Abstract
The aim of this study was to evaluate the effects of transcorneal electrical stimulation
in subjects with primary open-angle glaucoma. Five eyes of four male subjects with primary
open-angle glaucoma (average age: 52.25 ± 14.68 years) were enrolled. The subjects
underwent transcorneal electrical stimulation every 3 months according to the following
procedure. A Dawson-Trick-Litzkow electrode was placed on the cornea, and biphasic
electric current pulses (10 ms, 20 Hz) were delivered using a stimulator (BPG-1,BAK
Electronics) and a stimulus isolation unit (BSI-2). A current that evoked a phosphene that
the subject perceived in the whole visual area was delivered continuously for 30 min.
Humphrey visual field testing was performed after every third transcorneal electrical
stimulation treatment. Changes in mean deviation (MD) values were evaluated with a linear
regression model. Transcorneal electrical stimulation was performed 18.2 ± 9.4 times over
a period of 49.8 ± 23.0 months. The average pretranscorneal electrical stimulation
intraocular pressure, best corrected visual acuity, and MD values were 11.8 ± 1.79 mmHg,
0.14 ± 0.19 (logMAR) and −17.28 ± 6.24 dB, respectively. No significant differences were
observed in intraocular pressure before and after transcorneal electrical stimulation.
However, there was a significant positive linear relationship between changes in MD values
and the number of transcorneal electrical stimulation treatments (R2 = 0.176,
P = 0.005, Spearman correlation R =0.294, P = 0.008).
Transcorneal electrical stimulation treatment may improve glaucomatous visual field
defects in subjects with primary open-angle glaucoma. Large-scale studies are necessary to
confirm these preliminary findings.
Introduction
Glaucoma involves the progressive loss of retinal ganglion cells (RGCs) with concomitant
visual field (VF) loss. Reducing intraocular pressure (IOP) is an effective treatment for
open-angle glaucoma (OAG).1 However,
glaucomatous VF loss can be seen in some patients with normal IOP, suggesting that keeping
IOP low alone is not enough to inhibit glaucomatous optic neuropathy.
In a 1967 publication, Jarvik et al. reported the use of transcorneal electrical
stimulation (TES), a noninvasive procedure involving electrical neuro-retinal stimulation,
to treat retrograde amnesia in mice.2 Since
then, many studies have described the use of TES to treat various diseases, including eye
diseases. For example, Morimoto et al. reported that electrical stimulation has
neuroprotective effects after optic nerve transection in adult rats,3 and Fujikado et al. described the
neuroprotective effects of TES.4 TES has
also been found to delay the degeneration of photoreceptors and the impairment of retinal
function in Royal College of Surgeons rats used as an animal model of retinitis
pigmentosa.5 In clinical studies, TES
has been shown to improve visual acuity (VA) and/or VF in patients with various neuroretinal
diseases, including retinal artery occlusion (RAO), nonarteritic ischemic optic neuropathy,
Best vitelliform macular dystrophy, and traumatic optic neuropathy.6,7,8,9,10 TES also
leads to improved electroretinography (ERG) findings and VF in patients with retinitis
pigmentosa.11 To date, however, no
information is available concerning the long-term therapeutic effects of TES on
glaucoma.
The aim of this study was to evaluate the effects of TES on subjects with primary open
angle glaucoma (POAG).
Subjects and Methods
This was a prospective hospital-based case-series study carried out at Keio University
Hospital, Tokyo, Japan. It was approved by the Ethics Committee of Keio University School of
Medicine, and all procedures were in accordance with the Declaration of Helsinki. All
subjects gave written informed consent prior to enrolment.
