Abstract
Proton pump inhibitors (PPIs) are widely used medicines worldwide. However, a rare
etiology of syndrome of inappropriate secretion of antidiuretic hormone (SIADH) related to
PPI was recently reported. Therefore, the putative role of PPIs in SIADH cannot be
underestimated. A 78-year-old Japanese woman was admitted to our hospital for treatment of
left Bell’s palsy. On admission, the patient was oriented with normal laboratory data,
including a serum Na level of 135 mEq/L. Oral glucocorticoids and a proton pump inhibitor
were initiated in combination with oral valaciclovir. Six days later, the patient’s
consciousness became impaired. Laboratory data showed a serum Na level of 103 mEq/L, a
urine Na level of 64.8 mEq/L, a urine K level of 43.6 mEq/L, and a urine osmolality of 450
mOsm/kg H2O. The patient met the criteria for SIADH. The initial treatment
included water restriction and 3% hypertonic saline administration. The cessation of PPI
significantly improved the urine diluting capacity and concomitantly increased serum Na,
which indicated that the use of PPI had been responsible for the etiology of SIADH. The
present case illustrates that physicians need to be aware of the uncommon adverse effects
of PPI, such as SIADH.
Introduction
Hyponatremia, defined as a serum Na concentration below 135 mEq/L, is a condition
characterized by an excess of water without Na deficit caused by impaired excretion of free
water.1 Renal free water excretion is
tightly regulated by the serum antidiuretic hormone (ADH). In normal conditions, the serum
osmolality plays an important role in regulating ADH release. An increase in serum
osmolality of even 1% significantly increases serum ADH, with a proportional increase in
urine concentration.2
In contrast to the normal response to serum osmolality, the syndrome of inappropriate
secretion of ADH (SIADH) is a condition in which ADH is disproportionally secreted
regardless of the serum osmolality. This inappropriate secretion results in water retention
and subsequent hyponatremia. There are several etiologies of SIADH, including central
nervous system disturbances, malignancy, recent surgery, and drugs.3
Proton pump inhibitors (PPIs) are one of the most widely administered drugs worldwide.
However, there has been a growing concern that PPI use is associated with various adverse
effects, including cardiovascular diseases,4Clostridium difficile infection,5 bone fractures,6 kidney damage, and electrolyte disturbances.7,8
Although electrolyte disturbances were considered to be a relatively rare side effect,
hypomagnesemia, hypocalcemia, and hypokalemia have been reported.8 Hyponatremia related to PPI administration is less common, and
its pathophysiology remains to be elucidated. Herein, we present the case of a female
patient with hyponatremia due to SIADH, which might have been related to PPI use.
Case Presentation
A 78-year-old Japanese woman with hyponatremia was referred to the Nephrology Department
for evaluation. Six days earlier, the patient had been transferred to the
Otorhinolaryngology Department because of the sudden onset of left facial paralysis. The
patient’s medical history included hypothyroidism and she had been administered
levothyroxine. On admission, the patient was alert and oriented. Cranial nerve examination
demonstrated the inability to generate wrinkles on the left side of the forehead, loss of
the left nasolabial fold, loss of taste sensation, and drooping of the left corner of the
mouth. The patient did not drink alcohol, smoke tobacco, or use supplements. Laboratory
tests were normal for kidney function, liver function, and electrolytes, including a serum
Na level of 135 mEq/L (Table 1). Brain magnetic
resonance imaging revealed no abnormalities in the internal auditory canal or the
cerebellopontine angle. The patient was diagnosed with left Bell’s palsy. A dose of
50 mg/day of oral glucocorticoids was initiated. Proton pump inhibitor (esomeprazole)
administration was concomitantly initiated to prevent glucocorticoid-induced gastric ulcer.
Oral valaciclovir was also prescribed for 7 days.
Table 1.
