Abstract
Purpose: To investigate the root and canal morphology of mandibular second molars, including anatomical variations, in a Black South African population using two classification systems.
Methods: Cone-beam computed tomography images of 386 teeth were evaluated. The number of roots and canal configurations were categorized using the classifications of Vertucci (with modifications by Sert and Bayirli) and Ahmed et al. (including the modified Melton classification). Relationships between variables were assessed using Fisher’s exact test (P < 0.05).
Results: Mandibular second molars were predominantly two-rooted (91.7%). The majority of teeth had three canals including Type IV mesial (41.2%) and Type I (75.1%) distal (Ahmed et al. configuration: 2MDM M2 D1). Three or more canals were present in almost one-fifth of mesial (n = 72/386, 18.6%) and a small number of distal (n = 21/386, 5.4%) roots. Males displayed additional canals more frequently in the distal root (P = 0.02). C-shaped anatomy was found in 5.7%. Among the C-shapes, the most common was Melton’s Type III in the coronal (50%), middle (81%) and apical (72%) thirds.
Conclusion: In this population, mandibular second molar teeth exhibited diverse morphology, which would have clinical significance for endodontic practitioners. The Ahmed et al. classification provided a better description than the Vertucci classification.
Introduction
Knowledge of both common and aberrant root and canal anatomy is vital for both nonsurgical and surgical endodontics [1]. Mandibular second molars frequently require endodontic treatment, and commonly display two roots with three canals [2], but several studies have reported deviations from this norm [3,4,5]. These deviations may include conical roots [5], C-shaped morphology [5], or the presence of additional canals in both the mesial and distal root systems. For this tooth type, C-shaped canals, as well a Vertucci Type IV configuration in the mesial root of two-rooted mandibular second molars, reportedly have a higher prevalence in Asian populations [6]. These anatomical variations may have clinical significance in the context of endodontic treatment. Anatomical differences in dental morphology are known to be influenced by race, age, sex, ethnicity, and even geographical area [7].
Historically, clearing and staining have been widely used to evaluate canal morphology [8]. More recently, cone-beam computed tomography (CBCT) has been successfully applied in studies of dental morphology in the context of endodontics [9]. The non-destructive nature of CBCT facilitates precise three-dimensional (3D) imaging at an acceptable radiation dose, allowing retrospective analysis of dental anatomy in large numbers of samples [10].
The well-known Vertucci classification [1] has been widely used for reporting root canal morphology [10]. However, this system has limitations and is unable to classify all configurations, especially in complex teeth [11]. To aid the description of complex canal configurations, additions to the original classification were proposed [12]. In 2017, the classification system of Ahmed et al. was introduced with the aim of reporting both root number and canal configuration (simple or complex) of any tooth type simultaneously, using a single code denoting the root and canal structure [13]. So far, only a limited number of studies have used this newer classification system to describe root and canal morphology, including dental anomalies, in comparison with more established classifications [14].
The population of South Africa consists mainly of Black Africans [Statistics South Africa, 2011]. Few studies have documented the dental anatomy of this specific population group [11,15], or that of mixed South African population groups [7].
A review of the existing literature found no information on the overall root and canal morphology (including dental anomalies, such as C-shaped anatomy) of mandibular second molars exclusively within a Black South African population. Consequently, no data are available concerning the prevailing root and canal morphology of this population group and region. The aim of the present study was to describe the root and canal morphology, including C-shaped anatomy, of mandibular second molars in this previously unreported population group and region based on CBCT images and two classification systems.
Materials and Methods
Subjects
This descriptive, cross-sectional observational study was approved by the Research Ethics Committee of the Faculty of Health Sciences, University of Pretoria (Protocol number: 331/2021). CBCT images of mandibular second molars were evaluated from patients attending the diagnostic imaging unit at the University of Pretoria Oral Health Center between November 2014 and September 2021. Scans in the existing database were studied retrospectively. No additional subjects were exposed to radiation for this study. The as low as reasonably achievable (ALARA) concept had been used at the time of scan acquisition by experienced radiographers. Scans meeting the following inclusion criteria were assessed:
-
1.
Black South African patients aged 15 years or older, seeking dental treatment at an academic hospital.
-
2.
Mature mandibular second molars demonstrating fully developed apices (i.e., closed roots).
-
3.
No previous treatment that had modified the original root and canal anatomy (i.e., teeth with posts, crowns, previous endodontic treatment and endodontic surgery were excluded).
-
4.
Scans of a quality acceptable for visualization of root and canal anatomy.
-
5.
Voxel size equal to or smaller than 0.2 mm.
Convenience sampling was employed, and sample size calculations were determined using statistical software (Epi-Info version 7, Atlanta, GA, USA). Assuming a prevalence of 50% with a 5% margin of error and a 95% confidence interval, the minimum required sample size was determined to be n = 384, including both male and female subjects with scans from both sides.
Evaluation of CBCT scans
The methodology employed has been reported previously [15]. The CBCT images included had been acquired using a Planmeca Promax 3D Max CBCT machine (Planmeca OY, Helsingfors, Finland) for a number of reasons, including maxillofacial and oral surgery (for diagnosis and treatment of maxillofacial trauma and pathology), as well as diagnosis and treatment planning in a number of different specialist dental fields. The CBCT machine parameters were adjustable and were varied as needed for each clinical indication. The scanning parameters were variable depending on the scan required, as follows: tube current 1-14 mA, tube voltage 54-90 kV, focal spot diameter 0.6 mm. The resulting voxel size therefore varied from 0.15 to 0.60 mm.
