRF) microscopy. By studying the interaction of PEs with intestinal fluids (IFs), it was noted that free caprate monomers are more available in fasted-state fluids (FaSSIF) than in fed-state fluids (FeSSIF). Caprylate and caprate incorporated into the membrane in the presence of FaSSIF were 1.7 to 2.6-fold higher than those incorporated in the presence of FeSSIF. Moreover, QCM-D showed that the amount of incorporated caprate in FaSSIF was two times higher than that in FeSSIF. As for membrane diffusivity, caprylate and caprate diffused two-to-three-fold greater when incorporated with FaSSIF than that with FeSSIF. Therefore, it can be concluded that the ability of caprylate and caprate to perturb the membrane can be increased by alteration in bile composition.
Lu et al.33) studied the stability and in vitro digestion of curcumin encapsulated in different milled cellulose particle-stabilized Pickering emulsions. Curcumin was added to oils such as Neobee@1053, which is a caprylic/capric triacylglycerol, soybean oil, and canola oil at 8 mg mL–1 and mixed with freshly prepared milled cellulose suspension forming curcumin-loaded Pickering emulsion. An in vitro digestion technique using a pH-state lipolysis model was employed in this study. It monitors the amount of free fatty acids (FFAs) released over time. Subsequently, Pickering emulsions droplets with MCTs, canola, and soybean oil had a volume mean diameter of 46±12 μm, 27±8 μm, and 41±11 μm, respectively. The curcumin encapsulated in Pickering emulsions exhibited an encapsulation of 81.5±3.5%, 80.1±2.6%, and 82.5±2.5% in MCTs, canola, and soybean oil, respectively. More than 85% of the MCTs were converted to monoglycerides and FA after 40 min of digestion under fed-state digestion, indicating that the release of FFAs from emulsions with MCTs was much faster and higher. Hence, this study proves that the digestion of emulsions with MCTs is effective and independent of the bile salt concentration.
Another study by Wang et al.34) proposed the development of a self-microemulsifying drug delivery system (SMEDDS) to evaluate the oral bioavailability and hypolipidemic activity of dihydromyricetin (DMY). The SMEDDS was composed of a caprylic oil phase, Tween 80 as an emulsifier, and PEG 200 as a co-emulsifier. It was then loaded with DMY to produce DMY-SMEDDS. High-performance liquid chromatography (HPLC) and in vivo evaluation were performed using SD rats. A 2.34 times higher oral bioavailability than DMY, higher solubility, lower PDI value of 0.160±0.01 and a ZP value of 17.37±0.09 mV, 98% entrapment efficiency (EE), higher in vitro dissolution rate and plasma drug concentration of 2.23±0.19 μg mL–1 which was higher than rats taking oral free-DMY indicates that the combination of SMEDDS containing MCTs with DMY is a potential way to treat hyperlipidemia.
Zoubari et al.35) examined the influence of lipid carrier type and lipid drug solubility on the in vitro drug release from lipid nanoparticles for the topical route (Table 5). Dexamethasone and diclofenac sodium drugs were combined with different lipids such as Gelucire® 50/13 and Witepsol® S55 (a solid lipid), and Capryol® 90 (liquid lipid). The lipid combination produced five formulations, namely F1, F2, F3, F4, and F5, using the high-shear homogenization technique. The compositions of the lipid formulations are listed in Table 6. It was found that dexamethasone and diclofenac sodium had a higher solubility in Capryol® 90 (approximately, 9.33±0.22 and 42.37±0.25, respectively) as compared to that in the other lipids. A smaller PS and a narrow PDI of 0.13 were detected when tested with F5 since F5 formulation contains Capryol® 90 as a co-emulsifier due to its hydrophilic-lipophilic balance of 6. A combination of lipid phases such as 8:1 ratio of Gelucire 50/13 and Capryol® 90 resulted in an EE of >90% for both drugs. Hence, from this study it can be concluded that the inclusion of MCTs (Capryol® 90) results in a less organized lipidic structure and resulted in a faster drug release.
Table 5
Overview of included studies (topical route).

Table 6
Lipid formulations composition. Formulation F4 Capryol® 90 which is a MCTs while formulation F5 is the combinations of all lipid types.

De Souza et al.36) studied the preparation and characterization of nanostructured lipid carriers (NLC) containing vitamin E (NLC-VE). An in vitro study design using the emulsion solidification technique was used to prepare the particles. NLC-VE were prepared using MCTs (C8/C10) as a liquid lipid at a 1:3 mass ratio of the solid lipid-to-liquid lipid phase. This study showed that smaller particles were obtained from MCTs (21±nm) and the smallest particles were produced from coconut oil (16±1 nm). The particles obtained from MCTs released the highest quantity of vitamin E within 24 h (50%). Consequently, the NLC prepared using MCTs have the potential to effectively deliver more vitamin E within a day.
Three studies discussed the effects of MCTs on the transdermal route (Table 7). A study conducted by He et al.37) established a solid theoretical and practical framework for the development of stable and transdermal formulations of an indirubin microemulsion-based hydrogel (IR-ME gel) utilizing MCTs (capric/caprylic triglycerides) oil as the oil phase. Indirubin (IR) has shown efficacy in treating psoriasis with a low risk of side effects; however, its poor solubility and bioavailability limit its therapeutic potential. In this study, MCTs was selected as the excipient oil phase, castor oil polyoxyethylene ether (Cremophor EL) was used as the surfactant, and PEG-400 was used as the emulsifier. Carbomer 394 (1%) was used as a gelling agent to modify IR-ME into an IR-ME gel. By constructing a pseudo-ternary phase diagram, researchers optimized a microemulsion system consisting of MCTs in a 2:8 ratio with a mixed surfactant. In this optimized system, the average particle size of IR-ME was measured to be 84.37 nm, with a PDI below 0.2 and a ZP between 0 and –20 mV. After 24 h in vitro penetration profile using Franz diffusion cell apparatus, the transdermal flux/skin retention for both IR-ME and IR-ME gel was 47.34±3.59 μg cm–2/8.77±1.26 μg cm–2/ and 39.01±3.21 μg cm–2/6.5±0.6 μg cm–2 respectively as compared to medicinal olive oil solution (22.21±2.14 μg cm–2/4.18±0.79 μg cm–2) and aqueous solution (3.60±0.11 μg cm–2/2.68±0.36 μg cm–2). These findings provide further evidence that MCTs play a significant role in improving the solubility and permeability of IR.