Blood and urinary analysis on admission and on days 6 and 11
|
Day 1 |
Day 6 |
Day 11 |
| Serum |
|
|
|
| Na mEq/L |
135 |
103 |
132 |
| K mEq/L |
3.7 |
3.5 |
3.2 |
| Cl mEq/L |
97 |
72 |
87 |
| BUN mg/dL |
10.6 |
7.6 |
7.6 |
| Creatinine mg/dL |
0.71 |
0.42 |
0.63 |
| Uric acid mg/dL |
4.4 |
1.9 |
3.1 |
| Alb |
4.0 |
3.9 |
3.0 |
| Osmolality mOsm/kg H2O |
- |
218 |
- |
| ADH pg/mL |
- |
27.4 |
- |
| Cortisol µg/dL |
- |
30.8 |
- |
| TSH µUI/mL |
- |
3.43 |
- |
| Free T4 ng/mL |
- |
1.39 |
- |
| Urine |
|
|
|
| Na mEq/L |
- |
64.8 |
59.6 |
| K mEq/L |
- |
43.6 |
10.2 |
| Cr mg/dL |
- |
39.3 |
25.2 |
| Osmolality mOsm/kg H2O |
- |
450 |
243 |
ADH, anti diuretic hormone; BUN, blood urea nitrogen; TSH, thyroid stimulating hormone;
T4, Thyroxine 4.
On the sixth day of hospitalization, the patient’s consciousness was impaired. Laboratory
tests showed a serum Na level of 103 mEq/L, a urine Na level of 64.8 mEq/L, a urine K level
of 43.6 mEq/L, and a urine osmolality of 450 mOsm/kg H2O (Table 1). The possible etiologies of hyponatremia were evaluated.
During hospitalization, the patient ate about 50% of her meals (because of loss of taste
sensation) and took about 500–700 mL of fluid in addition to meals. However, the patient
denied any vomiting, diarrhea, or polydipsia. Medications associated with hyponatremia, such
as antidepressants, anticonvulsants, antipsychotics, and vasopressin analogs, were not used.
On examination, the vital signs were unremarkable, with a blood pressure of 118/60 mm Hg, a
temperature of 36.5°C, and a heart rate of 68 beats/min. Physical examination showed no
peripheral edema and no abnormal heart or respiratory sounds. The patient history and
physical examination indicated that the patient was euvolemic. Additional laboratory
examinations ruled out hypothyroidism or adrenal insufficiency. Inadequate oral intake might
have contributed to the development of hyponatremia; however, it is not likely that this
alone caused such a sudden decrease in serum Na levels from 135 to 103 mEq/L. As an
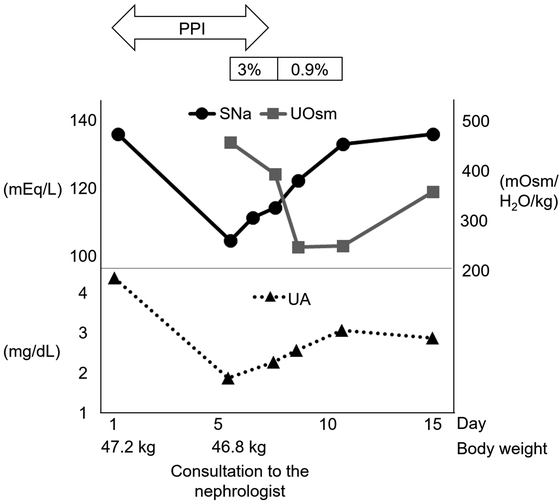
underlying etiology of hyponatremia, SIADH has been suggested. Initial treatment was
performed with fluid restriction combined with administration of 3% hypertonic saline at
0.6 mL/kg/h (Fig. 1). Hypertonic saline (3%) was
used because the patient’s urine tonicity (urine Na + urine K) exceeded serum Na, which
indicated that free water excretion was impaired and spontaneous improvement of serum Na
seemed unlikely. After 2 days, serum Na improved to 113 mEq/L with a urine Na level of 33.1
mEq/L, a urine K level of 25.7 mEq/L, and a urine osmolality of 386 mOsm/kg H2O.