Digital imaging software (Romexis version 6.0, Planmeca, Planmeca OY, Helsingfors, Finland) was used for analysis of the scans. Software settings (e.g., sharpness, brightness and contrast) were optimized by each observer before serial coronal, axial and sagittal sections were viewed. The number of roots and canal morphology were determined. Two observers (previously calibrated through assessment of 50 teeth unrelated to the study) evaluated the samples. In keeping with previously described methodology [16], the first observer (experienced in endodontics) evaluated all of the images and the second observer (both an anatomist and dentist experienced in oral radiology) evaluated one tenth of the sample. Disagreements not resolved by consensus were referred to a third observer for a final opinion regarding the classification. Data were entered into Microsoft Excel 2016 (Microsoft Corp., Redmond, WA, USA).
Classification
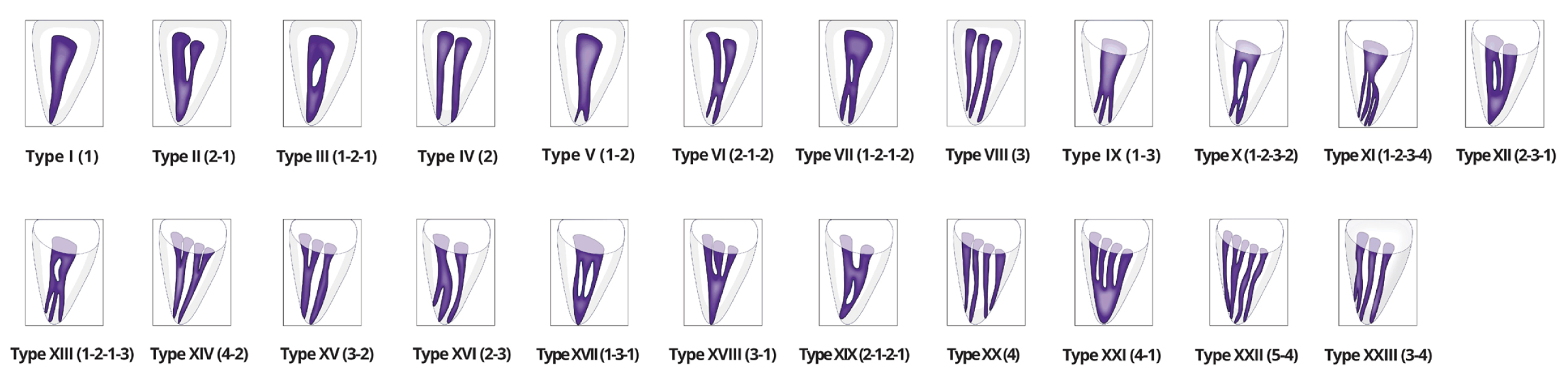
The root and canal morphology of the mandibular second molars was classified using the original Vertucci classification [1], including the later additions proposed by Sert et al. [12]. Canal configurations were reported per root (Fig. 1). Classification was additionally performed using the Ahmed et al. system [17], in conjunction with the modified Melton classification for description of C-shaped anatomy where present [18]. A limited description of the Ahmed et al. system, relevant to the present study, is provided in Fig. 2. The code MDM was allocated as a descriptor for mandibular second molars when the Ahmed et al. system was used. As C-shaped canals cannot be described using the Vertucci classification [1], these were reported as unclassified in the present study. Conical roots with non-C-shaped anatomy were, however, described using the Vertucci classification. The Ahmed et al. system does make provision for C-shaped anatomy [17], and this is reported by Fan et al. as part of a single descriptive code based on the modified Melton classification [18]. C-shaped anatomy according to this classification, as used in the present study, was described as follows using the prefix “CSC” for “C-shaped canal”, followed by an Arabic numeral indicating the type of C-shape. CSC1: a continuous C-shaped canal with no separation; CSC2: a semi-colon shaped canal, with dentin separating the canals from each other; CSC3: two or three separate canals: CSC4: a single canal, either oval or round in shape; CSC5: no observable canal.
To ensure subject anonymity, all scans were de-identified prior to statistical analysis by assigning numbers to the dataset instead of the subjects’ hospital file information. Both the age and sex of the subjects were recorded to evaluate differences in root number and/or canal morphology. In keeping with previous methodology [10], three age cohorts were selected in order to evaluate clinically relevant differences in canal morphology: <25 years; 25-40 years; and >40 years. Differences in the prevalence of canal morphology in relation to sex and age were reported using Fisher’s Exact test, with corrections for multiple testing where required. Statistical analysis was performed using R Statistical Software version 4.1.1 (R Core Team 2021. R. A language and environment for statistical computing. R Foundation for statistical computing, Vienna, Austria). The level of significance was set at P < 0.05. Simple percentage agreement was used to represent inter- and intra-rater reliability.
Results
Sample description and examiner agreement
In total, 386 mandibular second molar teeth were evaluated from 239 subjects. The subject age range was 15-79 years (mean: 35.4 years). The distribution of left- (n = 195/386, 50.5%) and right-sided (n = 191/386, 49.5%) samples was approximately even. The sex distribution included slightly fewer teeth from female subjects (n = 192/386, 49.7%) than from males (n = 194/386, 50.3%). No samples were excluded. The inter- (87.1%) and intra-observer (84.6%) scores indicated a high degree of examiner agreement.