Table 7
Overview of included studies (transdermal route).

A study by Gu et al.21) used MCTs to enhance the transdermal penetration of nanoparticles (NPs) loaded with triptolide (TPL) for transdermal delivery, including nanostructured lipid carriers (NLC) and lipid nanoparticles (SLN). The optimal TPL-NLC formulation consisted of TPL, Compritol 888 ATO, Capryol 90, Tween 80, Transcutol HP, soy lecithin, and redistilled water that were combined in the following ratios: 1:7.56:1.71:18.54:6.14:0.33:121. TPL-SLNs, on the other hand, had the same components as TPL-NLCs, but without Capryol 90, with a ratio of 1:9.27:18.54:6.14:0.33:121. As a result, the size and PDI for TPL-NLC and TPL-SLN were 139.6±2.53 nm, 104.0±1.82 nm, and 0.280±0.025, 0.278±0.018, respectively. Besides, ZP of TPL-NLC and TPL-SLN was –36.7±1.39 mV and –38.8±1.49 mV, respectively. The EE in TPL-NLC was higher (97.15±9.46%) as compared to that in TPL-SLC (92.81±8.52%) probably due to the addition of Capryol 90, which contains medium chain monoglyceride in TPL-NLC that help in NLC loading higher quantity of drug. In addition, TPL-NLC exhibited a higher transdermal flux (79.51±9.64 μg cm–2) in the 12 h in vitro permeation study, whereas TPL-SLN achieved a lower flux of only (53.94±5.72 μg cm–2). This may be related to the higher DL% and added liquid lipid (Capryol 90, which can potentially loosen SC in a manner similar to other surfactants) in the TPL-NLCs. Qing et al.38) used Capryol 90 as the excipient oil phase in a transdermal nanoemulsion formulation to solubilize Capryol 90 in sulconazole. Sulconazole nanoemulsions (SCZ-NEs) that consist of NE1-NE5, were prepared by a spontaneous titration method, and the optimized NE1 was obtained using a central composite design (CCD). Based on the findings, NE1 exhibited the smallest particle size (54.2±3.4 nm), lowest PDI (0.205±0.02), and a better ZP (23.2±1.2 mV) than those of the other NEs. Moreover, NE1 also exhibit higher percentage of EE with 87.1±3.2%. An in vitro skin permeation study confirmed that the cumulative permeability of the optimized NE1 was approximately 1.7-fold higher than that of the commercial reference miconazole (MCZ) cream and 3-fold higher than that of the SCZ solution. These studies suggest that Capryol 90 plays a significant role in improving the performance of these formulations for transdermal drug delivery.
For the parenteral route (Table 8), Li et al.39) investigated the in situ phase transition of microemulsions for parenteral injection, yielding lyotropic liquid crystalline carriers of the antitumor drug bufalin (BUF). A pseudo-ternary phase diagram of the oil (O) /surfactant (S) /water (W) system contained capric/caprylic triglycerides (MCTs) and a co-surfactant blend of macrogol (15)-hydroxystearate (Solutol HS 15) and sorbitan monooleate (Span 80). Two compositions with different MCTs oil contents were selected from the pseudo-ternary phase diagram: B-LC-ME-BUF and C-LC-ME-BUF carriers. The pseudo-ternary phase diagram is shown in Fig. 3. The B-LC-MEBUF and C-LC-ME-BUF formulations showed smooth release curves with similar trends. Meanwhile, the cumulative release of BUF after 96 hours in the C-LC-ME-BUF and B-LC-ME-BUF sample was 48.3±2.8% and 67.9±3.1%, respectively. Additionally, the C-LC-ME-BUF formulation enhanced the apoptosis of A549 cells by approximately 53.97% compared to that by the B-LC-ME-BUF formulation (39.44%). The AUC0-τ, AUC0-∞ and t1/2 of the C-LC-ME-BUF are 22.28 μg mL–1h–1, 27.60 μg mL–1h–1, and 7.87 h, respectively, which is higher than those of the free BUF. Thus, this study confirms that MCTs oil usage delivers an effective BUF release.
Table 8
Overview of included studies (parenteral route).


Khan et al.40) investigated the potential of carbamazepine-loaded nanostructured lipid carriers (CBZ-NLCs) for improved brain delivery. CBZ was loaded with NLCs such as trilaurin and oleic acid as a binary system along with the surfactants Poloxamer 188, Tween 80, and Span 80, forming formulations F1, F2, F3, F4, and F5. The trilaurin content was higher than the oleic acid content in all five formulations. The formulation F3 was selected for further evaluation of physicochemical properties, in vitro release, in vivo brain kinetics, and anticonvulsant and anxiolytic activities. The F3 CBZ-NLC produced average PS of 97.7±1.2 nm, PDI value of 0.27±0.04, ZP of –22±1.5 mV, incorporation efficiency (IE) of 85%, and a drug loading capacity (DLC) of 4.26%. The aqueous solubility of CBZ also increased 7.89-fold from 113 μg mL–1 to 892 μg mL–1. Moreover, the brain enhancement factor of CBZ increased by 1.35–5 fold along with increased anxiolytic effects. Thus, this study concluded that CBZ-NLCs present a promising strategy to improve brain delivery and therapeutic outcomes of CBZ in epilepsy.
