Abstract
Anemia in chronic kidney disease (CKD) is a risk factor for cardiovascular diseases and
is treated by long-acting erythropoiesis-stimulating agents (ESA). Although results of
previous studies showed that the hemoglobin level could not be maintained at initiation of
dialysis in CKD patients treated with recombinant human erythropoietin, it remains
undetermined if long-acting ESA are effective to prevent the progression of anemia at
initiation of dialysis. In the present study, hemoglobin levels in 40 CKD patients treated
with darbepoetin alfa (DA) and 15 CKD patients treated with a continuous erythropoietin
receptor activator (CERA) were retrospectively compared during the 6 months period prior
to initiation of dialysis. Results showed that DA and CERA, respectively, maintained
hemoglobin levels around 10 g/dL from 6 months to 1 month before dialysis. However,
hemoglobin levels at initiation of dialysis were significantly decreased to 9.1 ± 1.2 g/dL
in DA group and 9.0 ± 1.0 g/dL in CERA group, respectively. Although total doses of ESA
used for 6 months were similar between two groups, DA-treated CKD patients received
subcutaneous injections more frequently than patients treated with CERA. These results
suggest that CKD patients are needed to receive more intense ESA therapy to prevent a
decline in hemoglobin levels at initiation of dialysis, even under the use of long-acting
ESA, and also raise a possibility that CERA is more useful than DA to reduce the number of
injections during the pre-dialysis period.
Background
Anemia is a common complication of chronic kidney disease (CKD) that occurs as a result of
inadequate erythropoietin production by the damaged kidneys. It develops early in the course
of CKD,1 and is associated with the reduced
quality of life,2 the development of
cardiovascular diseases such as left ventricular hypertrophy3 and congestive heart failure,4 as well as the increased mortality5 in pre-dialysis CKD patients. Anemia in CKD is treated by
erythropoiesis-stimulating agents (ESA). Correction of anemia with ESA has been shown to
improve the quality of life and left ventricular hypertrophy,6 and to prolong the kidney survival.7,8
Currently, the guidelines published by the Japanese Society for Dialysis Therapy recommend a
target hemoglobin (Hb) concentration of 11.0 to 13.0 g/dL for pre-dialysis CKD
patients.9
Two long-acting ESA, darbepoetin alfa (DA) and a continuous erythropoietin receptor
activator (CERA, also known as methoxy polyethylene glycol-epoetin beta), have been approved
for the treatment of anemia in patients with CKD. Whereas DA exhibits a half-life of 24–48 h
in peritoneal dialysis patients,10 CERA
has unique pharmacologic properties, acting differently from recombinant human
erythropoietin (epoetin) and DA at the erythropoietin receptor level, with a long half-life
of approximately 130 h.11 These half-life
values are markedly longer than that of 8.5 h of epoetin. Both DA and CERA have been shown
to successfully correct anemia and maintain stable Hb levels within the recommended target
range in non-dialysis CKD patients at extended administration intervals.12,13,14,15 However,
it has not been fully elucidated if they are also effective to prevent the progression of
anemia at initiation of dialysis when Hb levels decrease most severely. Indeed, results of
previous studies showed that the Hb level declined to 8.35 g/dL at initiation of dialysis in
Japanese CKD patients treated with epoetin.16 In the present study, we therefore compared the efficacy of CERA and DA
on anemia in pre-dialysis CKD patients during the 6 months prior to initiation of
hemodialysis.
Methods
Patients
This study was a retrospective study conducted at a single center in Japan. The study
protocol was approved by the Ethics Committee of Keio University. Outpatients who visited
Keio University Hospital for treatment of CKD for more than 6 months prior to initiation
of dialysis, and started hemodialysis therapy between January 1, 2014 and October 31, 2015
were recruited. They were divided into two groups, DA group and CERA group, based on the
use of ESA during the pre-dialysis period. There were no restrictions for their primary
physicians regarding the selection of ESA. Patients who had malignancies, hematological
disorders, or liver cirrhosis, patients who received red blood cell transfusion, patients
who were administrated both DA and CERA during the pre-dialysis period were excluded.