At this point, the patient’s urine Na and urine osmolality were still elevated. Therefore,
drug-induced SIADH was suspected. The medications used during hospitalization included
glucocorticoids, levothyroxine, valaciclovir, and a proton pump inhibitor. The proton pump
inhibitor was considered to be the likely causative factor for SIADH and was discontinued.
Subsequently, serum Na gradually increased with a concomitant decrease in urine osmolarity.
Administration of hypertonic saline was switched from 3% to 0.9% at 1 mL/kg/h until the
patient could take enough food. She was discharged on the 15th day of hospitalization with a
serum Na level of 135 mEq/L. Written informed consent was obtained from the patient for
reporting this case.
Discussion
The underlying mechanism of hyponatremia related to PPI use remains to be fully elucidated.
However, as an underlying etiology of hyponatremia, administration of PPI was likely
responsible for the development of SIADH in some cases.9,10,11 There are
several test results that point to a diagnosis of SIADH. First, the presence of decreased
urine diluting capacity is the essential feature of SIADH.12 For example, hyponatremia with high urine concentration
(usually >300 mOsm/kg H2O) is a good indication that should raise the
suspicion of SIADH. Second, SIADH is mostly associated with euvolemic
hyponatremia.13,14 Urine Na levels combined with physical
examinations are useful to evaluate volume status. A previous study illustrated the
diagnostic value of urine Na levels in hyponatremic patients without edema. It showed that
the mean urine Na was 72 mEq/L in patients with euvolemia (SIADH) compared to 18 mEq/L in
patients with hypovolemic hyponatremia.13
Third, the coexistence of hypouricemia (<4 mg/dL) with increased fractional excretion of
uric acid (FEUA) is often observed in patients with SIADH.15 Interestingly, in patients with SIADH, the improvement in
hypouricemia and FEUA was concomitantly observed with the increase in
hyponatremia.16 Lastly, before SIADH
is diagnosed, other etiologies of euvolemic hyponatremia, including polydipsia,
malnutrition, glucocorticoid deficiency, and hypothyroidism, should be excluded.
In our case, the clinical history and physical examination results suggested that the
patient was euvolemic. The presence of high urine osmolality, high urine Na concentration,
and the concomitant improvement in hyponatremia and hypouricemia were all consistent with
the characteristics of SIADH. Finally, the detection of an elevated serum ADH level
confirmed the diagnosis of SIADH. Before consultation, intravenous fluid was not
administered; therefore, iatrogenic hypotonic fluid-induced hyponatremia was ruled out.
Other causes of hyponatremia, including polydipsia, hypovolemic hyponatremia, heart failure,
liver cirrhosis, adrenal insufficiency, thyroid dysfunction, and renal salt wasting, were
all ruled out. The cessation of PPI significantly improved urine osmolarity and
concomitantly increased serum Na. Although PPI-induced SIADH is considered to be rare,
recent studies have reported this possibility.9,10,11
Concomitant with previous reports, we interpreted our clinical course as the putative
involvement of PPI in SIADH. Therefore, we propose that physicians should consider PPI as a
possible cause of SIADH. In general, some mechanisms of drug-induced SIADH are
known.17 For example, carbamazepine
and oxcarbazepine reportedly increase sensitivity to ADH. Chlorpropamide increases the
number of vasopressin-2 (V2; antidiuretic) receptors in collecting tubules. Abuse of
methylenedioxymethamphetamine is associated with the direct release of ADH and stimulation
of thirst, which further worsens hyponatremia. However, PPI-induced SIADH is less common;
therefore, the precise mechanism remains unclear and more research is needed.
PPIs are also known to cause acute interstitial nephritis (AIN). If PPI-induced AIN occurs
concomitantly with SIADH, it will disturb free water excretion and exacerbate hyponatremia.