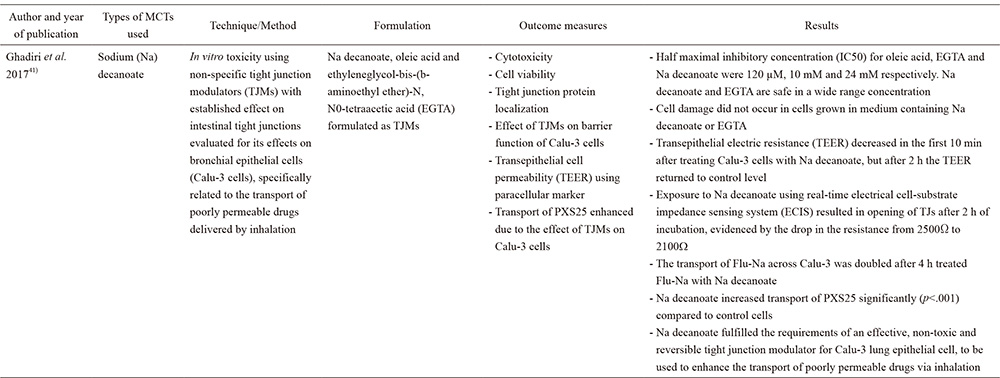
Finally, for the pulmonary route (Table 9), research done by Ghadiri et al.41)studied the effect of nonspecific tight junction modulators (TJM) on the transepithelial transport of poorly permeable drugs across airway epithelial cells. Sodium (Na) decanoate, oleic acid, and ethyleneglycol-bis-(b-aminoethyl ether)-N, N0-tetraacetic acid (EGTA) are formulated as TJMs. The prepared TJMs were subjected to in vitro toxicity evaluation using bronchial epithelial cells (Calu-3 cells). The half-maximal inhibitory concentrations (IC50) for Na decanoate, oleic acid, and EGTA were 24 mM, 120 μM, and 10 mM respectively, indicating that there was no damage to the cells grown in the medium containing Na decanoate or EGTA. The TEER values dropped from 2500 to 2100 Ω when tight junctions were exposed to Na decanoate. The permeation of sodium fluorescein (Flu-Na), a paracellular marker, across Calu-3 cells doubled after treatment with Na decanoate for 4 h. Na-decanoate also significantly increased the transport of PXS25 (an antifibrotic compound) (p<0.001) compared to that by the control cells. Thus, this study confirmed that Na decanoate, an MCT, enhanced the transport of poorly permeable drugs via inhalation.
Table 9
Overview of included studies (pulmonary route).
4 Discussion
The use of MCTs as an excipient in the pharmaceutical industry has been significantly investigated for the past years7),8). Several studies have been conducted to investigate the MCTs and its effects in DDS. Thus, this systematic review summarizes the studies on types and effects of MCTs and their fractions in DDS over the last 6 years. This systematic review mainly focuses on oral/enteral, topical, parenteral and pulmonary routes that are presented in the DDS.
4.1 Selection of MCTs and MCT fractions in DDS
All routes selected for this systematic review included the presence of MCTs and MCT fractions in the DDS. For example, in the oral/enteral route, Captex®8000 or caprylic acid or caprylate (C8), capric acid or caprate (C10), and C12 were used. Several synthetic MCTs were also widely used, such as Miglyol 812N and Captex 300 as glyceryl tricaprylate/tricaprate, Capmul® MCM C8 EP as glyceryl monocaprylate, and Neobee@1053 as caprylic/capric (C10/C8) triacylglycerol. Capryol® 90, a liquid lipid, was used to study the effect of MCTs on the topical and transdermal routes. For the parenteral route, caprylic/capric (C10/C8) triglycerides and trilaurin (C12C12C12) was used whereas for the pulmonary route, sodium (Na) decanoate was used as the MCT fraction to study their effects on the DDS.
Natural sources of MCTs and their fractions included coconut oil, palm kernel oil, and bovine milk16). Coconut oil consists of 46–54% of C12, 5–10% of C8, and 5–8% of C10. Similarly, 45–50% of C12, 3–5% of C8, 3–4% of C10 and 0.1–0.5% of C6 is found in palm kernel oil. However, the amount of MCFAs present in milk fat is very low with C12, C10, C12, and C6 constituting approximately 2.5–4%, 1.5–3.5%, 0.5–1.6%, and 0.5–3.0%, respectively. In bovine milk, C6, C8, and C10 acids constitute approximately 4–12% whereas C12 constitutes approximately 3–5% of the total FAs16). A study by De Souza et al.36) for topical DDS used coconut oil as MCTs to study NLC for vitamin E transportation since it is a natural source of MCTs and their fractions. The use of coconut oil resulted in effects similar to those of MCTs and their fractions.
4.2 The effect of MCTs on DDS
MCTs are beneficial excipients that are being researched in detail for lipid-based pharmaceutical dosage forms application7),8). The results showed that the effects of MCTs and their fractions resulted in an increased rate of delivery of the DDS. This can be clearly observed through a characterization study to assess the effectiveness of the MCTs. The characteristics evaluated in this systematic review were PS, PDI, ZP, EE, DLC, and cell viability. These characteristics exhibited similar ranges for the four types of routes studied in this systematic review.
PS is an important factor to determine the stability, solubility, and drug release properties of MCTs in the delivery system. A typical PS value lies within the range of 10–1000 nm42). From the studies, the PS range of the formulations using MCTs was between 50 and 500 nm; 50–470 nm for the oral/enteral route, 16–21 nm for the topical route, 20–200 nm for the transdermal route, and >90 nm for the parenteral route30),31),33),36),38),40). MCTs incorporation has a significant influence on the assembly and structure of bilayers, producing lipid particles with a larger radius of curvature30). In addition, according to Khan et al.40), the most commonly researched and ideal nanoparticle size for brain administration in animal models is between 50–100 nm. This is because the effectiveness of NP in penetrating the blood brain barrier is size-dependent, with the finest particles exhibiting the greatest effectiveness. Similarly, the incorporation of MCTs for both topical and transdermal applications is associated with enhanced solubility and skin permeation. This effect was attributed to the theory that smaller particles (below than 200 nm) generate greater surface-to-volume ratios, effectively interacting with the skin by disrupting the stratum corneum and accelerating drug release21),35),36),38).