Subjects
Five eyes of four male subjects with POAG were enrolled. The average age of the subjects
was 52.25 ± 14.68 years (mean ± standard deviation) (Table 1). Glaucoma specialists (NO, IK) carried out the following tests on all
subjects: best-corrected visual acuity (BCVA) measurement, IOP measurement (by Goldmann
applanation tonometry), slit lamp microscopy, gonioscopy, fundus examination, and visual
field measurement (with a Humphrey visual field analyzer [HFA]). All subjects were
familiar with HFA testing, having been subjected to it at least twice in the 9 months
before they entered the study. All subjects had typical glaucomatous optic disc cupping
and concomitant glaucomatous VF defects (mean deviation; MD <–12 dB). Average pre-TES
IOP, BCVA, and MD values were 11.8 ± 1.79 mmHg, 0.14 ± 0.19 (logMAR), and −17.28 ± 6.24
dB, respectively.
Table 1.
Clinical features of five eyes in four male patients with POAG
| Case |
Eye |
Type of glaucoma |
Age (years) |
VA pre-TES (LogMar) |
IOP pre-TES (mmHg) |
Baseline MD pre-TES (dB) |
| 1 |
R |
POAG |
34 |
0 |
9 |
−13.44 |
| 2 |
L |
NTG |
69 |
0.3 |
12 |
−28.14 |
| 3 |
R |
POAG |
57 |
0.4 |
12 |
−16.59 |
| 3 |
L |
POAG |
57 |
0 |
14 |
−12.95 |
| 4 |
L |
NTG |
49 |
0 |
12 |
−15.28 |
R, right eye; NTG, normal-tension glaucoma.
The baseline MD pre-TES values are the average of those obtained on the last two
examinations before TES.
The sensitivity of the visual field to the presented stimulus is recorded for each test
location. The threshold calculated for that point is compared to a database of normal
individuals of similar age. The average of these deviations over all test points is called
the mean deviation (MD).
TES procedure
The cornea and conjunctiva were anesthetized with 0.4% oxybuprocaine hydrochloride and
covered with 3% hyaluronic acid and 4% chondroitin sulfate (Viscoat, Alcon Japan, Tokyo,
Japan). A Dawson-Trick-Litzkow electrode (Tomey, Nagoya, Japan) was placed on the cornea
(Fig. 1a). Biphasic electric current pulses
were delivered using a stimulator (BPG-1, BAK Electronics, Mount Airy, MD, USA) through a
stimulus isolation unit (BSI-2, BAK Electronics) (Fig.
1b). The current of the pulses (duration: 10 ms, frequency: 20 Hz) was increased
to determine the threshold current necessary to elicit a phosphene. The current that
evoked a phosphene that the patient perceived over almost the whole visual area was
determined (409.38 ± 390.28 μA, [range 100–1800]), and this level of current was delivered
continuously for 30 min via biphasic pulses (Fig.
2). We performed stimulation with 300 μA or less when subjects felt brightness
throughout the visual field with 300 μA or less. When the brightness did not change even
with stimulation of more than 500 μA, we performed TES with an amplitude (300–500 μA) at
which patients did not feel pain on the skin. TES was performed in all cases by NO or
IK.

TES was performed once every 3 months. The examiners who performed VF testing were
blinded to TES treatment. Humphrey VF testing and multifocal ERG (mfERG) were performed
after every third TES treatment. During the course of the study, topical medication to
decrease IOP was administered as necessary.
Values analyzed
BCVA, IOP, and changes in MD values as determined with the HFA central 30–2 program
(Swedish Interactive Threshold algorithm 30–2) were analyzed. Changes in MD were
calculated as the MD value after TES treatment minus the value at baseline.
The mfERG findings were processed with Visual Evoked Response Imaging System software
(VERIS science 4.1.1, Mayo, Inazawa, Japan). The stimulus was composed of 61 hexagonal
elements, but hexagons lying on the horizontal midline were not used in the analysis. The
initial negative wave (N1) and the first positive peak (P1) were examined. We also
analyzed the latencies and amplitudes of both N1 and P1.
Statistical analysis
The Spearman correlation coefficient, a linear regression model, and a mixed effect model
were used to evaluate BCVA, IOP, changes in MD values, and N1 and P1 amplitudes and
latencies. SPSS software (version 23, IBM, NY, USA) was used for the analyses. A
P value less than 0.05 was considered statistically significant.
