Abstract
Introduction of the robotic stapler has allowed robotic lobectomy to be performed from a
surgical console in complete autonomy. The robotic stapler fits a 12-mm port, which is
larger than the standard 8-mm port and increases the risk of postoperative pain. However,
in many cases, to cover all possible angles of approach, two 12-mm ports are preferably
used. However, limiting instrument inventory and simplifying surgical procedures are also
desirable to reduce costs. In a multicenter study, we assessed the feasibility of robotic
lobectomy with a single type of robotic stapler [SureForm45 Curved-Tip (SF45C); Intuitive
Surgical Inc.] inserted through one 12-mm port placed at the anterior tip of the lower
intercostal space. We also investigated the potential cost savings of using an additional
60-mm stapler for interlobar division. A total of 135 lobectomy cases were enrolled. In
all cases, all stapling procedures were completed using the SF45C inserted from the
designated 12-mm port. We found that it was potentially less expensive to use the
SureForm60 stapler if more than six SF45C reloads were needed for interlobar division.
However, in our series, only 1 case (0.7%) met this requirement. The use of a single type
of stapler from one 12-mm port in a robotic lobectomy is technically feasible. This
approach may be expected to allow for surgical simplification, minimize the risk of
postoperative pain, and reduce inventory costs.
Introduction
The da Vinci surgical system (Intuitive Surgical Inc., Sunnyvale, CA, USA) has several
advantages when compared with conventional thoracoscopic surgical systems, including
three-dimensional imaging, a stable camera and operating platform, articulating instruments
with seven degrees of freedom, excellent ergonomics, motion scaling, and tremor-free
movements.1 However, although stapler
division of the hilar pulmonary structures is the most important and potentially dangerous
step of the operation, a robotic stapler has not been available for use with the
conventional da Vinci Si system. Instead, this task has been delegated to and performed by
the bedside assistant.2,3
The introduction of the first robotic stapler [EndoWrist (EW); Intuitive Surgical Inc.] in
the da Vinci Xi system made it possible for a Robot-assisted Thoracic Surgery (RATS)
lobectomy to be controlled directly by the operating surgeon, who can divide the hilar
structures from the robotic console. This development has facilitated the introduction of
robotic surgery in the field of general thoracic surgery.2,3
At present, stapling strategies play a significant role in choosing where to place trocars
with the da Vinci Xi system. The robotic stapler is a large device and placing the stapling
ports as low as possible (i.e., close to the diaphragm) is thought to be advantageous and to
allow the greatest degree of maneuverability in the chest cavity. To cover all possible
angles, most surgeons place one stapling trocar anteriorly and another posteriorly. Surgeons
should also consider that the robotic stapler requires a large 12-mm port even though
standard robotic instruments fit through 8-mm ports. Large 12-mm port placement increases
the risk of postoperative pain, especially in the narrow posterior intercostal
space.4
Despite its utility, the cost of robotic surgery is high. Obviously, there are many
stapling options, including the use of both a robotic stapler and a hand-held endoscopic
linear stapler (ELS) by a bedside assistant. Limiting the range of instruments, including
staplers, and simplification of the surgical procedure are required to reduce the inventory
cost and operating times for the sustainable development of robotic surgery.5
The newest robotic stapler [SureForm (SF); Intuitive Surgical Inc.] has a 120-degree cone
of articulation, which is much wider than the conventional EW robotic stapler, the
articulation of which is elliptical (i.e., 108 degrees left to right and 54 degrees up and
down). This improvement may allow surgeons to complete the entire stapling procedure with a
single 12-mm stapler port placed in an anterior intercostal space. In addition, given that
anterior intercostal spaces are larger than posterior intercostal spaces, this approach may
reduce the risk of postoperative pain. Based on the issues described above, we assessed the
feasibility of using a single type of stapler (SureForm45 Curved-Tip, SF45C) inserted
through one 12-mm port to perform robotic lobectomy in a multicenter setting.
Ethics and consent
All study procedures were conducted in accordance with the Declaration of Helsinki and its
later amendments. This study was approved by the Ethics Review Committee of the Saiseikai
Yokohama-shi Tobu Hospital (referral number 20210215), Southern Tohoku General Hospital
(referral number 544), Showa University (referral number 2023–193-B), and Shin-Yurigaoka
General Hospital (referral number 20230828–2).
Given the retrospective nature of the study, the opt-out approach was used to provide
consent. Only anonymized data were included in the customized database.
Institution
Four institutions participated in this study: Saiseikai Yokohama-shi Tobu Hospital,
Southern Tohoku General Hospital, Showa University, and Shin-Yurigaoka General Hospital.
Robotic lobectomies performed at participating institutions between April 2020 and
February 2022 were included and operation data were retrospectively collected and studied.