PDI is the particle size distribution of a sample43). A PDI value of 0.1–0.25 implies a narrow size distribution, which is rated as the ideal and suitable particle size distribution44). Meanwhile, a PDI value of 0.3 is considered to be optimum, whereas a PDI value <0.3 is deemed to be suitable in drug delivery applications using LBF43),44). A PDI value of >0.5 may cause stability disruptions due to a higher possibility of particle coalescence44). For the oral/enteral route, two out of nine articles were chosen to study the PDI values, and both studies showed a narrow size distribution of 0.16031),34). In contrast, Liu et al.31) showed that MCTs (RH40) produces a PDI value of <0.2. For topical and parenteral routes, PDI values of 0.13 and 0.27 were detected, respectively, indicating a better drug delivery with MCTs incorporation. Similarly, in the transdermal route, a PDI value of less than 0.3 was observed, which demonstrates the uniformity of droplets and a higher chance of interacting with the skin’s outermost layer (the stratum corneum), and thus can penetrate more effectively, leading to an increase in the drug’s bioavailability and therapeutic potential21),37),38).
Zeta potential (ZP) describes the electrokinetic potential in colloidal systems and has a significant impact on the properties of DDS. It is also considered as an indicator of the NP stability45),46). The ZP depends on several environmental factors, including pH, ionic strength, and the types of ions present47). Generally, a ZP value of ±30 mV is indicated as good stability where it can provide full electrostatic stabilization, which is considered to have sufficient repulsive force to attain better physical colloidal stability. Meanwhile, the ZP value of ±60 mV represents excellent stability and ±20 mV only gives short-term stability to ensure both electrostatic and steric stabilization. Values in the range of ±5 mV signify quick aggregation45),46) and a ZP value of ±10 mV is considered to be neutral48). This systematic review summarizes ZP based on different routes in DDS. For the oral/enteral route, a study by Liu et al.31) showed that MCTs (RH40) produced a ZP value of –25 mV indicating a good colloidal stability. Another study by Luo et al.30) showed that the MCTs exhibited a ZP of –44.4 mV leading to an excellent stability, while those in a study by Wang et al.34) showed a ZP value of 17.37 mV. For the parenteral route, the MCTs in a research by Khan et al.40) showed a ZP of –22±1.5 mV leading to a moderate stability. For the transdermal route, the findings of the study by Gu et al.21) demonstrated consistent ZP values of more than –30 mV, signifying that the formulations achieved substantial stability from aggregation and coalescence resulting in consistency in drug delivery and sustained efficacy over time.
Entrapment or encapsulation efficiency (EE) is defined as the ratio of the initial drug content to the free or unencapsulated drug content in the residue with regard to the overall drug quantity integrated in the formulations49). EE is an important component in determining DLC of particles50). DLC is the amount of drug loaded per unit weight of the particles51). In oral/enteral route, a study conducted by Lu et al.33) resulted in an EE of 81.5±3.5% indicating that curcumin encapsulated in Pickering emulsions containing MCTs exhibit improved stability and drug release. Wang et al.34) concluded that the DMY-loaded self-microemulsion containing caprylic acid improves the poor water solubility and oral bioavailability of DMY as it exhibited an EE of 98.04±0.25% and a DLC of 6.90±0.19%. A study by Zoubari et al.35) using topical route resulted in an EE of >80% for both dexamethasone and diclofenac sodium drugs formulated with Capryol® 90. Similarly, Gu et al.21) reported that as TPL was formulated into an NLC using Capryol 90, TPL-NLC had higher DLC% and EE% (10.35±1.12%, 97.15±9.46%) compared to that in TPL-SLN (9.93±0.98%, 92.81±8.52%). This was due to the disruption of the ordered solid long-chain lipids in Compritol 888 ATO, caused by the incorporation of liquid medium-chain lipids in Capryol 90. This disruption made it easier for the NLCs to load a larger quantity of the drug, which contributed to an increased drug loading and EE in the transdermal distribution. For the parenteral route, an experiment by Li et al.39) produced an EE of >90% for both B-LC-ME-BUF and C-LC-ME-BUF formulations as sustained-release carriers for the antitumor drug BUF. In addition, the MCTs in the study by Khan et al.40) exhibited an EE of 85% and a DLC of 4.26% for CBZ-NLCs containing a high composition of trilaurin. This indicates that CBZ-NLCs are a promising strategy for improving brain delivery and therapeutic outcomes of CBZ in epilepsy. According to Zoubari et al.35), the higher the DLC proportion, the higher the amount of drug released. A DLC of >10% is considered appropriate for formulations44). However, most of the aforementioned articles produced DLC of <10%, as developing methods to increase DLC remains as a challenge52).
Drug solubility refers to the solubility of a drug in water. It is also known as the highest-concentration of a component that can be completely dissolved in a particular solvent at a specific temperature and pressure. The solubility of a drug is determined by the amount of solvent required to dissolve one gram of the drug at a certain temperature53). Drug solubility is directly proportional to oral bioavailability, as it can influence the DDS. The higher the oral bioavailability, the higher the drug solubility53). According to a study by Wang et al.34), the oral bioavailability of DMY in an SMEDDS (C8) was 2.34 times higher than that of pure DMY. This led to the solubility of DMY in C8 being higher than that in the other oil phases. In topical and transdermal delivery systems, the solubility of poorly soluble drugs in the oil phase is crucial because it directly influences drug loading in the formulation. This is particularly important because the capacity of the formulation to retain the drug after solubilization is significantly influenced by the solubility of the drug in the oil phase. For instance, the study by Zoubari et al.35) reported a higher solubility for dexamethasone in Capryol® 90 (9.33±0.22 mg g–1) compared to that in the other lipid carriers. Dexamethasone generally has a low solubility profile; however, incorporation of MCTs increases drug solubility. Diclofenac sodium also had a higher solubility of 42.37±0.25 mg g–1 in Capryol® 90 compared to that in other lipids. This indicates that inclusion of Capryol® 90 resulted in a less organized lipidic structure and a higher drug solubility. Moreover, a study by Qing et al.38) reported the use of Capryol 90 in their formulations. The solubility SCZ in different oils was determined and it was observed to be highest in Capryol 90 (3.30±0.05 mg g–1) as compared to that in other oils. This may be due to the polarity of SCZ, which favors its solubilization in medium-molar-volume oils, such as medium-chain triglycerides or mono- or diglycerides54). In a parenteral DDS, Khan et al.40) proved that a higher MCTs (trilaurin) composition in CBZ-NLCs increased drug solubility. The aqueous solubility of CBZ increased from 113 μg mL–1 to 892 μg mL–1 (7.89-fold) in CBZ-NLCs. This eventually resulted in the selection of CBZ-NLCs as a promising strategy to improve the brain delivery and therapeutic outcomes of CBZ in epilepsy.