Variables
Baseline characteristics (age, gender, height, body weight, primary cause of CKD, past
history of cardiovascular disorders), clinical data (systolic and diastolic blood
pressure, use of angiotensin converting enzyme inhibitors or angiotensin receptor
blockers, use of iron supplementation, and dates and doses of injection of ESA), and
laboratory data (Hb, mean corpuscular volume, total protein, albumin, urea nitrogen,
creatinine, estimated glomerular filtration rate (eGFR), calcium, inorganic phosphate,
iron, total iron binding capacity, ferritin, transferrin saturation, C-reactive protein,
and cardio-thoracic ratio) were obtained from medical records.
Statistical analysis
Data are reported as percentages or mean ±standard deviation. Categorical data were
compared by means of the chi-square test or Fisher's exact test. Continuous variables were
tested by unpaired t test or one-way factorial ANOVA with a post hoc
Fisher protected least significant difference test. When the data failed to pass the
normality test, Wilcoxon rank sum test or Kruskal-Wallis test with Dunn's post
hoc test was performed. Association between Hb levels and creatinine levels, as
well as association between changes in Hb levels during 1 month before the initiation of
dialysis and creatinine levels, were assessed by Pearson's regression analysis. P values
<0.05 were considered significant.
Results
A total of 90 CKD patients started hemodialysis therapy between January 1, 2014 and October
31, 2015 in our hospital. Out of the 90 patients included in the study, 36 were excluded
from the analysis for one of the following reasons: the patients who visited our hospital
for less than 6 months before starting dialysis, the patients who had malignancies,
hematological disorders or liver cirrhosis, the patients who received red blood cell
transfusion, and the patients who were treated by the combinatorial use of DA and CERA.
Eventually, 40 CKD patients treated with DA and 15 CKD patients treated with CERA over 6
months prior to initiation of hemodialysis were analyzed in the present study.
The characteristics of the patients showed no significant differences in gender, height,
weight, systolic and diastolic blood pressure, primary cause of CKD, past history of
cardiovascular diseases, the use of angiotensin converting enzyme inhibitors or angiotensin
receptor blockers, and iron supplement use between DA and CERA groups, although DA group was
significantly older than CERA group (Table 1).
Laboratory data at initiation of dialysis also showed no significant differences in serum
levels of urea nitrogen, creatinine, total protein, albumin, calcium, inorganic phosphate,
iron, total iron binding capacity, transferrin saturation, ferritin, and C-reactive protein
between these groups (Table 2). Although the
parameters for iron deficiency, such as iron, total iron binding capacity, transferrin
saturation and ferritin, were not different between DA and CERA groups, mean corpuscular
volume was smaller in CERA group than DA group. Reticulocyte levels were unavailable in most
patients. Cardio-thoracic ratio and eGFR did not differ between the two groups.
During the 6-months pre-dialysis period, serum levels of creatinine gradually increased in
both groups (Figs. 1A–1C). Indeed, serum levels of
creatinine 6 months before dialysis were 6.0 ± 1.6 mg/dL in DA group and 5.0 ± 1.7 mg/dL in
CERA group, respectively (Table 3), and they
were not significantly different between the two groups (P = 0.056). At
initiation of hemodialysis, they were 9.9 ± 2.9 mg/dL in DA group and 10.0 ± 3.1 mg/dL in
CERA group, respectively, and also did not differ between the two groups (P
= 0.828). Hb levels were kept constant from 6 months before dialysis to 1 month before
dialysis, although they significantly decreased at initiation of dialysis in both groups
(Figs. 1D–1F). Hb levels at initiation of
dialysis were similar between DA group (9.1 ± 1.2 g/dL) versus CERA group (9.0 ± 1.0 g/dL).