Case selection for robotic lobectomy was left to the individual institutions. During this
period, all the participating institutions had introduced robotic lobectomy under the
supervision of the corresponding author (M.O.). Each institution used the same port,
instruments, and stapler strategy as described below.
Port placement
We utilized the RPL-4 approach (robotic portal lobectomy with four arms) with carbon
dioxide insufflation using the da Vinci Xi surgical system (Fig. 1).6 Patients
were placed in a lateral decubitus position and were managed with general anesthesia and
double lumen intubation. Three 8-mm ports were placed in the same intercostal space. More
specifically, they were placed in the sixth intercostal space for upper lobectomies and in
the seventh intercostal space for middle and lower lobectomies. A 12-mm stapling port was
placed as far anteriorly as possible, usually one interspace below the other three ports.
In this study, in principle, all the stapling procedures were performed from this 12-mm
port using the SF45C with a white up to a black reload. A 12-mm AirSeal (ConMed, Utica,
NY, USA) assist port was inserted in the anterior tenth intercostal space.
Data collection
Lobectomy data were collected using a questionnaire. The questionnaires were sent to the
coauthors at each institution. The completed questionnaires were then returned to the lead
author (Y.I.) by E-mail.
The complete survey included the following information for each lobectomy:
-
2. Number of staplers used (excluding staplers used for intraoperative frozen section
diagnosis),
-
3. Number and type of staplers used for division of the pulmonary vessels, bronchus,
and fissure,
-
4. If a stapler other than the designated SF45C was used and why, and
-
5. Whether a stapler was used from a port other than the designated anterior 12-mm
port and if so, where and why.
Investigation of potential cost saving by using additional 60-mm
stapler
The thoracic cavity is much narrower than the abdominal cavity. Therefore, from the
standpoint of maneuverability and safety, the use of a 45-mm stapler, rather than a 60-mm
stapler, is appropriate for division of the hilar structure. However, there is a potential
cost advantage to the added use of a 60-mm stapler for obliterated interlobar division
instead of using a 45-mm stapler alone. Therefore, we estimated and compared the cost of
completing the entire procedure using the SF45C alone and adding the SF60 for interlobar
fissure division. The potential advantages of using the SF60 in clinical practice were
considered.
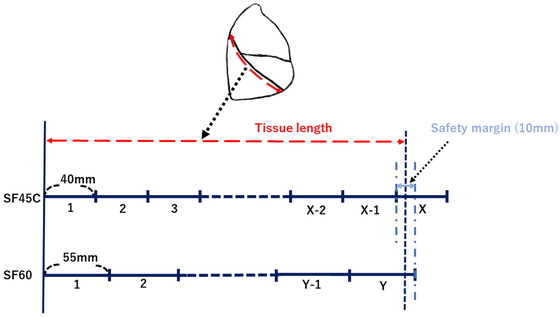
The potential cost savings from the added use of the SF60 were assessed as follows: if
X and Y represent the respective numbers of SF45C and
SF60 stapler reloads required for interlobar division, and the catalog cutline lengths of
SF45C and SF60 are 40 mm and 55 mm, respectively, when X reloads of the
SF45C are required to cut the interlobar tissue, X−1 reloads of the SF45C
are insufficient to cut the tissue. This condition can be expressed in the
inequality:
40×(X−1) < Tissue
length
When the tissue can be cut with Y reloads of the SF60, the following
inequality holds:
Tissue length < 55 ×
Y
Therefore, the condition for tissue length
is:
40 × (X−1) < Tissue
length < 55 × Y
If the difference between 40 × (X−1) and 55 × Y is too
small, this inequality will almost never be satisfied, making it impractical.
Therefore, assuming that the difference in staple length (safety margin) between
X−1 reloads of the SF45C and Y reloads of the SF60 is
at least 10 mm (Fig. 2), the relationship
between X and Y
is:
40 × (X−1) < 55 × Y+10
(1)
The SF45C and SF60 stapler shafts each cost 35,000 yen (US 233.30 at an exchange
rate of 150 yen to the dollar). Stapler reloads cost 31,000 yen for SF45C and 34,000 yen
for SF60 (206.70 and 226.70, respectively).
If using SF45C and SF60 together is cheaper than using SF45C alone, the following
inequality holds:
31,000 × X > 35,000 +
34,000 × Y
(2)
We investigated the potential cost saving by the use of an additional 60-mm stapler by
identifying the proportion of cases that may satisfy these simultaneous inequalities.
Exclusion criteria
The following cases were excluded from this study: those in which surgery was performed
by other robotic port approaches; cases in which staplers other than the SF45C were used
for non-technical reasons; and cases that required conversion to another approach [i.e.,
conventional video-assisted thoracic surgery (VATS) and/or open thoracotomy].