Results
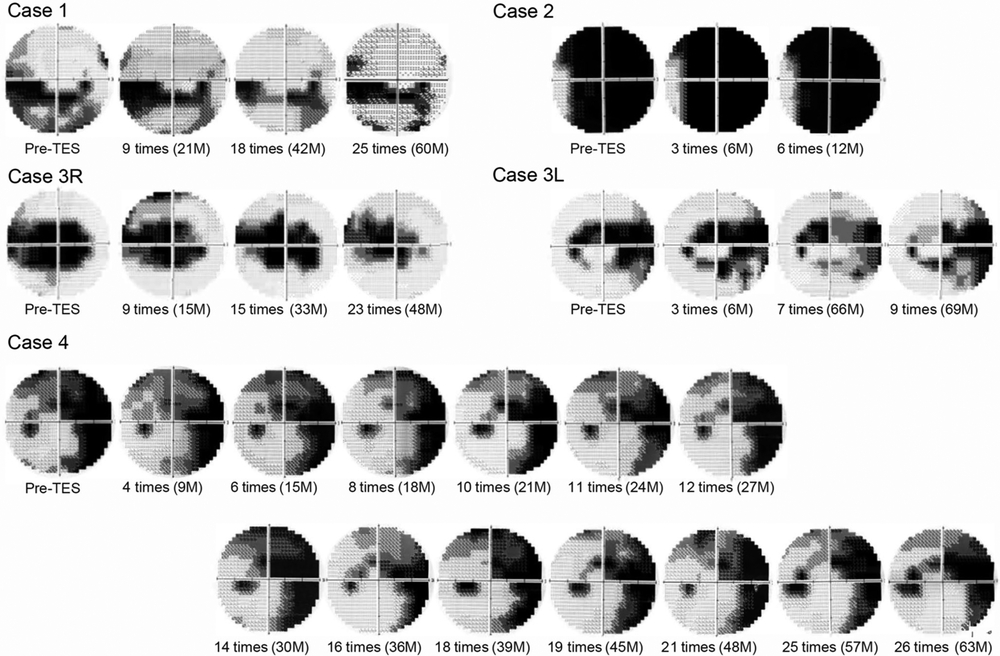
During the study period, TES was performed 18.2 ± 9.4 times (mean ± standard deviation,
range 6–27) over a period of 49.8 ± 23.0 months (range 11–68 months).
There was no significant change in MD value in any patient by linear regression analysis
(P > 0.05, Fig. 3 and 4).
However, there was a significant positive linear relationship between changes in MD values
and the number of TES treatments (R2 = 0.176, P = 0.005;
Spearman correlation R = 0.294, P = 0.008) (Fig. 5).


The average IOP before TES treatment was 11.8 mmHg, and at 6 months, 12 months, and 18
months after the series of TES interventions, it was 11.3 mmHg, 12.0 mmHg, and 15.7 mmHg,
respectively. Thus, there was no significant difference in IOP before and after TES
treatment (P > 0.05, mixed model). Nor was any significant difference
observed in N1 latency or amplitude in either the superior area or the inferior area before
and after TES treatment (P > 0.05, a mixed model, Fig. 6), or in P1 latency or amplitude in either area
(P > 0.05, mixed model, Fig.
7). BCVA at baseline was 0.14 ± 0.19 (mean ± standard deviation, logMAR), and after
the last TES it was 0.68 ± 0.90. All subjects had superficial punctate keratopathy after TES
treatment. One patient developed a cataract during the study period. Decreased VA in
association with the progression of glaucomatous VF loss was noted in only one eye during
TES treatment.
Discussion
This is the first study describing the effects of long-term TES treatment on patients with
glaucoma. It showed that the number of TES treatments is positively associated with changes
in MD values, suggesting that TES may improve RGC function.