The monthly doses of ESA did not change significantly from 6 months before dialysis to
initiation of dialysis in each group (Figs. 1G
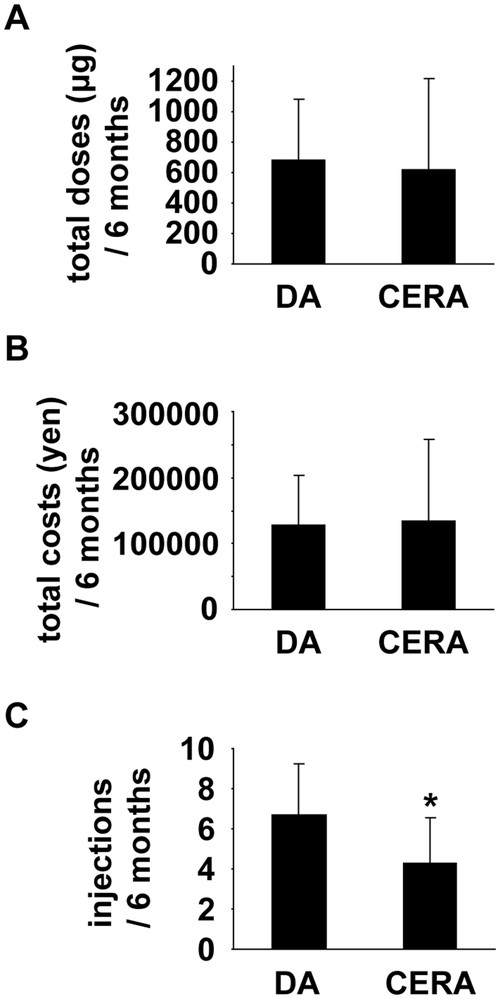
and 1H). In addition, total amounts of ESA, as
well as total costs of ESA, used for 6 months were not different between the two groups
(Figs. 2A and
2B). However, as shown in Fig.
2C, DA group received subcutaneous injections of ESA more frequently (6.6 ±
2.5 times/6 months) than CERA group (4.3 ± 2.3 times/6 months).
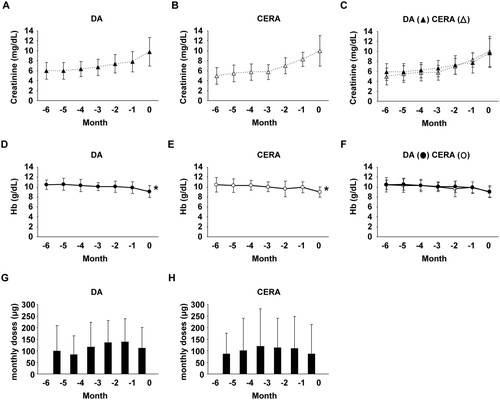
Table 1.
Characteristics of patients at initiation of dialysis
|
DA (n=40) |
CERA (n=15) |
P-value |
| age (years) |
69.4 ± 12.4 |
59.7 ± 14.2 |
0.016 |
| male (%) |
70.0 |
66.6 |
1.000 |
| height (cm) |
161.0 ± 8.6 |
160.4 ± 7.3 |
0.794 |
| body weight (kg) |
58.9 ± 15.4 |
63.4 ± 9.7 |
0.302 |
| systolic blood pressure (mmHg) |
136 ± 22 |
145 ± 21 |
0.172 |
| diastolic blood pressure (mmHg) |
74 ± 15 |
73 ± 14 |
0.738 |
| CKD etiology |
|
|
|
| diabetes (%) |
32.5 |
40.0 |
0.888 |
| hypertension (%) |
27.5 |
26.7 |
1.000 |
| primary glomerular diseases (%) |
25.0 |
20.0 |
1.000 |
| polycystic kidney disease (%) |
5.0 |
0.0 |
1.000 |
| others (%) |
10.0 |
13.3 |
0.660 |
| history of CVD (%) |
17.5 |
26.7 |
0.468 |
| ACEI or ARB use (%) |
30.0 |
46.7 |
0.401 |
| iron supplement use (%) |
22.5 |
26.7 |
0.734 |
CVD: cardiovascular disease; ACEI: angiotensin converting enzyme inhibitors; ARB:
angiotensin receptor blockers
Table 2.