Root number and C-shaped anatomy
The mandibular second molars evaluated in the present study were predominantly two-rooted (n = 354/386, 91.7%). A smaller number of teeth were single-rooted (n = 24/386, 6.2%), three-rooted (n = 6/386, 1.6%) or four-rooted (n = 2/386, 0.5%).
One tooth demonstrated true fusion of the mesial and distal roots and was not considered C-shaped. C-shaped roots and canals were found in only a small number of teeth (n = 22/386, 5.7%). The most common C-shaped canal morphology in the coronal third was type 3 (n = 11/22, 50.0%), followed by type 1 (n = 6/22, 27.3%), type 2 (n = 2/22, 9.1%) and type 4 (n = 3/22, 13.6%). No type 5 C-shapes were found. The type of C-shape in a given tooth was not necessarily consistent along the root’s length, and the morphology varied between the coronal, middle and apical root thirds. These variations are presented in Table 1. Information regarding the number of canals present in C-shaped teeth was reported under the Ahmed et al. classification’s findings of the present study (Table 4).
Table 1
Distribution of C-shaped canal anatomy of mandibular second molars per root third
| Type of C-shape |
C1 (%) |
C2 (%) |
C3 (%) |
C4 (%) |
Total n (%) |
| Coronal |
6 (27.3) |
2 (9.1) |
11 (50.0) |
3 (13.6) |
22 (100) |
| Middle |
- |
1 (4.6) |
18 (81.8) |
3 (13.6) |
22 (100) |
| Apical |
1 (4.6) |
- |
16 (72.7) |
5 (22.7) |
22 (100) |
Vertucci canal configurations
For molar teeth, the Vertucci classification is normally applied to roots [1]. Table 2 summarizes the canal configurations of mandibular second molars according to Vertucci.
Twenty-four of the present mandibular second molars were single-rooted. One single-rooted mandibular second molar was classified as Vertucci Type I (n = 1/24, 4.2%) and another as Type II (n = 1/24, 4.2%). The remaining single-rooted teeth were found to be C-shaped (n = 22/24, 91.6%) and were considered unclassifiable by the Vertucci system.
Among two-rooted mandibular second molars, the majority of mesial roots displayed Type IV configurations (n = 146/354, 41.2%), followed by Type III (n = 64/354, 18.1%), Type II (n = 43/354, 12.1%) and Type X (n = 22/354, 6.2%). Several other mesial root configurations were also represented in small numbers. The majority of the distal roots of two-rooted teeth displayed a Type I configuration (n = 265/354, 74.9%), followed by a Type III configuration (n = 43/354, 12.1%).
Among three-rooted mandibular second molars (n = 6/386), five teeth had a mesial root that split into separate mesiobuccal and mesiolingual roots approximately half way down the root surface. The mesial roots of four of these five teeth were classified as Vertucci Type IV, and one as Type XV. The remaining three-rooted sample (n = 1/386, 0.25%) was observed as a radix entomolaris (with separate mesial, distal and distolingual roots), and displayed a Type XII configuration in the mesial root, Type I in the distal root, and Type I in the separate distolingual root.
Two four-rooted mandibular second molars were observed. Both of these teeth showed a split of the mesial and distal roots about halfway down the root surface (branching into separate mesiobuccal, mesiolingual, distobuccal and distolingual roots). Whilst each root displayed individual canals in the apical half, the mesial roots were classified as Type IV and the distal roots as Type V by the Vertucci classification due to the overall canal morphology.
More than two canals were found in almost one-fifth of mesial roots (n = 72/386, 18.6%) and a smaller number of distal (n = 21/386, 5.4%) roots.
Table 2
Canal configurations per root of mandibular second molars according to the Vertucci classification
| Root number |
Canal location
|
I
1
(%) |
II
2-1
(%) |
III
1-2-1
(%) |
IV
2
(%) |
V
1-2
(%) |
VI
2-1-2
(%) |
VII
1-2-1-2
(%) |
VIII
3
(%) |
IX
1-3
(%) |
X
1-2-3-2
(%) |
XII
2-3-1
(%) |
XIV
4-2
(%) |
XV
3-2
(%) |
XVI
2-3
(%) |
XVII
1-3-1
(%) |
XVIII
3-1
(%) |
XIX
2-1-2-1
(%) |
XXI
4-1
(%) |
Unclassi-fied
|
Total n of teeth
|
| One |
|
1
(4.2) |
1
(4.2) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
22
(91.6) |
24 |
| Two |
M |
8
(2.3) |
43
(12.1) |
64
(18.1) |
146
(41.2) |
17
(4.8) |
1
(0.3) |
3
(0.8) |
1
(0.3) |
|
22
(6.2) |
10
(2.8) |
3
(0.8) |
8
(2.3) |
1
(0.3) |
17
(4.8) |
1
(0.3) |
1
(0.3) |
1
(0.3) |
7
(2.0) |
354 |
| D |
265
(74.9) |
6
(1.6) |
43
(12.1) |
1
(0.3) |
17
(4.9) |
1
(0.3) |
|
|
3
(0.8) |
3
(0.8) |
|
|
|
|
11
(3.1) |
|
|
2
(0.6) |
2
(0.6) |
|
| Three |
MB/ML |
|
|
|
4
(66.6) |
|
|
|
|
|
|
|
|
1
(16.7) |
|
|
|
|
|
|
6 |
| M |
|
|
|
|
|
|
|
|
|
|
1
(16.7) |
|
|
|
|
|
|
|
|
|
| D |
5
(83.3) |
|
|
|
1
(16.7) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| DL |
1
(100) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Four |
MB/ML |
|
|
|
2
(100) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
| DB/DL |
|
|
|
|
2
(100) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Total |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
386 |
Canal configurations according to the Ahmed et al. classification
Tables 3 and 4 provide a description of mandibular second molar teeth according to the Ahmed et al. classification. Using this classification, mandibular second molars were divided into two groups: conventional teeth (i.e., non-C-shaped anatomy, n = 364/386, 94.3%) and those with C-shaped anatomy (n = 22/386, 5.7%).