It is important for physicians to evaluate whether AIN contributes to the development of
hyponatremia. In our case, the patient did not show any allergic-type symptoms related to
AIN and laboratory data did not indicate AIN, e.g., increased levels of eosinophilia or
eosinophiluria. Therefore, we excluded the possibility of PPI-induced AIN. Furthermore, the
possible contribution of valacyclovir to the development of hyponatremia should be
addressed. A previous report described a patient who received valacyclovir and developed
acute kidney injury concomitant with hyponatremia.18 Another report involved a patient who was administered acyclovir and
developed hyponatremia.19 The latter
report proposed a possible mechanism of hyponatremia due to SIADH, which might have been
caused by herpes zoster virus infection and the administration of acyclovir. However, a
causative relationship between valacyclovir and hyponatremia remains inconclusive. We
speculate that the administration of valacyclovir in our case might have accelerated the
development of PPI-induced SIADH.
Whether the type of PPI or the duration of PPI administration influences the development of
hyponatremia remains unclear. One previous study showed that the hyponatremia effect was
most pronounced for omeprazole, followed by lansoprazole and rabeprazole.8 In our case, esomeprazole was considered to be
responsible for SIADH. Therefore, it should be noted that all types of PPI could be
responsible for SIADH. Another study found that moderate hyponatremia was observed in
18.7–46.3% of elderly patients who took PPI for more than 1 year.20 In our case, both the onset and improvement of hyponatremia
occurred quickly compared to previous cases.20,21 We
speculate that the susceptibility to PPIs might vary between individuals.
In conclusion, we presented the case of a patient who rapidly developed hyponatremia that
might have been related to PPI use. We emphasize that it is important to realize the
uncommon adverse effect of PPIs, such as SIADH, regardless of the type of PPI or duration of
use. This advice will help physicians to provide appropriate patient management in clinical
practice.
Conflicts of Interest
The authors declare that no conflicts of interest exist.
References
- 1. Adrogué HJ, Madias NE: Hyponatremia. N Engl J Med
2000; 342: 1581–1589. PMID:10824078, DOI:10.1056/NEJM200005253422107
- 2. Robinson AG: Disorders of antidiuretic hormone
secretion. Clin Endocrinol Metab 1985; 14: 55–88. PMID:3893810,
DOI:10.1016/S0300-595X(85)80065-7
- 3. Ellison DH, Berl T: Clinical practice. The
syndrome of inappropriate antidiuresis. N Engl J Med 2007; 356: 2064–2072. PMID:17507705,
DOI:10.1056/NEJMcp066837
- 4. Davis TM, Drinkwater J, Davis WA: Proton pump
inhibitors, nephropathy, and cardiovascular disease in type 2 diabetes: The Fremantle
Diabetes Study. J Clin Endocrinol Metab 2017; 102: 2985–2993. PMID:28591820,
DOI:10.1210/jc.2017-00354
- 5. Trifan A, Stanciu C, Girleanu I, Stoica OC,
Singeap AM, Maxim R, Chiriac SA, Ciobica A, Boiculese L: Proton pump inhibitors therapy
and risk of Clostridium difficile infection: systematic review and meta-analysis. World J
Gastroenterol 2017; 23: 6500–6515. PMID:29085200,
DOI:10.3748/wjg.v23.i35.6500
- 6. Sugiyama T, Watarai K, Oda T, Kim YT, Oda H:
Proton pump inhibitors and fracture: they impair bone quality and increase fall risk?
Osteoporos Int 2016; 27: 1675–1676. PMID:26860500,
DOI:10.1007/s00198-016-3509-7
- 7. Rosenberg K: Proton-pump inhibitor use associated
with kidney injury, electrolyte abnormalities. AJN, Am J Nurs 2019; 119: 68–69.