Laboratory data at initiation of dialysis
|
DA (n=40) |
CERA (n=15) |
P-value |
| urea nitrogen (mg/dL) |
99 ± 29 |
83 ± 24 |
0.056 |
| creatinine (mg/dL) |
9.9 ± 2.9 |
10.0 ± 3.1 |
0.828 |
| eGFR (mL/min/1.73 m2) |
4.8 ± 1.8 |
4.9 ± 1.6 |
0.712 |
| total protein (g/dL) |
6.0 ± 0.8 |
5.9 ± 0.7 |
0.615 |
| albumin (g/dL) |
3.2 ± 0.7 |
3.2 ± 0.6 |
0.872 |
| calcium (mg/dL) |
7.9 ± 1.0 |
7.5 ± 1.0 |
0.279 |
| inorganic phosphate (mg/dL) |
6.8 ± 1.8 |
6.3 ± 1.6 |
0.512 |
| iron (μg/dL) |
63.6 ± 42.1 |
60.9 ± 27.5 |
0.736 |
| total iron binding capacity (μg/dL) |
242.1 ± 58.5 |
238.2 ± 48.9 |
0.832 |
| transferrin saturation (%) |
27.2 ± 18.3 |
26.2 ± 12.3 |
0.705 |
| ferritin (ng/mL) |
146.0 ± 103.7 |
190.0 ± 126.1 |
0.305 |
| mean corpuscular volume (fL) |
92.6 ± 3.7 |
87.8 ± 4.4 |
0.003 |
| C-reactive protein (mg/dL) |
1.78 ± 2.57 |
1.21 ± 1.72 |
0.642 |
| cardio-thoracic ratio (%) |
56.4 ± 7.7 |
56.2 ± 7.4 |
0.705 |
Table 3.
Laboratory data at 6 months before initiation of dialysis
|
DA (n=40) |
CERA (n=15) |
P-value |
| urea nitrogen (mg/dL) |
62 ± 18 |
51 ± 20 |
0.060 |
| creatinine (mg/dL) |
6.0 ± 1.6 |
5.0 ± 1.7 |
0.056 |
| albumin (g/dL) |
3.6 ± 0.8 |
3.6 ± 0.7 |
0.873 |
| calcium (mg/dL) |
8.4 ± 0.7 |
8.3 ± 0.7 |
0.621 |
| inorganic phosphate (mg/dL) |
5.2 ± 0.9 |
4.8 ± 0.7 |
0.963 |
| C-reactive protein (mg/dL) |
0.45 ± 0.84 |
0.14 ± 0.22 |
0.191 |
The guidelines published by the Japanese Society for Dialysis Therapy9 recommend the dose reduction or interruption of
ESA therapy if the Hb level exceeds 13 g/dL in pre-dialysis CKD patients (or exceeds 12 g/dL
in pre-dialysis CKD patients with a history of serious cardiovascular disease). We examined
the number of pre-dialysis CKD patients whose Hb level was elevated more than these levels.
One in 40 CKD patients treated with DA and 1 in 15 CKD patients treated with CERA,
respectively, had such an episode of Hb overshoot. The incidence of Hb overshoot was not
significantly different between DA and CERA groups.
Finally, we examined the relationship between Hb levels and serum levels of creatinine at
initiation of dialysis in both groups together. No significant correlation was observed
between these parameters (r =0.074, P = 0.590, n =55). In addition, no
significant correlation was observed between changes in Hb levels during the 1 month before
initiation of dialysis and serum levels of creatinine at initiation of dialysis (r =0.201,
P = 0.297, n =55), suggesting that the decline in Hb levels at initiation
of dialysis is not simply caused by the decline in kidney function.
Discussion
In the present study, we examined the effect of DA and CERA on anemia in pre-dialysis CKD
patients during the 6 months period before initiation of hemodialysis. The results showed
that DA and CERA, respectively, maintained Hb levels around 10 g/dL from 6 months before
dialysis to 1 month before dialysis, but they both failed to prevent a decline in Hb levels
at initiation of dialysis. Hb levels at initiation of dialysis decreased to 9.1 ± 1.2 g/dL
in DA group and 9.0 ± 1.0 g/dL in CERA group, respectively. Results also showed that CKD
patients treated with DA received more subcutaneous injections than those treated with CERA,
although total doses and total costs of ESA used during the 6-months pre-dialysis period
were similar between the two groups. The reduction in the number of subcutaneous injection
is of importance, because administration of ESA is painful and some CKD patients receive
injections with fear. As such, results of the present study suggest that: 1) CKD patients
are required to get more attention to prevent the progression of anemia immediately before
dialysis; and 2) CERA is, possibly, more useful than DA to reduce the number of subcutaneous
injections during the pre-dialysis period.