In the conventional group, two single-rooted teeth were found. These teeth were coded as 1MDM1 (n = 1/364, 0.3%) and 1MDM2-1 (n = 1/364, 0.3%) respectively.
The most common configuration observed in conventional two-rooted mandibular second molars was 2MDM M2 D1 (n = 96/364, 26.3%), followed by 2MDM M1-2-1 D1 (n = 55/364, 15.1%) and 2MDM M2-1 D1 (n = 33/364, 9.1%). The remaining two-rooted mandibular second molars displayed a large number of unique codes, each with a small number of representatives (Table 3).
Among three-rooted mandibular second molars, the most common configuration was 3MDM MB1 ML1 D1 (n = 4/364, 1.2%). The remaining three-rooted tooth was coded as 3MDM MB1 ML2-1 D1-2 (n = 1/364, 0.3%).
Two four-rooted mandibular second molars were observed, and both were considered to be 4MDM MB1 ML1 DB//DL1-2 (n = 2/364, 0.5%).
The mandibular second molars demonstrating C-shaped anatomy according to the Ahmed et al. classification were exclusively single-rooted (Table 4). The most common configurations observed were (CSC3)1MDM3 (n = 4/22, 18.3%) and (CSC3)1MDM3-2 (n = 4/22, 18.3%), both of which demonstrated type 3 C-shapes in the coronal third. This was followed by (CSC1)1MDM1-2 (n = 3/22, 13.7%) and (CSC4)1MDM1 (n = 2/22, 9.2%). The remainder of the C-shaped teeth demonstrated unique codes when classified using the Ahmed et al. system.
Table 3
Root canal configurations of mandibular second molar teeth without C-shaped anatomy according to the Ahmed et al. classification
| Configuration |
Number (n =) |
Total percentage (%) |
Cumulative total |
| (RE)3MDM MB2-3-1 D1 L1 |
1 |
0.3 |
1 |
| 1MDM1 |
1 |
0.3 |
2 |
| 1MDM2-1 |
1 |
0.3 |
3 |
| 2MDM 1M2 D1 |
6 |
1.6 |
9 |
| 2MDM 1M2 D2 |
1 |
0.3 |
10 |
| 2MDM BRM2 BRD1-2 |
1 |
0.3 |
11 |
| 2MDM BRM2 D1 |
4 |
1.0 |
15 |
| 2MDM BRM2 D1-2 |
1 |
0.3 |
16 |
| 2MDM BRM2 D1-2-1 |
1 |
0.3 |
17 |
| 2MDM BRM2 D1-3 |
1 |
0.3 |
18 |
| 2MDM M1 D1 |
8 |
2.1 |
26 |
| 2MDM M1-2 BRD1-2 |
1 |
0.3 |
27 |
| 2MDM M1-2 D1 |
14 |
3.8 |
41 |
| 2MDM M1-2 D1-2-1 |
2 |
0.5 |
43 |
| 2MDM M1-2-1 D1 |
55 |
15.1 |
98 |
| 2MDM M1-2-1 D1-2 |
2 |
0.5 |
100 |
| 2MDM M1-2-1 D1-2-1 |
6 |
1.6 |
106 |
| 2MDM M1-2-1 D2-1 |
1 |
0.3 |
107 |
| 2MDM M1-2-1-2 D1 |
2 |
0.5 |
109 |
| 2MDM M1-2-1-2 D1-2 |
1 |
0.3 |
110 |
| 2MDM M1-2-3-2 D1 |
13 |
3.5 |
123 |
| 2MDM M1-2-3-2 D1-2 |
1 |
0.3 |
124 |
| 2MDM M1-2-3-2 D1-2-1 |
3 |
0.8 |
127 |
| 2MDM M1-2-3-2 D1-3 |
1 |
0.3 |
128 |
| 2MDM M1-2-3-2 D1-3-1 |
3 |
0.8 |
131 |
| 2MDM M1-2-3-2/D1-2 |
1 |
0.3 |
132 |
| 2MDM M1-3-1 D1 |
13 |
3.5 |
145 |
| 2MDM M1-3-1 D1-2-1 |
2 |
0.5 |
147 |
| 2MDM M1-3-1 D1-3-1 |
1 |
0.3 |
148 |
| 2MDM M1-3-1/D1 |
1 |
0.3 |
149 |
| 2MDM M1-3-2-1 D1 |
1 |
0.3 |
150 |
| 2MDM M1-3-2-1 D1-3-1 |
1 |
0.3 |
151 |
| 2MDM M2 BRD1 |
1 |
0.3 |
152 |
| 2MDM M2 D1-3-6-2 |
1 |
0.3 |
153 |
| 2MDM M2 D1 |
96 |
26.3 |
249 |
| 2MDM M2 D1-2 |
8 |
2.2 |
257 |
| 2MDM M2 D1-2-1 |
15 |