An important issue is whether it is possible to improve VF in patients with glaucoma. It is
widely believed that genuine improvements in glaucomatous VF do not occur. Nevertheless, our
findings that TES improved glaucomatous VF is supported by several reports describing
improvements in glaucomatous VF defects in humans.12,13,14,15 Caprioli
et al. investigated the proportions of VF locations decaying or improving before and after
surgery in POAG patients treated with trabeculectomy: 30% of locations improved
preoperatively, and 44% improved postoperatively.16 In their control group, 34% of locations improved during the first half
of follow-up, and 35% improved during the second half of follow-up; a chi-squared comparison
of the rates of improvement in these two groups was statistically significant
(P < 0.0001), suggesting that trabeculectomy can improve glaucomatous
VF defects. Musch et al. also found that some patients participating in the Collaborative
Initial Glaucoma Treatment Study showed VF improvement over a long period after starting
initial treatment; they also showed, importantly, that measures of better IOP control during
treatment were significantly predictive of VF improvement, thereby indicating that
improvement was not just a learning effect or chance.17 Caprioli et al. attributed the improvements they observed in
glaucomatous VF loss to the revitalization of RGCs. We believe that TES may revitalize RGC
function by mimicking the IOP lowering effect of trabeculectomy, thereby improving
glaucomatous VF defects. However, the exact mechanism by which TES improves these defects
remains to be elucidated.
Morimoto et al. investigated the effects of TES after optic nerve (ON) transection in
rats.3,18 Seven days after transection, the number and
survival rate of RGCs were measured, and the RGC survival rate in the TES group was found to
be significantly higher than that in the controls. The levels of insulin-like growth factor
1 (IGF-1), a neurotrophic factor, in the retinas of rats not undergoing ON transection also
increased significantly after TES, as determined by RT-PCR and western blot analysis. In the
intact retina, IGF-1 is located in the basal endfeet of Muller cells,3 and TES promotes the level of IGF-1 secretion
from Muller cells. A high dose of JB-3, an IGF-1 receptor antagonist, reduced the survival
of RGCs after TES in rats undergoing ON transection.3 These results indicate that IGF-1 plays a role in the survival of
injured RGCs.
Tagami et al. reported that axonal regeneration after ON transection was promoted by daily
TES treatment in rats.19 This result was
also related to IGF-1 levels. TES may promote RGC function by promoting axonal regeneration
in human POAG patients.
Another possible explanation for improved VF is increased ocular blood flow. Inomata et al.
showed that the light reflectance changes in the posterior retina induced by TES were slow
in two healthy rhesus monkeys, and also that there was a strong correlation between the slow
components of the intrinsic signal and blood flow changes.20 This finding suggests that TES increases blood flow. Kurimoto
et al. reported that chorioretinal blood flow midway between the optic disc and the macula
increased after TES in healthy human subjects.21 The Leuven Eye Study showed that patients with OAG had lower blood
velocities in the central retinal vessels than the controls did.22 From these studies, we can hypothesize that TES has an effect
on the retinal vessels and improves chorioretinal blood flow, which may improve RGC
function.
Our study revealed no significant differences in latencies and amplitudes on ERG before and
after TES, suggesting that the side effects of TES on retinal function in POAG subjects is
minimal. Shatz et al. demonstrated that latencies and amplitudes on ERG in patients with
retinitis pigmentosa during TES treatment did not change significantly,11 and Naycheva et al. also reported similar
results in RAO subjects before and after TES.8 However, some researchers have reported improved mfERG responses. Oono et
al. reported significant reductions in N1 and P1 latency after TES in subjects with RAO,
although the N1 and P1 amplitudes did not change significantly.9 Inomata et al. demonstrated that N1 and P1 amplitudes improved
significantly after TES in some patients with longstanding RAO.10 Although differing mfERG responses have been reported in
previous TES studies, at least no deterioration in responses after TES treatment has been
reported, which indicates that TES has no harmful effects on the retina. In 2015, Machida et
al. reported that a focal photopic negative response on the ERG indicates RGC function in
OAG subjects.23 In future studies, it
would be helpful to use focal macular ERG or full-field photopic ERG to objectively evaluate
RGC function.