Results of previous studies showed that hemodialysis patients had a high mortality rate
within 120 days after initiation of hemodialysis,17 and that the incidence of cardiovascular events in the first week after
initiation of hemodialysis was much higher than the subsequent period.18 Because Hb levels decrease most severely at
initiation of dialysis16 and because
anemia is a risk factor for the development of cardiovascular diseases and the increased
mortality,3,4,5 it is highly possible that the prevention of a decline in Hb levels at
initiation of dialysis improves the prognosis in CKD patients. In support of this, results
of recent studies showed that low Hb level at hemodialysis initiation was a significant risk
factor for coronary artery disease and cerebrovascular disease.19 Based on the results described above and those of the present
study, it is suggested that CKD patients need larger doses and/or more frequent injections
of ESA immediately before dialysis, even under the use of long-acting ESA.
The target Hb level for renal anemia is 11–13 g/dL in patients with CKD stage 3–5 according
to the guidelines of the Japanese Society of Dialysis Therapy.9 However, mean Hb levels in both DA and CERA groups did not
achieve the target in the present studies. In spite of the guideline recommendation, monthly
ESA doses were not increased during the observation period. There are several explanations
about this phenomenon. First, ESA are expensive, and patients sometimes refuse to increase
the doses. Second, some patients are unable to visit the hospital frequently for personal
reasons. Third, some nephrologists might consider the negative effect of ESA on the risk of
cardiovascular diseases. Indeed, there are several studies reporting that higher Hb targets
by ESA therapy did not improve the outcome in pre-dialysis CKD patients.20,21,22 These reasons may affect the fact that, even under the treatment with
ESA, mean Hb levels were below 11.0 g/dL during the observation period.
Recently, two groups have independently reported retrospective studies similar to our
present studies.23,24 Results of both studies showed the decline in
Hb levels at initiation of dialysis in CKD patients treated with epoetin, DA, or CERA. Any
one of these ESA failed to maintain target Hb levels at initiation of dialysis, as we have
shown. As compared to our present study, the advantage of these studies is that they
analyzed larger number of CKD patients. On the other hand, the disadvantage of these studies
is that they enrolled CKD patients who started dialysis from 2007 to 2014 in one
study23 and from 2009 to 2015 in
another study.24 During these long
periods, the guideline has been revised,9
and many papers which may affect the decision of the nephrologists regarding the ESA therapy
have been reported. Nonetheless, results of the previous studies and our present study all
suggest that more intense ESA therapy is needed for pre-dialysis CKD patients to avoid the
progression of anemia immediately before initiation of dialysis.
In the present study, the efficacy of DA and CERA was analyzed as equivalent ESA dose.
Indeed, some previous studies used a dose conversion ratio of DA:CERA =1:0.93 for
non-dialysis CKD patients,13 whereas
others used a ratio of 1:1.23,24 Even if
the conversion ratio of 1:0.93 was adapted, the conclusions of the present study were
unaffected.
There are several limitations in the present study. First, the number of CKD patients
treated with DA versus CERA was quite different. Second, the age was also different between
the two groups. These differences may contribute to the efficiency of ESA on anemia
treatment. Moreover, although alcohol consumption and smoking might influence renal anemia,
the history of these habits could not be determined accurately because of the nature of
retrospective studies. Prospective randomized studies are needed in future.
In summary, results of the present study suggest that CKD patients need to be treated with
more intense ESA therapy to prevent the progression of anemia immediately before dialysis,
and that CERA is, possibly, more useful than DA to reduce the number of subcutaneous
injections during the pre-dialysis period. It is of interest to determine the relationship
between Hb level and the prognosis of CKD patients enrolled in the present study in
future.
Acknowledgements
M.H. received grants from Kyowa Hakko Kirin Co., Ltd.. and Chugai Pharmaceutical Co.
However, these corporations were not involved in designing or conducting this study. T.Y.
has no conflicts of interest to declare.
References
- 1. Hsu CY, McCulloch CE, Curhan GC: Epidemiology of
anemia associated with chronic renal insufficiency among adults in the United States:
results from the Third National Health and Nutrition Examination Survey. J Am Soc Nephrol
2002; 13: 504–510.