4.1 |
272 |
| 2MDM M2 D1-2-3-2 |
3 |
0.8 |
275 |
| 2MDM M2 D1-3 |
1 |
0.3 |
276 |
| 2MDM M2 D1-3-1 |
7 |
1.9 |
283 |
| 2MDM M2 D2 |
2 |
0.5 |
285 |
| 2MDM M2-1 D1 |
33 |
9.1 |
318 |
| 2MDM M2-1 D1-2-1 |
3 |
0.8 |
321 |
| 2MDM M2-1 D1-2-3-1 |
1 |
0.3 |
322 |
| 2MDM M2-1 D1-3-1 |
1 |
0.3 |
323 |
| 2MDM M2-1 D2-1 |
1 |
0.3 |
324 |
| 2MDM M2-1 D4-1 |
1 |
0.3 |
325 |
| 2MDM M2-1-2 D1 |
1 |
0.3 |
326 |
| 2MDM M2-1-2-1 D1 |
1 |
0.3 |
327 |
| 2MDM M2-3 D1 |
1 |
0.3 |
328 |
| 2MDM M2-3-1 D1 |
6 |
1.6 |
334 |
| 2MDM M2-3-1 D1-2-1 |
4 |
1.2 |
338 |
| 2MDM M2-3-2 D1 |
2 |
0.5 |
340 |
| 2MDM M2-3-2 D1-2-1 |
1 |
0.3 |
341 |
| 2MDM M2-4-2 D1 |
1 |
0.3 |
342 |
| 2MDM M3 D1-2 |
1 |
0.3 |
343 |
| 2MDM M3-1 D1 |
1 |
0.3 |
344 |
| 2MDM M3-2 D1 |
2 |
0.5 |
346 |
| 2MDM M3-2 D1-2-1 |
4 |
1.2 |
350 |
| 2MDM M3-2 D2-1 |
2 |
0.5 |
352 |
| 2MDM M3-2-1 D1 |
1 |
0.3 |
353 |
| 2MDM M4-1 D4-1 |
1 |
0.3 |
354 |
| 2MDM M4-2 D1 |
2 |
0.5 |
356 |
| 2MDM M4-2 D1-2-1 |
1 |
0.3 |
357 |
| 3MDM MB1 ML1 D1 |
4 |
1.2 |
361 |
| 3MDM MB1 ML2-1 D1-2 |
1 |
0.3 |
362 |
| 4MDM MB1 ML1 DB//DL1-2 |
2 |
0.5 |
364 |
| Total |
364 |
100 |
364 |
Table 4
Root canal configurations of mandibular second molar teeth with C-shaped anatomy according to the Ahmed et al. classification
| Configuration |
Number (n =) |
Total percentage (%) |
Cumulative total |
| (CSC1)1MDM1 |
1 |
4.5 |
1 |
| (CSC1)1MDM1-2 |
3 |
13.7 |
4 |
| (CSC1)1MDM1-2-3-2 |
1 |
4.5 |
5 |
| (CSC1)1MDM1-3-1 |
1 |
4.5 |
6 |
| (CSC2)1MDM2-3 |
1 |
4.5 |
7 |
| (CSC2)1MDM2-3-2 |
1 |
4.5 |
8 |
| (CSC3)1MDM2 |
1 |
4.5 |
9 |
| (CSC3)1MDM3 |
4 |
18.3 |
13 |
| (CSC3)1MDM3-1 |
1 |
4.5 |
14 |
| (CSC3)1MDM3-2 |
4 |
18.3 |
18 |
| (CSC3)1MDM3-2-1 |
1 |
4.5 |
19 |
| (CSC4)1MDM1 |
2 |
9.2 |
21 |
| (CSC4)1MDM1-2-3 |
1 |
4.5 |
22 |
| Total |
22 |
100 |
22 |
Effect of age and sex on canal configuration
No relationships between age and the Vertucci classification were demonstrated for the mesial root system (P = 0.49) or the distal root system (P = 0.60) of two-rooted teeth. Furthermore, no relationship was observed between sex and the Vertucci classification for the mesial root system (P = 0.23). In the distal root system, however, a relationship was observed between sex and the Vertucci classification (P = 0.02), males being more likely to display more than one canal in this root (P = 0.02).
With regard to age and the Ahmed et al. classification, no relationships were observed in either the mesial (P = 0.49) or distal root canal systems (P = 0.59). In the mesial root, no relationship was found between sex and the Ahmed et al. classification (P = 0.23). In the distal root system, a relationship between sex and the Ahmed et al. classification was observed (P = 0.02, Table 5), males being more likely to display additional canals in this root (P = 0.02).
No relationship between sex and the presence of C-shaped morphology was observed (P = 0.19).