Cytotoxicity refers to the toxicity of a substance toward cells. It can be assessed by measuring parameters such as cell viability and IC50. Cell viability (%) is defined as the proportion of healthy cells in a sample, whereas IC50 is defined as the potency of a substance to inhibit a specific biological or biochemical function55). Both indicators measure cellular or metabolic changes associated with viable or non-viable cells. There are 3 articles from the 17 articles that studied the toxicological effects of MCTs. An article by Bunchongprasert et al.22) studying the oral/enteral DDS showed that the presence of triglycerides such as Captex®8000 (C8T) in nanoformulations can reduce the toxicity of Capmul® MCM. The cell viability of SEN2 containing C8T is 147.57±34.42% whereas that of SEN1 containing soybean oil was 104.00±23.56%. This is due to the incorporation of C8T which renders the emulsion system more lipophilic, which may aid in the retention of Capmul® MCM within the lipid droplets via lipid-lipid interaction. At relatively low concentrations, Capmul® MCM monomers may diffuse more readily from less lipophilic droplets without triglycerides to lipophilic cell membranes, disrupting the cell membrane or tight junctions and producing toxicity. In a study by Ghadiri et al.41) of pulmonary DDS, cell viability and IC50 were measured to evaluate the cytotoxicity of each TJM in Calu-3 cells. The IC50 of Na-decanoate was 24 mM, indicating that Na-decanoate was safe over a wide range of concentrations. No cell damage occurred in cells grown in the medium containing Na decanoate. This shows that Na decanoate as MCTs fulfills the requirements of an effective and nontoxic TJM for poorly permeable drug transportation via inhalation. Last but not least, in a study conducted by Gu et al.21) of transdermal delivery, blank vehicles NLC without TPL that consists of Capryol 90 showed no cytotoxicity with the cell survival rates higher than 90%, which indicates that the use of Capryol 90 along with non-ionic surfactants such as Tween 80, Transcutol HP and lecithin are biocompatible and less to toxic to HaCaT cells.
Other than the characterizations collated from the selected studies, there are various other methods with which DDS are commonly analyzed, which include but are not limited to electron and atomic force microscopy, calorimetry, drug release kinetics, and shelf-life determination.
This systematic review summarized the types and effects of the incorporation of MCTs in DDS, and all 17 articles showed similar outcome measures that supported the objectives. In the oral/enteral route, the most common MCTs were identified in three of nine extracted articles, namely Captex and Miglyol 812N22),23),29), while the most common MCTs fractions were identified in four articles, including caprylic (C8:0) and capric (C10) acids29),31),32),34). As for topical and parenteral routes, capric/caprylic (C10/C8) triglycerides are the most commonly MCTs used36),39) whereas Capryol 90 was commonly used as an oil phase for transdermal formulations in selected prior studies21),38). Only one article was found on the pulmonary route, which used sodium (Na) decanoate as an MCTs fraction41).
Generally, MCTs and their fractions have prominent effects on drug transportation because of their distinctive and special characteristics. These unique characteristics affect their absorption and metabolic processes, which increases the efficiency of the DDS8),12),20). In conclusion, outcome measures such as PS of 50-500 nm, PDI value of <0.3, ZP from±25 to ±45 mV, EE of >80% and a higher rate of drug solubility suggests that inclusion of MCTs and their fractions in oral/enteral, topical, transdermal, parenteral, and pulmonary routes increase the drug delivery rate eventually stabilizing the DDS.
4.3 Limitations
This systematic review had some limitations. Research on MCTs usage and its effects on the oral/enteral route is wider than that on other routes, such as topical, parenteral, and pulmonary routes. This led to some difficulties in determining similar outcome measures to assess the effects of MCTs in the stated routes for DDS. For example, only one study has been conducted on the effects of MCTs on the pulmonary route. Thus, future studies should focus more on the pulmonary route to study the effects of MCTs on the route. Future studies should focus on routes other than the stated ones to deepen the understanding of the effects of MCTs on various DDS. Next, because of this review’s article selection based on the inclusion and exclusion criteria, some relevant scientific articles on MCTs and their fractions were excluded, as there were no specified MCTs types and no detailed explanations for MCT-related outcomes. In addition, restricting the search process to studies published in English may have excluded important or fundamental research articles published in other languages.
5 Conclusion
In summary, this systematic review explores the different types and effects of MCTs incorporation in various DDS via oral/enteral, topical, transdermal, parenteral, and pulmonary routes. The selected studies consistently reported that using MCTs improves a variety of critical criteria affecting DDS performance. Notably, the small particle size ranging from 50 to 500 nm, narrow polydispersity index less than 0.3, and favourable zeta potential between±25 to ±45 mV all contributes to formulation stability across several administration routes. In addition, high encapsulation efficiency and sufficient drug loading capacity illustrates the efficacy of MCTs in ensuring reliable and efficient drug delivery. Moreover, MCTs play a key role in enhancing drug solubility, particularly in poorly soluble drugs, impacting their oral bioavailability. This characteristic is importance in designing formulations that address the challenges associated with low solubility. The review also emphasizes the biological compatibility of MCTs and their fractions, showcasing minimal cytotoxicity in various formulations. This aspect is crucial for the safety profile of DDS, especially considering their potential application in topical or transdermal delivery. While the results of this review consistently support the positive effects of MCTs in DDS, the current body of research in the pulmonary route is relatively limited, necessitating further investigation to unravel the full scope of MCTs effects. This review not only merges existing knowledge but also calls for further research initiatives to unlock the full potential of MCTs in developing novel and advanced pharmaceutical formulations and drug delivery systems.
Author Contributions
HP performed the literature search, extraction, analysis, and the initial draft of the manuscript. SII contributed to the manuscript writing. NMH performed additional searches, extractions, and writing. MHZ conceptualized the idea and contributed to the writing.
Acknowledgements
The authors would like to thank the Ministry of Higher Education, Malaysia, for providing funding through the Fundamental Research Grant Scheme (FRGS/1/2020/SKK0/UKM/02/13) for this study.