- 2. Revicki DA, Brown RE, Feeny DH, Henry D, Teehan
BP, Rudnick MR, Benz RL: Health-related quality of life associated with recombinant human
erythropoietin therapy for predialysis chronic renal disease patients. Am J Kidney Dis
1995; 25: 548–554.
- 3. Kuwahara M, Iimori S, Kuyama T, Akita W, Mori Y,
Asai T, Tsukamoto Y, Adachi S, Rai T, Uchida S, Sasaki S: Effect of anemia on cardiac
disorders in pre-dialysis patients immediately before starting hemodialysis. Clin Exp
Nephrol 2011; 15: 121–125.
- 4. Walker AM, Schneider G, Yeaw J, Nordstrom B,
Robbins S, Pettitt D: Anemia as a predictor of cardiovascular events in patients with
elevated serum creatinine. J Am Soc Nephrol 2006; 17: 2293–2298.
- 5. Levin A, Djurdjev O, Duncan J, Rosenbaum D, Werb
R: Haemoglobin at time of referral prior to dialysis predicts survival: an association of
haemoglobin with long-term outcomes. Nephrol Dial Transplant 2006; 21:
370–377.
- 6. Hirakata H, Tsubakihara Y, Gejyo F, Nishi S, Iino
Y, Watanabe Y, Suzuki M, Saito A, Akiba T, Inaguma D, Fukuhara S, Morita S, Hiroe M, Hada
Y, Suzuki M, Akaishi M, Aonuma K, Akizawa T: Maintaining high hemoglobin levels improved
the left ventricular mass index and quality of life scores in pre-dialysis Japanese
chronic kidney disease patients. Clin Exp Nephrol 2010; 14: 28–35.
- 7. Kuriyama S, Tomonari H, Yoshida H, Hashimoto T,
Kawaguchi Y, Sakai O: Reversal of anemia by erythropoietin therapy retards the progression
of chronic renal failure, especially in nondiabetic patients. Nephron 1997; 77:
176–185.
- 8. Jungers P, Choukroun G, Oualim Z, Robino C,
Nguyen AT, Man NK: Beneficial influence of recombinant human erythropoietin therapy on the
rate of progression of chronic renal failure in predialysis patients. Nephrol Dial
Transplant 2001; 16: 307–312.
- 9. Tsubakihara Y, Nishi S, Akiba T, Hirakata H,
Iseki K, Kubota M, Kuriyama S, Komatsu Y, Suzuki M, Nakai S, Hattori M, Babazono T,
Hiramatsu M, Yamamoto H, Bessho M, Akizawa T: 2008 Japanese Society for Dialysis Therapy:
guidelines for renal anemia in chronic kidney disease. Ther Apher Dial 2010; 14:
240–275.
- 10. Macdougall IC, Gray SJ, Elston O, Breen C,
Jenkins B, Browne J, Egrie J: Pharmacokinetics of novel erythropoiesis stimulating protein
compared with epoetin alfa in dialysis patients. J Am Soc Nephrol 1999; 10:
2392–2395.
- 11. Macdougall IC, Robson R, Opatrna S, Liogier X,
Pannier A, Jordan P, Dougherty FC, Reigner B: Pharmacokinetics and pharmacodynamics of
intravenous and subcutaneous continuous erythropoietin receptor activator (C.E.R.A.) in
patients with chronic kidney disease. Clin J Am Soc Nephrol 2006; 1:
1211–1215.
- 12. Macdougall IC, Walker R, Provenzano R, de Alvaro
F, Locay HR, Nader PC, Locatelli F, Dougherty FC, Beyer U, ARCTOS Study Investigators:
C.E.R.A. corrects anemia in patients with chronic kidney disease not on dialysis: results
of a randomized clinical trial. Clin J Am Soc Nephrol 2008; 3: 337–347.
- 13. Minutolo R, Zamboli P, Chiodini P, Mascia S,
Vitiello S, Stanzione G, Bertino V, Conte G, De Nicola L: Conversion of darbepoetin to low
doses of CERA maintains hemoglobin levels in non-dialysis chronic kidney disease patients.
Blood Purif 2010; 30: 186–194.