Table 5
Sex versus Vertucci and Ahmed et al. classification in the distal root canal system of mandibular second molars
| Sex |
Single canals (n) |
Multiple canals (n) |
Female
(z-score) |
133
(0.385) |
31
(0.089) |
Male
(z-score) |
127
(0.368) |
54
(0.156) |
Fisher’s exact test: P = 0.02
Discussion
Knowledge of both conventional anatomy as well as anatomical variations is necessary for clinicians to locate, clean and fill entire root canal systems effectively [1,5]. It is well known that missed canals or untreated anatomy may negatively affect endodontic treatment outcomes [10]. Mandibular second molars in particular commonly display aberrations or variations of typical anatomy, and endodontic clinicians should be aware of all possible root and canal configurations in this tooth type in different population groups [5]. The present study confirmed this assertion for mandibular second molars in the Black South African population. As the study design was observational, descriptive and retrospective in nature, it was possible to evaluate a large number of samples, which were found to display both simple and complex morphology. This made it possible to compare the morphology of this tooth type and population group with previously reported populations.
Investigations pertaining to the dental anatomy of South African populations are limited [15], and no studies of mandibular second molars limited specifically to Black South African subjects could be found in the literature. The present study therefore provides new information regarding the dental morphology of the Black South African population living in the Southern African region. A previous study evaluated the root and canal morphology of mandibular first and second molars in a mixed South African population, but the findings were not limited to any particular population [Tredoux S, Root and canal configurations of mandibular molars using CBCT, with an emphasis on middle mesial canals. University of Pretoria (Dissertation): 1-75, 2020].
The mandibular second molars in the present study were predominantly two-rooted, and located mesiodistally. This corresponds with the findings of many others [5], and is historically considered to be a Caucasian trait [5]. However, root number in mandibular second molars may vary, being higher or lower [5], as was the case in the present sample. The prevalence of single-rooted teeth varies, but has been found in up to 41% of mandibular second molars [5]. The number of single-rooted teeth observed here was low, similar to the findings of Plotino et al. [2]. Three-rooted teeth were observed less commonly in the present study (1.6%), and have been reported less frequently than single- or double-rooted mandibular second molars [19]. The prevalence of three-rooted second molars in the present sample was similar to that reported for a Thai population (1.2%) but lower than that for Indian populations (8.9%) [8,20]. In the present investigation, three-rooted teeth were mainly observed as a splitting of the mesial root into separate mesiobuccal and mesiolingual roots with single canals, consistent with the findings of a previous South African study [Tredoux S, Dissertation: 1-75, 2020]. Only one radix entomolaris was observed, and this was considered a rare anatomical variation in this population. Some studies have reported four-rooted mandibular second molars, but this should also be considered uncommon [Tredoux S, Dissertation: 1-75, 2020]. Only two four-rooted teeth were found in the present sample, supporting this assertion.
C-shaped root and canal morphology is an important anatomical variation of mandibular second molars [5]. C-shapes have a wide range of reported prevalence (0-44.5%), but are more commonly found in Asian subjects [21]. C-shaped morphology is thought to be caused by failure of Hertwig’s epithelial root sheath to fuse on the buccal or lingual aspect of the root [22]. The presence of C-shape morphology has great clinical significance in endodontics, as these teeth have a complex internal morphology, requiring modification of cleaning, shaping and filling techniques [6], and may be vulnerable to coronal [23] and/or strip perforations [4]. This variation may additionally result in a variety of canal shapes [18], and the morphology may change along the length of the root [24], with no consistency [6]. This phenomenon was also observed in the present study (Fig. 3), and clinicians should be aware that the morphology evident in the coronal third of C-shaped teeth may not necessarily correspond to that found lower down the root [5], and may impact endodontic treatment. The present study reported a relatively low prevalence of C-shaped mandibular second molars (5.7%) in comparison with Korean [4], Saudi Arabian [25] and Sudanese [26] populations, and was similar to that of a White population [2] and another South African population [Tredoux S, Dissertation: 1-75, 2020]. Von Zuben et al. found a 9.3% prevalence of C-shaped mandibular second molars in a mixed South African population [27]. Rwenyonyi observed no C-shaped second molars in a Ugandan population [28]. Variation in the reported prevalence of C-shaped anatomy may be explained by differing study methodologies and sample sizes, population groups and CBCT machine parameters.
Racial and ethnic differences have previously been reported to influence anatomical variations in mandibular second molars [5]. Differing geographic location may also affect anatomical variation [7]. Future research aimed at describing the dental morphology of other Southern African populations would be desirable, as information from this region and the African continent in general is limited [28].
With regard to sex, a higher prevalence of C-shaped roots has been reported in females relative to males [5]. However, other investigations have found an opposite trend [3] or no such relationship [3]. The present study found no relationship between sex and C-shaped morphology. Age and tooth position of mandibular second molars have been reported to show no relationship in terms of anatomical variation [5]. Another South African study similarly found no age or sex correlations with root and canal configuration [Tredoux S, Dissertation: 1-75, 2020]. In the present study, no relationships between age and root canal anatomy were observed. However, males were found to display additional canals in the distal root canal system of mandibular second molars more frequently than females (P = 0.02).
