Abstract
Introduction: The kickstand rod technique (KRT) is developed by Lenke et al. to correct residual intraoperative and postoperative coronal malalignment (CM) in thoracic-iliac corrective surgery. The iliac bone on the shift side is arranged through the usual median longitudinal skin incision and another iliac screw is added, and a closed-closed domino connector is placed at the thoracolumbar transition of the main rod on the shift side. A kickstand rod is placed between the added iliac screw and the domino connector, the set screws securing the two main rods are loosened except at the sacral and iliac regions, and a distraction force to correct is applied between the domino corrector and the distal rod grippers. Regarding CM after adult spinal deformity correction surgery, it is reported that CM remains in 60% and occurs iatrogenically in 9% of the cases postop. Insufficient correction of the lumbosacral fractional curve can result in oblique takeoff and cause CM. Here, we describe 3 cases of intraoperative additional correction of lumbar degenerative scoliosis with KRT for CM that remains after the usual correction procedure.
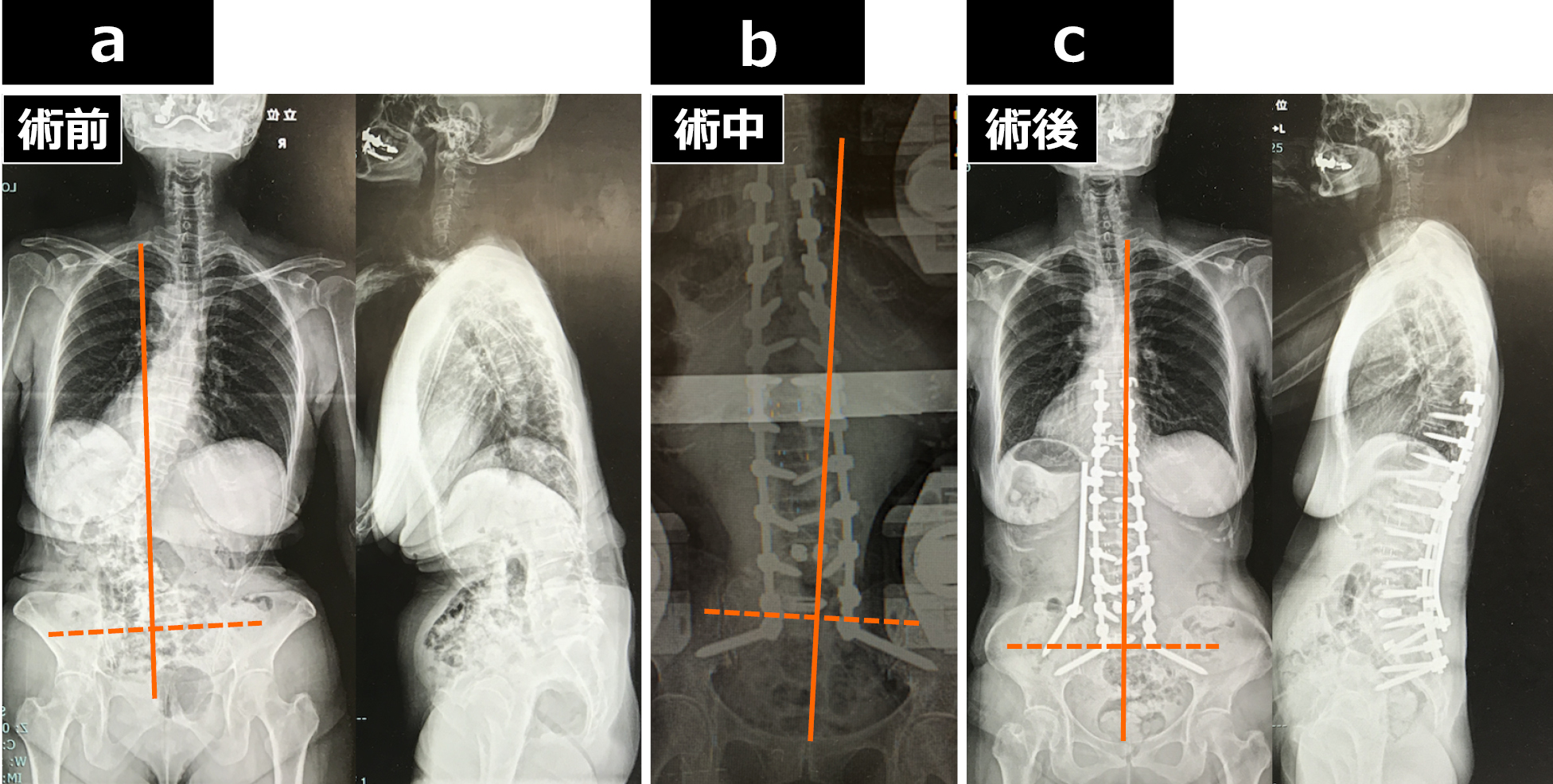
Case Report: The ages at surgery were 68, 73, and 74 years, and the preoperative distance between the C7 plumbline and center sacral vertical line (C7PL-CSVL) was 20, 65, and 33 mm. In each case, lateral interbody fusion (LIF) (L2/3-4/5, L2/3-4/5, L1/2-5/6) was performed anteriorly, and posterior fixation (9th thoracic vertebrae-ilium) was performed in two stages. Posterior lumbar interbody fusion was performed on the lower lumbar-sacral vertebrae that did not undergo LIF, and the fractional curve was corrected. Since CM remained in the intraoperative X-ray after the usual correction procedure, the additional correction was performed with KRT. The C7PL-CSVL was 13, 11, and 18 mm in the postoperative first standing position X-ray.
Conclusions: We experienced three cases of intraoperative additional correction with KRT for CM that remains after the usual correction procedure. KRT is a simple and useful procedure that can be the standard for spine surgeons.