- 14. Roger SD, Locatelli F, Woitas RP, Laville M, Tobe
SW, Provenzano R, Golper TA, Ruangkanchanasetr P, Lee HY, Wu KD, Nowicki M, Ladanyi A,
Martínez-Castelao A, Beyer U, Dougherty FC: C.E.R.A. once every 4 weeks corrects anaemia
and maintains haemoglobin in patients with chronic kidney disease not on dialysis. Nephrol
Dial Transplant 2011; 26: 3980–3986.
- 15. Frimat L, Mariat C, Landais P, Koné S, Commenges
B, Choukroun G: Anaemia management with C.E.R.A. in routine clinical practice: OCEANE
(Cohorte Mircera patients non-dialyses), a national, multicenter, longitudinal,
observational prospective study, in patients with chronic kidney disease not on dialysis.
BMJ Open 2013; 3: e001888.
- 16. Akizawa T, Saito A, Gejyo F, Suzuki M, Nishizawa
Y, Tomino Y, Tsubakihara Y, Akiba T, Hirakata H, Watanabe Y, Kawanishi H, Bessho M,
Udagawa Y, Aoki K, Uemura Y, Ohashi Y, Co-JET Study Group: Impacts of recombinant human
erythropoietin treatment during predialysis periods on the progression of chronic kidney
disease in a large-scale cohort study (Co-JET study). Ther Apher Dial 2014; 18:
140–148.
- 17. Robinson BM, Zhang J, Morgenstern H, Bradbury BD,
Ng LJ, McCullough KP, Gillespie BW, Hakim R, Rayner H, Fort J, Akizawa T, Tentori F,
Pisoni RL: Worldwide, mortality risk is high soon after initiation of hemodialysis. Kidney
Int 2014; 85: 158–165.
- 18. Eckardt KU, Gillespie IA, Kronenberg F, Richards
S, Stenvinkel P, Anker SD, Wheeler DC, de Francisco AL, Marcelli D, Froissart M, Floege J,
ARO Steering Committee: High cardiovascular event rates occur within the first weeks of
starting hemodialysis. Kidney Int 2015; 88: 1117–1125.
- 19. Kataoka H, Tsuchiya K, Naganuma T, Okazaki M,
Komatsu M, Kimura T, Shiohira S, Kawaguchi H, Nitta K: Relationship between anaemia
management at haemodialysis initiation and patient prognosis. Nephrology (Carlton) 2015;
20(Suppl 4): 14–21.
- 20. Drüeke TB, Locatelli F, Clyne N, Eckardt KU,
Macdougall IC, Tsakiris D, Burger HU, Scherhag A, CREATE Investigators: Normalization of
hemoglobin level in patients with chronic kidney disease and anemia. N Engl J Med 2006;
355: 2071–2084.
- 21. Singh AK, Szczech L, Tang KL, Barnhart H, Sapp S,
Wolfson M, Reddan D, CHOIR Investigators: Correction of anemia with epoetin alfa in
chronic kidney disease. N Engl J Med 2006; 355: 2085–2098.
- 22. Pfeffer MA, Burdmann EA, Chen CY, Cooper ME, de
Zeeuw D, Eckardt KU, Feyzi JM, Ivanovich P, Kewalramani R, Levey AS, Lewis EF, McGill JB,
McMurray JJ, Parfrey P, Parving HH, Remuzzi G, Singh AK, Solomon SD, Toto R, TREAT
Investigators: A trial of darbepoetin alfa in type 2 diabetes and chronic kidney disease.
N Engl J Med 2009; 361: 2019–2032.
- 23. Koibuchi K, Miyagi M, Arai T, Aoki T, Aikawa A,
Sakai K: Comparing the efficacy of continuous erythropoietin receptor activator and
darbepoetin Alfa treatments in Japanese patients with chronic kidney disease during the
predialysis period: A propensity-matched analysis. Nephrology (Carlton) 2015; 20(Suppl 4):
22–28.
- 24. Kawahara K, Minakuchi J, Yokota N, Suekane H,
Tsuchida K, Kawashima S: Treatment of renal anaemia with erythropoiesis-stimulating agents
in predialysis chronic kidney disease patients: Haemoglobin profile during the 6 months
before initiation of dialysis. Nephrology (Carlton) 2015; 20(Suppl 4):
29–32.