The mandibular second molars observed in this Black South African population showed a wide variety of canal morphology. Single-rooted, non-C-shaped teeth had relatively simple single or double canal systems. Among two-rooted teeth, Type IV Vertucci configurations (two canals with two apical foramina) in the mesial root, and Type I (a single canal and foramen) in the distal root (Ahmed code: 2MDM M2 D1) were the structures most commonly observed. Although suggested by some to be an Asian trait [20], this feature has been reported in other ethnic groups [2]. This differed from American [29], Australian [22] and Turkish [12] studies, which found predominantly Type II (two canals with a single foramen) configurations in the mesial roots. However, Plotino et al. reported Type IV to be the most common configuration in a White population [2], as was the case in the present Black South African population. Three or more canals were found in almost one-fifth of mesial (n = 72/386, 18.6%) and some distal (n = 21/386, 5.4%) roots (Fig. 4A, B). This was similar to the findings of a previous study of a mixed South African population, where the prevalence of middle mesial canals was 17% and that of middle distal canals 2% [Tredoux S, Dissertation: 1-75, 2020]. This differed from the findings of Ahmed et al., who reported a 10% prevalence of both middle mesial and middle distal canals in mandibular second molars of a Sudanese population [26].
The present investigation used the classification systems of both Vertucci and Ahmed et al. [1,13]. Over time, the original eight Vertucci configurations were expanded to describe ever-increasing morphologic variations. The additions of Sert and Bayirli list 23 possible configurations [12], and this system has been used for the study of mandibular second molars [10]. Despite these additions, the Vertucci system remains unable to describe either root number or anomalies/variations [13]. Therefore, when using the Vertucci system some teeth invariably remain unclassified, as was confirmed in the present study. This should be considered a significant limitation of the Vertucci system. For this reason, C-shaped morphology has traditionally been described using alternative classifications, such as those originally proposed by Melton [24], and the additions made by Fan et al. [18]. In 2017, a new classification was created by Ahmed et al. to describe root and canal configurations simultaneously using a single descriptive code [13]. This system has the advantage of being able to describe anatomical variations and anomalies (such as C-shaped morphology) in addition to root and canal structures [17], as well as incorporating other classification systems (e.g. Fan et al. [18]) into the descriptive code for root and canal structures [17]. In the present study, this feature was used successfully, allowing all mandibular second molars to be described effectively. This should be considered a significant advantage over previous classification systems. One drawback of the Ahmed et al. system is that it creates several individual configurations, as was evident here. A limited number of investigations have compared the Ahmed et al. classification with other systems [14]. However, no previous attempts have been made to compare the Ahmed et al. system with the Vertucci classification system for description of mandibular second molars. Therefore, the present study may the first to have reported the anatomy of this tooth type with a comparison of these two classifications (including C-shaped morphology as part of the description), thereby improving knowledge and usage of the newer system for complex teeth.
The use of CBCT for the three-dimensional study of structures in the maxillofacial region, including endodontic anatomy, is well established [9]. The non-destructive nature of the technology allows retrospective evaluation of the prevalence of root and canal morphology in large samples [10,30]. The undistorted three-dimensional images of CBCT have been reported to be equal to those obtained by clearing and staining in studies of dental anatomy [31]. This imaging modality has been used by others for the study of mandibular second molars [14]. However, the 200-µm resolution used in the present investigation should be considered a limitation. Micro-CT is also popularly used for the study of root and canal morphology, but this technology cannot be used on living subjects [14].
In conclusion, the present study has revealed the diverse morphology of root and canal structures of mandibular second molars in a Black South African population. Two-rooted mandibular second molars were the type most commonly observed, and the prevalence of C-shaped anatomy was relatively low (5.7%). The most common canal configuration in the mesial roots was Vertucci Type IV (41.2%) and the Type I distal root (75.1%), or 2MDM M2 D1 as described by the Ahmed et al. classification. Three or more canals were found in a number of mesial (n = 72/386, 18.6%) and distal (n = 21/386, 5.4%) roots. Males demonstrated additional canals in the distal root canal system more frequently than females (P = 0.02). The use of CBCT, in combination with the Ahmed et al. classification, more effectively described the anatomy of mandibular second molars in comparison with the Vertucci classification. Clinicians must be cognisant of the existence of both normal root and canal morphology, as well as anatomical variations, in order to perform successful endodontic treatment on mandibular second molars.

Conflict of Interest
All authors substantially contributed to the study and agreed on the final text of the manuscript. This research did not receive any specific funding from agencies in the public, commercial, or not-for-profit sectors. The authors have no conflicts of interest to declare in relation to this study.
References
- 1. Vertucci FJ (1984) Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol 58, 589-599.
- 2. Plotino G, Tocci L, Grande NM, Testarelli L, Messineo D, Ciotti M et al. (2013) Symmetry of root and root canal morphology of maxillary and mandibular molars in a white population: a cone-beam computed tomography study in vivo. J Endod 39, 1545-1548.
- 3. Zheng Q, Zhang L, Zhou X, Wang Q, Wang Y, Tang L et al. (2011) C-shaped root canal system in mandibular second molars in a Chinese population evaluated by cone-beam computed tomography. Int Endod J 44, 857-862.
- 4. Seo DG, Gu Y, Yi YA, Lee SJ, Jeong JS, Lee Y et al. (2012) A biometric study of c-shaped root canal systems in mandibular second molars using cone-beam computed tomography. Int Endod J 45, 807-814.
- 5. Kim SY, Kim BS, Kim Y (2016) Mandibular second molar root canal morphology and variants in a Korean subpopulation. Int Endod J 49, 136-144.
- 6. Seo MS, Park DS (2004) C-shaped root canals of mandibular second molars in a Korean population: clinical observation and in vitro analysis. Int Endod J 37, 139-144.