References
- 1) Liu, D.; Yang, F.; Xiong, F.; Gu, N. The smart drug delivery system and its clinical potential.Theranostics6, 1306-1323 (2016). doi: 10.7150/thno.14858
- 2) Bhowmik, D. Topical Drug Delivery System (2013).
- 3) Jain, K.K. Drug delivery systems - An overview. in Drug Delivery Systems (Jain, K.K. ed.), Humana Press, pp. 1-50 (2008). doi: 10.1007/978-1-59745-210-6_1
- 4) Nikolić, V.; Ilić-Stojanović, S.; Petrović, S.; Tačić, A.; Nikolić, L. Chapter 21 - Administration routes for nano drugs and characterization of nano drug loading. in Characterization and Biology of Nanomaterials for Drug Delivery (Mohapatra, S.S.; Ranjan, S.; Dasgupta, N.; Mishra, R.K.; Thomas, S. eds.), Elsevier, pp. 587-625 (2019). doi: 10.1016/B978-0-12-814031-4.00021-0
- 5) Benson, H.A.E.; Grice, J.E.; Mohammed, Y.; Namjoshi, S.; Roberts, M.S. Topical and transdermal drug delivery: From simple potions to smart technologies.Curr. Drug Deliv.16, 444-460 (2019).
- 6) Brunaugh, A.D.; Smyth, H.D.C.; Williams III, R.O. Essential Pharmaceutics [Internet]. 2019. 1-193 p. Available from: http://link.springer.com/10.1007/978-3-030-31745-4
- 7) Efendy Goon, D.; Sheikh Abdul Kadir, S.H.; Latip, N.A.; Ab Rahim, S.; Mazlan, M. Palm oil in lipid-based formulations and drug delivery systems.Biomolecules9, 64 (2019). doi: 10.3390/biom9020064
- 8) Prajapati, H.N.; Dalrymple, D.M.; Serajuddin, A.T. A comparative evaluation of mono-, di- and triglyceride of medium-chain fatty acids by lipid/surfactant/water phase diagram, solubility determination and dispersion testing for application in pharmaceutical dosage form development.Pharm. Res.29, 285-305 (2012). doi: 10.1007/s11095-011-0541-3
- 9) Chen, F.M.; Wang, J.Y.; Sun, L.C.; Juang, R.F.; Huang, T.J. et al. Efficacy of medium-chain triglycerides compared with long-chain triglycerides in total parenteral nutrition in patients with digestive tract cancer undergoing surgery.Kaohsiung J. Med. Sci.21, 487-494 (2005). doi: 10.1016/s1607-551x (09) 70156-1
- 10) Izgelov, D.; Shmoeli, E.; Domb, A.J.; Hoffman, A. The effect of medium-chain and long chain triglycerides incorporated in self-nano emulsifying drug delivery systems on oral absorption of cannabinoids in rats.Int. J. Pharm.580, 119201 (2020). doi: 10.1016/j.ijpharm.2020.119201
- 11) Nimbkar, S.; Leena, M.M.; Moses, J.A.; Anandharamakrishnan, C. Medium-chain triglycerides (MCTs) : State-of-the-art on chemistry, synthesis, health benefits and applications in food industry.Compr. Rev. Food Sci. Food Saf.21, 843-867 (2022). doi: 10.1111/1541-4337. 12926
- 12) Shah, N.D.; Limketkai, B.N. The use of medium-chain triglycerides in gastrointestinal disorders.Pract. Gastroenterol.41 (2), 20-28 (2017).
- 13) Myrie, S.B.; Jones, P.J.H. 10 - Functional foods and obesity. in Functional Foods (Second ed.) (Saarela, M. ed.), Woodhead Publishing, pp. 234-260 (2011). doi: 10.1533/9780857092557.2.234
- 14) Huang, C.B.; Alimova, Y.; Myers, T.M.; Ebersole, J.L. Short- and medium-chain fatty acids exhibit antimicrobial activity for oral microorganisms.Arch. Oral Biol.56, 650-654 (2011). doi: 10.1016/j.archoralbio. 2011.01.011
- 15) Roopashree, P.G.; Shetty, S.S.; Suchetha Kumari, N. Effect of medium-chain fatty acid in human health and disease.J. Funct. Foods87, 104724 (2021). doi: 10. 1016/j.jff.2021.104724
- 16) Jadhav, H.B.; Annapure, U.S. Triglycerides of medium-chain fatty acids: A concise review.J. Food Sci. Technol.60, 2143-2152 (2023). doi: 10.1007/s13197-022-05499-w
- 17) Bach, A.C.; Babayan, V.K. Medium-chain triglycerides: An update.Am. J. Clin. Nutr.36, 950-962 (1982). doi: 10.1093/ajcn/36.5.950
- 18) Interim Revision Announcements (IRAs). Medium-Chain Triglycerides. United States Pharmacopeial Conv [Internet]. 2019;3-6. Available from: https://www.uspnf.com/sites/default/files/usp_pdf/EN/USPNF/revisions/medium-chain-triglycerides-ira.pdf
- 19) Marten, B.; Pfeuffer, M.; Schrezenmeir, J. Medium-chain triglycerides.Int. Dairy J.16, 1374-1382 (2006). doi: 10.1016/j.idairyj.2006.06.015
- 20) Dayrit, F.M. Lauric acid is a medium-chain fatty acid, coconut oil is a medium-chain triglyceride.Philipp. J. Sci.143, 157-166 (2014).