Many studies have shown improved BCVA after TES in subjects with nonarteritic ischemic
optic neuropathy, RAO, traumatic optic neuropathy, or Best vitelliform macular
dystrophy.6,7,10 However, we observed no improvements in BCVA in our study. This may be
partially explained by the specific conditions of two of our subjects. In case 2, slight
changes were difficult to detect because central VF had already been lost before TES. This
patient experienced central vision loss, probably as a result of the progression of
glaucomatous VF loss. In case 4, we could not evaluate the actual effect of TES on BCVA
because the patient developed a cataract. After the study, this patient had cataract
surgery, following which BCVA improved. Further study is needed to evaluate the effects of
TES on BCVA in subjects with POAG.
As far as we know, no studies examining the effects of TES on IOP have been reported, but
our study revealed no significant differences in IOP before and after TES treatment.
Reducing IOP is the standard treatment for glaucoma, so we gave our subjects topical
IOP-lowering drugs, and IOP was maintained at a low level. Therefore, we could not confirm
whether the effects on glaucoma we saw were the result of IOP control or TES treatment,
although we can say that VF loss may have progressed without TES. For confirmation, we need
to carry out further studies with a control group.
This study is subject to several limitations. First, we did not have a control group. It is
possible that improvements in VF might have been observed in a control group, although, in
general, glaucomatous VF defects do not improve. Second, our sample of POAG patients
undergoing TES treatment was small. Third, we changed the topical anti-glaucoma treatment
during the study period, which may have affected our results.
In conclusion, patients with POAG are able to tolerate TES treatment for long periods, and
TES may have beneficial therapeutic effects in some cases of progressive glaucomatous optic
neuropathy. Large-scale studies are necessary to confirm our preliminary findings.
Source of support
The authors received no financial support for this study.
Conflict of Interest
We have no conflict of interest to declare.
References
- 1. Coleman AL, Miglior S: Risk factors for glaucoma
onset and progression. Surv Ophthalmol 2008; 53(Suppl1): S3–S10.
- 2. Jarvik ME, Kopp R: Transcorneal electroconvulsive
shock and retrograde amnesia in mice. J Comp Physiol Psychol 1967; 64:
431–433.
- 3. Morimoto T, Miyoshi T, Matsuda S, Tano Y,
Fujikado T, Fukuda Y: Transcorneal electrical stimulation rescues axotomized retinal
ganglion cells by activating endogenous retinal IGF-1 system. Invest Ophthalmol Vis Sci
2005; 46: 2147–2155.
- 4. Fujikado T: Development of a new evaluation
system for visual function. Nippon Ganka Gakkai Zasshi 2004; 108: 809–834, discussion 835.
[in Japanese]
- 5. Morimoto T, Fujikado T, Choi JS, Kanda H, Miyoshi
T, Fukuda Y, Tano Y: Transcorneal electrical stimulation promotes the survival of
photoreceptors and preserves retinal function in Royal College of Surgeons rats. Invest
Ophthalmol Vis Sci 2007; 48: 4725–4732.
- 6. Ozeki N, Shinoda K, Ohde H, Ishida S, Tsubota K:
Improvement of visual acuity after transcorneal electrical stimulation in case of Best
vitelliform macular dystrophy. Graefes Arch Clin Exp Ophthalmol 2013; 251:
1867–1870.
- 7. Fujikado T, Morimoto T, Matsushita K, Shimojo H,
Okawa Y, Tano Y: Effect of transcorneal electrical stimulation in patients with
nonarteritic ischemic optic neuropathy or traumatic optic neuropathy. Jpn J Ophthalmol
2006; 50: 266–273.
- 8. Naycheva L, Schatz A, Willmann G, Bartz-Schmidt
KU, Zrenner E, Röck T, Gekeler F: Transcorneal electrical stimulation in patients with
retinal artery occlusion: a prospective, randomized, sham-controlled pilot study.
Ophthalmol Ther 2013; 2: 25–39.