- 7. Buchanan GD, Gamieldien MY, Tredoux S, Vally ZI (2020) Root and canal configurations of maxillary premolars in a South African subpopulation using cone beam computed tomography and two classification systems. J Oral Sci 62, 93-97.
- 8. Neelakantan P, Subbarao C, Subbarao CV, Ravindranath M (2010) Root and canal morphology of mandibular second molars in an Indian population. J Endod 36, 1319-1322.
- 9. Patel S, Durack C, Abella F, Shemesh H, Roig M, Lemberg K (2015) Cone beam computed tomography in endodontics – a review. Int Endod J 48, 3-15.
- 10. Tredoux S, Warren N, Buchanan GD (2021) Root and canal configurations of mandibular first molars in a South African subpopulation. J Oral Sci 63, 252-256.
- 11. Buchanan GD, Gamieldien MY, Fabris-Rotelli I, Van Schoor A, Uys A (2022) Root and canal morphology of maxillary second molars in a black South African subpopulation using cone-beam computed tomography and two classifications. Aust Endod J, Nov 14, doi: 10.1111/aej.12720.
- 12. Sert S, Bayirli GS (2004) Evaluation of the root canal configurations of the mandibular and maxillary permanent teeth by gender in the Turkish population. J Endod 30, 391-398.
- 13. Ahmed HMA, Versiani MA, De-Deus G, Dummer PMH (2017) A new system for classifying root and root canal morphology. Int Endod J 50, 761-770.
- 14. Ahmed HMA (2022) A critical analysis of laboratory and clinical research methods to study root and canal anatomy. Int Endod J 55, 229-280.
- 15. Buchanan GD, Gamieldien MY, Fabris-Rotelli I, Van Schoor A, Uys A (2022) Root and canal morphology of the permanent anterior dentition in a black South African population using cone-beam computed tomography and two classification systems. J Oral Sci 64, 218-223.
- 16. Fernandes NA, Herbst D, Postma TC, Bunn BK (2019) The prevalence of second canals in the mesiobuccal root of maxillary molars: a cone beam computed tomography study. Aust Endod J 45, 46-50.
- 17. Ahmed HMA, Ibrahim N, Mohamad NS, Nambiar P, Muhammad RF, Yusoff M et al. (2021) Application of a new system for classifying root and canal anatomy in studies involving micro-computed tomography and cone beam computed tomography: explanation and elaboration. Int Endod J 54, 1056-1082.
- 18. Fan B, Cheung GSP, Fan M, Gutmann JL, Bian Z (2004) C-shaped canal system in mandibular second molars: part I - anatomical features. J Endod 30, 899-903.
- 19. Zhang R, Wang H, Tian YY, Yu X, Hu T, Dummer PMH (2011) Use of cone-beam computed tomography to evaluate root and canal morphology of mandibular molars in Chinese individuals. Int Endod J 44, 990-999.
- 20. Gulabivala K, Opasanon A, Ng YL, Alavi A (2002) Root and canal morphology of Thai mandibular molars. Int Endod J 35, 56-62.
- 21. Yang ZP, Yang SF, Lin YC, Shay JC, Chi CY (1988) C-shaped root canals in mandibular second molars in a Chinese population. Endod Dent Traumatol 4, 160-163.
- 22. Manning SA (1990) Root canal anatomy of mandibular second molars. part I. Int Endod J 23, 34-39.
- 23. Jin GC, Lee SJ, Roh BD (2006) Anatomical study of c-shaped canals in mandibular second molars by analysis of computed tomography. J Endod 32, 10-13.
- 24. Melton DC, Krell KV, Fuller MW (1991) Anatomical and histological features of c-shaped canals in mandibular second molars. J Endod 17, 384-388.
- 25. Al-Fouzan KS (2002) C-shaped root canals in mandibular second molars in a Saudi Arabian population. Int Endod J 35, 499-504.
- 26. Ahmed HA, Abu-bakr NH, Yahia NA, Ibrahim YE (2007) Root and canal morphology of permanent mandibular molars in a Sudanese population. Int Endod J 40, 766-771.
- 27. Von Zuben M, Martins JNR, Berti L, Cassim I, Flynn D, Gonzalez JA et al. (2017) Worldwide prevalence of mandibular second molar c-shaped morphologies evaluated by cone-beam computed tomography. J Endod 43, 1442-1447.
- 28. Rwenyonyi CM, Kutesa A, Muwazi LM, Buwembo W (2009) Root and canal morphology of mandibular first and second permanent molar teeth in a Ugandan population. Odontology 97, 92-96.
- 29. Weine FS, Pasiewicz RA, Rice RT (1988) Canal configuration of the mandibular second molar using a clinically oriented in vitro method. J Endod 14, 207-213.
- 30. Buchanan GD, Gamieldien MY, Fabris-Rotelli I, Van Schoor A, Uys A (2022) A study of mandibular premolar root and canal morphology in a black South African population using cone-beam computed tomography and two classification systems. J Oral Sci 64, 300-306.
- 31. Neelakantan P, Subbarao C, Subbarao CV (2010) Comparative evaluation of modified canal staining and clearing technique, cone-beam computed tomography, peripheral quantitative computed tomography, spiral computed tomography, and plain and contrast medium-enhanced digital radiography in studying root canal morphology. J Endod 36, 1547-1551.