- 21) Gu, Y.; Yang, M.; Tang, X.; Wang, T.; Yang, D. et al. Lipid nanoparticles loading triptolide for transdermal delivery : Mechanisms of penetration enhancement and transport properties.J. Nanobiotechnology16, 68 (2018). doi: 10.1186/s12951-018-0389-3
- 22) Bunchongprasert, K.; Shao, J. Cytotoxicity and permeability enhancement of Capmul® MCM in nanoemulsion formulation.Int. J. Pharm.561, 289-295 (2019). doi: 10.1016/j.ijpharm.2019.03.010
- 23) Grüne, L.; Bunjes, H. Suitability of phosphatidylcholine-based formulations for liquid filling in hard capsules.Eur. J. Pharm. Sci.153, 105470 (2020). doi: 10.1016/j.ejps.2020.105470
- 24) Shah, A.; Serajuddin, A. Development of solid self-emulsifying drug delivery system (SEDDS) I: Use of Poloxamer 188 as both solidifying and emulsifying agent for lipids.Pharm. Res.29, 2817-2832 (2012). doi: 10.1007/s11095-012-0704-x
- 25) Hairul, N.M.; Ibrahim, S.I.; Nor Khaizan, A.; Salim, N.; Zulfakar, M.H. Celecoxib-loaded nanoemulsion: Solubility of Celecoxib in various fractionated medium chain trigylcerides and surfactants. in The Virtual 3rd International Research Network Initiative (IRNI) Symposium 2022 (Ramasamy, K.; Singh, G.K.S.; Karuppannan, M.; Sheshala, R.; Abdul Hamid, K. eds.), Malaysian Journal of Medicine and Health Sciences (MJMHS) 30-1 (2023).
- 26) Patil, M.U.; Rajput, A.P.; Belgamwar, V.S.; Chalikwar, S.S. Development and characterization of amphotericin B nanoemulsion-loaded mucoadhesive gel for treatment of vulvovaginal candidiasis.Heliyon8, e11489 (2022). doi: 10.1016/j.heliyon.2022.e11489
- 27) Kei-Xian, T.; Ling-Ling Evelyn, N.; Say Chye Joachim, L. Formulation development of a food-graded curcumin-loaded medium-chain triglycerides-encapsulated kappa carrageenan (CUR-MCTs-KC) gel bead based oral delivery formulation.Materials14, 2783 (2021). doi: 10.3390/ma14112783
- 28) Garcia, J.; Fernández-Blanco, Á.; Teixidó, M.; Sánchez-Navarro, M.; Giralt, E. d-Polyarginine lipopeptides as intestinal permeation enhancers.ChemMedChem.13, 2045-2052 (2018). doi: 10.1002/cmdc.201800428
- 29) Liu, Q.; Chen, J.; Qin, Y.; Jiang, B.; Zhang, T. Encapsulation of pterostilbene in nanoemulsions: Influence of lipid composition on physical stability, in vitro digestion, bioaccessibility, and Caco-2 cell monolayer permeability.Food Funct.10, 6604-6614 (2019). doi: 10.1039/c9fo01260e
- 30) Luo, L.; Chen, Q.; Wei, N.; Liu, Y.; He, H. et al. The modulation of drug-loading stability within lipid membranes via medium-chain triglycerides incorporation.Int. J. Pharm.566, 371-382 (2019). doi: 10.1016/j.ijpharm.2019.06.003
- 31) Liu, J.; Werner, U.; Funke, M.; Besenius, M.; Saaby, L. et al. SEDDS for intestinal absorption of insulin: Application of Caco-2 and Caco-2/HT29 co-culture monolayers and intra-jejunal instillation in rats.Int. J. Pharm.560, 377-384 (2019). doi: 10.1016/j.ijpharm. 2019.02.014
- 32) Hossain, S.; Joyce, P.; Parrow, A.; Jõemetsa, S.; Höök, F. et al. Influence of bile composition on membrane incorporation of transient permeability eEnhancers.Mol. Pharmaceutics17, 4226-4240 (2020). doi: 10.1021/acs.molpharmaceut.0c00668
- 33) Lu, X.; Huang, Q. Stability and in vitro digestion study of curcumin-encapsulated in different milled cellulose particle stabilized Pickering emulsions.Food Funct.11, 606-616 (2020). doi: 10.1039/c9fo02029b
- 34) Wang, Y.; Chen, L.; Adu-Frimpong, M.; Wei, C.; Weng, W. et al. Preparation, in vivo and in vitro evaluation, and pharmacodynamic study of DMY-loaded self-microemulsifying drug delivery system.Eur. J. Lipid Sci. Technol.123, 2000369 (2021). doi: 10.1002/ejlt. 202000369
- 35) Zoubari, G.; Staufenbiel, S.; Volz, P.; Alexiev, U.; Bodmeier, R. Effect of drug solubility and lipid carrier on drug release from lipid nanoparticles for dermal delivery.Eur. J. Pharm. Biopharm, 110, 39-46 (2017). doi: 10.1016/j.ejpb.2016.10.021
- 36) de Souza, I.D.L.; Saez, V.; de Campos, V.E.B.; Mansur, C.R.E. Size and vitamin E release of nanostructured lipid carriers with different liquid lipids, surfactants and preparation methods.Macromol. Symp.383, 1800011 (2019). doi: 10.1002/masy.201800011
- 37) He, E.; Li, H.; Li, X.; Wu, X.; Lei, K.; Diao, Y. Transdermal delivery of indirubin-loaded microemulsion gel : Preparation, characterization and anti-psoriatic activity.Int. J. Mol. Sci.23, 3798 (2022).