PMID:31135439, DOI:10.1097/01.NAJ.0000559812.67424.47
- 8. Makunts T, Cohen IV, Awdishu L, Abagyan R:
Analysis of postmarketing safety data for proton-pump inhibitors reveals increased
propensity for renal injury, electrolyte abnormalities, and nephrolithiasis. Sci Rep 2019;
9: 2282. PMID:30783195, DOI:10.1038/s41598-019-39335-7
- 9. Durst RY, Pipek R, Levy Y: Hyponatremia caused by
omeprazole treatment. Am J Med 1994; 97: 400–401. PMID:7942948,
DOI:10.1016/0002-9343(94)90313-1
- 10. Naharcý MI, Cintosun U, Ozturk A, Bozoglu E,
Doruk H: Pantoprazole sodium-induced hyponatremia in a frail elderly adult. J Am Geriatr
Soc 2014; 62: 787–788. PMID:24731036, DOI:10.1111/jgs.12767
- 11. Engelen A, Christiaens P, Bossuyt P, Cuyle PJ,
Van Olmen A, Carton S, Moons V: Syndrome of inappropriate antidiuretic hormone secretion
caused by proton pump inhibitor use. Acta Gastroenterol Belg 2018; 81: 542.
PMID:30645929
- 12. Disorders of Water Balance. In: Karl S, Glenn MC,
Philip AM, Maarten WT, Alan SLY, eds, Brenner and Rector’s The Kidney, Elsevier, 2015, pp.
540–594.
- 13. Chung HM, Kluge R, Schrier RW, Anderson RJ:
Clinical assessment of extracellular fluid volume in hyponatremia. Am J Med 1987; 83:
905–908. PMID:3674097, DOI:10.1016/0002-9343(87)90649-8
- 14. Decaux G, Musch W: Clinical laboratory evaluation
of the syndrome of inappropriate secretion of antidiuretic hormone. Clin J Am Soc Nephrol
2008; 3: 1175–1184. PMID:18434618, DOI:10.2215/CJN.04431007
- 15. Beck LH: Hypouricemia in the syndrome of
inappropriate secretion of antidiuretic hormone. N Engl J Med 1979; 301: 528–530.
PMID:460306, DOI:10.1056/NEJM197909063011005
- 16. Maesaka JK, Imbriano LJ, Ali NM, Ilamathi E: Is
it cerebral or renal salt wasting? Kidney Int 2009; 76: 934–938. PMID:19641485,
DOI:10.1038/ki.2009.263
- 17. Yasir M, Mechanic OJ: Syndrome of Inappropriate
Antidiuretic Hormone Secretion (SIADH). In: StatPearls [Internet]. Treasure Island (FL):
StatPearls Publishing; 2020 Jan. Last Update: April 14, 2020.
- 18. Murakami T, Akimoto T, Okada M, Hishida E, Sugase
T, Miki A, Kohara M, Yoshizawa H, Masuda T, Kobayashi T, Saito O, Muto S, Nagata D:
Valacyclovir neurotoxicity and nephrotoxicity in an elderly patient complicated by
hyponatremia. Drug Target Insights 2018; 12: 1177392818782899. PMID:30013310,
DOI:10.33393/dti.2018.1400
- 19. Kucukardali Y, Solmazgul E, Terekeci H, Oncul O,
Turhan V: Herpes zoster ophthalmicus and syndrome of inappropriate antidiuretic hormone
secretion. Intern Med 2008; 47: 463–465. PMID:18310984,
DOI:10.2169/internalmedicine.47.0629
- 20. Buon M, Gaillard C, Martin J, Fedrizzi S, Mosquet
B, Coquerel A, Peyro Saint Paul L: Risk of proton pump inhibitor-induced mild hyponatremia
in older adults. J Am Geriatr Soc 2013; 61: 2052–2054. PMID:24219214,
DOI:10.1111/jgs.12534
- 21. Ferreira F, Mateus S, Santos AR, Moreira H,
Ferreira N: Pantoprazole-related symptomatic hyponatremia. Eur J Case Rep Intern Med 2016;
3: 1. PMID:30755856, DOI:10.12890/2015_000341