- 9. Oono S, Kurimoto T, Kashimoto R, Tagami Y,
Okamoto N, Mimura O: Transcorneal electrical stimulation improves visual function in eyes
with branch retinal artery occlusion. Clin Ophthalmol 2011; 5: 397–402.
- 10. Inomata K, Shinoda K, Ohde H, Tsunoda K, Hanazono
G, Kimura I, Yuzawa M, Tsubota K, Miyake Y: Transcorneal electrical stimulation of retina
to treat longstanding retinal artery occlusion. Graefes Arch Clin Exp Ophthalmol 2007;
245: 1773–1780.
- 11. Schatz A, Röck T, Naycheva L, Willmann G, Wilhelm
B, Peters T, Bartz-Schmidt KU, Zrenner E, Messias A, Gekeler F: Transcorneal electrical
stimulation for patients with retinitis pigmentosa: a prospective, randomized,
sham-controlled exploratory study. Invest Ophthalmol Vis Sci 2011; 52:
4485–4496.
- 12. Salim S, Paranhos A, Lima M, Shields MB:
Influence of surgical reduction of intraocular pressure on regions of the visual field
with different levels of sensitivity. Am J Ophthalmol 2001; 132: 496–500.
- 13. Vuori ML, Vainio-Jylhä E, Viitanen TT: Localised
changes in glaucomatous visual fields after trabeculectomy. Acta Ophthalmol Scand 2001;
79: 468–471.
- 14. Yildirim E, Bilge AH, Ilker S: Improvement of
visual field following trabeculectomy for open angle glaucoma. Eye (Lond) 1990; 4:
103–106.
- 15. Folgar FA, de Moraes CG, Prata TS, Teng CC, Tello
C, Ritch R, Liebmann JM: Glaucoma surgery decreases the rates of localized and global
visual field progression. Am J Ophthalmol 2010; 149: 258–264.e2.
- 16. Caprioli J, de Leon JM, Azarbod P, Chen A,
Morales E, Nouri-Mahdavi K, Coleman A, Yu F, Afifi A: Trabeculectomy can improve long-term
visual function in glaucoma. Ophthalmology 2016; 123: 117–128.
- 17. Musch DC, Gillespie BW, Palmberg PF, Spaeth G,
Niziol LM, Lichter PR: Visual field improvement in the collaborative initial glaucoma
treatment study. Am J Ophthalmol 2014; 158: 96–104.e2.
- 18. Morimoto T, Miyoshi T, Sawai H, Fujikado T:
Optimal parameters of transcorneal electrical stimulation (TES) to be neuroprotective of
axotomized RGCs in adult rats. Exp Eye Res 2010; 90: 285–291.
- 19. Tagami Y, Kurimoto T, Miyoshi T, Morimoto T,
Sawai H, Mimura O: Axonal regeneration induced by repetitive electrical stimulation of
crushed optic nerve in adult rats. Jpn J Ophthalmol 2009; 53: 257–266.
- 20. Inomata K, Tsunoda K, Hanazono G, Kazato Y,
Shinoda K, Yuzawa M, Tanifuji M, Miyake Y: Distribution of retinal responses evoked by
transscleral electrical stimulation detected by intrinsic signal imaging in macaque
monkeys. Invest Ophthalmol Vis Sci 2008; 49: 2193–2200.
- 21. Kurimoto T, Oono S, Oku H, Tagami Y, Kashimoto R,
Takata M, Okamoto N, Ikeda T, Mimura O: Transcorneal electrical stimulation increases
chorioretinal blood flow in normal human subjects. Clin Ophthalmol 2010; 4:
1441–1446.
- 22. Abegão Pinto L, Willekens K, Van Keer K, Shibesh
A, Molenberghs G, Vandewalle E, Stalmans I: Ocular blood flow in glaucoma – the Leuven Eye
Study. Acta Ophthalmol 2016; 94: 592–598.
- 23. Machida S, Kaneko M, Kurosaka D: Regional
variations in correlation between photopic negative response of focal electroretinograms
and ganglion cell complex in glaucoma. Curr Eye Res 2015; 40: 439–449.