- 38) Yang, Q.; Liu, S.; Gu, Y.; Tang, X.; Wang, T. et al. Development of sulconazole-loaded nanoemulsions for enhancement of transdermal permeation and antifungal activity.Int. J. Nanomedicine14, 3955-3966 (2019). doi: 10.2147/IJN.S206657
- 39) Li, Y.; Angelova, A.; Liu, J.; Garamus, V.M.; Li, N. et al. In situ phase transition of microemulsions for parenteral injection yielding lyotropic liquid crystalline carriers of the antitumor drug bufalin.Colloids Surf. B Biointerfaces173, 217-225 (2019). doi: 10.1016/j.colsurfb.2018.09.023
- 40) Khan, N.; Shah, F.A.; Rana, I.; Ansari, M.M.; Din, F.U. et al. Nanostructured lipid carriers-mediated brain delivery of carbamazepine for improved in vivo anticonvulsant and anxiolytic activity.Int. J. Pharm.577, 119033 (2020). doi: 10.1016/j.ijpharm.2020.119033
- 41) Ghadiri, M.; Young, P.M.; Jarolimek, W.; Grau, G.E.R.; Oliver, B.G.G. et al. The effect of non-specific tight junction modulators on the transepithelial transport of poorly permeable drugs across airway epithelial cells.J. Drug Target.25, 342-349 (2017). doi: 10.1080/ 1061186X.2016.1258703
- 42) Kalepu, S.; Manthina, M.; Padavala, V. Oral lipid-based drug delivery systems - An overview.Acta Pharm. Sin. B3, 361-372 (2013). doi: 10.1016/j.apsb.2013. 10.001
- 43) Danaei, M.; Dehghankhold, M.; Ataei, S.; Hasanzadeh Davarani, F.; Javanmard, R. et al. Impact of particle size and polydispersity index on the clinical applications of lipidic nanocarrier systems.Pharmaceutics10, 57 (2018). doi: 10.3390/pharmaceutics10020057
- 44) Del Aram Jafari, T. Effectiveness of topical caraway essential oil loaded into nanostructured lipid carrier as a promising platform for the treatment of infected wounds.Colloids Surf.610, 125748 (2021). doi: 10. 1016/j.colsurfa.2020.125748
- 45) Honary, S.; Zahir, F. Effect of Zeta potential on the properties of nano-drug delivery systems - A review (Part 1).Trop. J. Pharm. Res.12, 255-264 (2013). doi: 10.4314/tjpr.v12i2.19
- 46) Honary, S.; Zahir, F. Effect of Zeta potential on the properties of nano-drug delivery systems - A review (Part 2).Trop. J. Pharm. Res.12, 265-273 (2013). doi: 10.4314/tjpr.v12i2.20
- 47) Khosa, A.; Reddi, S.; Saha, R.N. Nanostructured lipid carriers for site-specific drug delivery.Biomed. Pharmacother.103, 598-613 (2018). doi: 10.1016/j.biopha. 2018.04.055
- 48) Chauhan, I.; Yasir, M.; Verma, M.; Singh, A.P. Nanostructured lipid carriers: A groundbreaking approach for transdermal drug delivery.Adv. Pharm. Bull.10, 150-165 (2020). doi: 10.34172/apb.2020.021
- 49) Gaikwad, V.L.; Choudhari, P.B.; Bhatia, N.M.; Bhatia, M.S. Chapter 2 - Characterization of pharmaceutical nanocarriers: In vitro and in vivo studies. in Nanomaterials for Drug Delivery and Therapy (Grumezescu, A.M. ed.), William Andrew Publishing, pp. 33-58 (2019). doi: 10.1016/B978-0-12-816505-8.00016-3
- 50) Dey, S.; Pramanik, S.; Malgope, A. Formulation and optimization of sustained release stavudine microspheres using response surface methodology.ISRN Pharm.2011, 627623 (2011). doi: 10.5402/2011/ 627623
- 51) Waghule, T.; Rapalli, V.K.; Gorantla, S.; Saha, R.N.; Dubey, S.K. et al. Nanostructured lipid carriers as potential drug delivery systems for skin disorders.Curr. Pharm. Des.26, 4569-4579 (2020). doi: 10.2174/1381612826666200614175236
- 52) Liu, Y.; Yang, G.; Jin, S.; Xu, L.; Zhao, C.X. Development of high-drug-loading nanoparticles.Chempluschem.85, 2143-2157 (2020). doi: 10.1002/cplu.202000 496
- 53) Savjani, K.T.; Gajjar, A.K.; Savjani, J.K. Drug solubility: importance and enhancement techniques.ISRN Pharm.2012, 195727 (2012). doi: 10.5402/2012/ 195727
- 54) Azeem, A.; Rizwan, M.; Ahmad, F.J.; Iqbal, Z.; Khar, R.K.; Aqil, M. et al. Nanoemulsion components screening and selection: A technical note.AAPS PharmSciTech.10, 69-76 (2009).
- 55) Adan, A.; Kiraz, Y.; Baran, Y. Cell proliferation and cytotoxicity assays.Curr. Pharm. Biotechnol.17, 1213-1221 (2016). doi: 10.2174/13892010176661608081605

;%0A%09%09%09newWindow.document.open();%0A%09%09%09newWindow.document.write('<img src=%22./Graphics/73_ess23204_t1_1.jpg%22>');%0A%09%09%09newWindow.document.close();%0A%09%09)
;%0A%09%09%09newWindow.document.open();%0A%09%09%09newWindow.document.write('<img src=%22./Graphics/73_ess23204_t1_2.jpg%22>');%0A%09%09%09newWindow.document.close();%0A%09%09)
;%0A%09%09%09newWindow.document.open();%0A%09%09%09newWindow.document.write('<img src=%22./Graphics/73_ess23204_t2.jpg%22>');%0A%09%09%09newWindow.document.close();%0A%09%09)
;%0A%09%09%09newWindow.document.open();%0A%09%09%09newWindow.document.write('<img src=%22./Graphics/73_ess23204_t3.jpg%22>');%0A%09%09%09newWindow.document.close();%0A%09%09)
;%0A%09%09%09newWindow.document.open();%0A%09%09%09newWindow.document.write('<img src=%22./Graphics/73_ess23204_t4.jpg%22>');%0A%09%09%09newWindow.document.close();%0A%09%09)
;%0A%09%09%09newWindow.document.open();%0A%09%09%09newWindow.document.write('<img src=%22./Graphics/73_ess23204_t5.jpg%22>');%0A%09%09%09newWindow.document.close();%0A%09%09)
;%0A%09%09%09newWindow.document.open();%0A%09%09%09newWindow.document.write('<img src=%22./Graphics/73_ess23204_t6.jpg%22>');%0A%09%09%09newWindow.document.close();%0A%09%09)
;%0A%09%09%09newWindow.document.open();%0A%09%09%09newWindow.document.write('<img src=%22./Graphics/73_ess23204_t7.jpg%22>');%0A%09%09%09newWindow.document.close();%0A%09%09)
;%0A%09%09%09newWindow.document.open();%0A%09%09%09newWindow.document.write('<img src=%22./Graphics/73_ess23204_t8.jpg%22>');%0A%09%09%09newWindow.document.close();%0A%09%09)
;%0A%09%09%09newWindow.document.open();%0A%09%09%09newWindow.document.write('<img src=%22./Graphics/73_ess23204_t9.jpg%22>');%0A%09%09%09newWindow.document.close();%0A%09%09)