Results
Of the 163 cases collected, 28 were excluded because staplers other than SF45C were used
for non-technical reasons (out of stock or because of inventory clearance). All stapling
procedures in these 28 cases were completed by using a robotic stapler inserted through the
designated anterior inferior 12-mm port. A hand-held ELS was not used.
No operations were performed by other robotic port approaches. No cases were converted to
VATS or open thoracotomy. Consequently, a total of 135 cases of robotic lobectomy were
enrolled (Shin-Yurigaoka General Hospital, 35; Saiseikai Yokohama-shi Tobu Hospital, 45;
Southern Tohoku General Hospital, 37; Showa University Hospital, 18).
All stapling procedures were completed using the SF45C inserted through the designated
anterior inferior 12-mm port. The 135 surgical procedures included 44 right upper
lobectomies, 18 right middle lobectomies, 33 right lower lobectomies, 20 left upper
lobectomies, and 20 left lower lobectomies. The numbers of reloads required for each
surgical step (vessel division, bronchial division, and interlobar division) and for the
overall operation according to type of lobectomy are listed in Table 1.
Table 1.Number of reloads used per case for each surgical step according to lobectomy
type
| Lobectomy type |
Hilar vessel division |
Bronchial division |
Interlobar division |
Overall procedure |
| Right upper (n=44) |
3 [1–5] |
1 [1–2] |
3 [0–6] |
7 [4–11] |
| Right middle (n=18) |
2.5 [1–5] |
1 [1] |
3 [1–5] |
6.5 [4–10] |
| Right lower (n=33) |
2 [1–4] |
1 [1] |
2 [0–5] |
5.5 [3–9] |
| Left upper (n=20) |
4 [2–6] |
1 [1–2] |
1.5 [0–5] |
7 [4–11] |
| Left lower (n=20) |
3 [2–4] |
1 [1] |
2 [0–5] |
6 [3–9] |
| Overall (n=135) |
3 [1–6] |
1 [1–2] |
2 [0–6] |
6 [3–11] |
Data are shown as median [range].
For hilar vessel division, the number of stapler reloads (median [range]) required per case
was 3 [1–5] during right upper lobectomy, 2.5 [1–5] during right middle lobectomy, 2 [1–4]
during right lower lobectomy, 4 [2–6] during left upper lobectomy, and 3 [2–4] during left
lower lobectomy. Considering all lobectomies, 3 [1–6] stapler reloads were required for
hilar vessel division.
For bronchial division, 1 [1–2] stapler reload was required during right upper lobectomy or
left upper lobectomy and 1 [1] was required during right middle lobectomy, right lower
lobectomy, or left lower lobectomy. Considering all lobectomies, 1 [1–2] stapler reload was
required for bronchial division.
For interlobar division, 3 [0–6] stapler reloads were required during right upper
lobectomy, 3 [1–5] during right middle lobectomy, 2 [0–5] during right lower lobectomy or
left lower lobectomy, and 1.5 [0–5] during left upper lobectomy. Considering all
lobectomies, 2 [0–6] stapler reloads were required for interlobar division.
Based on all procedures, 7 [4–11] stapler reloads were required during right or left upper
lobectomy, 6.5 [4–10] during right middle lobectomy, 5.5 [3–9] during right lower lobectomy,
and 6 [3–9] during left lower lobectomy. Overall, 6 [3–11] stapler reloads were required
during all lobectomies.
In examining the potential cost savings of using an additional 60-mm stapler, Figure 3 shows the range for which the simultaneous
inequalities (1) and (2) are valid. If the SF45C requires more than six reloads to divide
the interlobular fissure, it may be more economical to switch to the SF60. In our series,
only one case (0.7%) met this requirement. This particular case was a right upper lobectomy
that required six stapler reloads for interlobar division. However, replacing the SF45C with
the SF60 in such situations would reduce costs by only 15,000 yen per case ($100).
Discussion
The development of the first robotic stapler, which was only available on the da Vinci Xi
robotic system, was a major technological leap and facilitated the introduction of
robot-assisted technology in thoracic surgery.2 Before the development of the robotic stapler, inexperienced assistants
who had to staple vessels using a hand-held ELS were a potential risk factor for
intraoperative catastrophic bleeding during major lung resection.2 Therefore, many thoracic surgeons were reluctant to adopt robots
in clinical practice. However, the introduction of the robotic stapler made it possible to
perform a complete robotic lung resection without entrusting hilar structure division to
inexperienced assistants.
Robotic staplers fit 12-mm robotic ports and are larger than standard robotic instruments
that fit 8-mm ports; therefore, their use may increase the risk of postoperative pain.
Nevertheless, many surgeons prefer to place two 12-mm ports (one anterior and one posterior)
to accommodate virtually all stapler angles for the division of any structure.4 This trend may be partly attributed to the fact
that the traditional robotic stapler (EW) is not sophisticated in terms of operability. In
comparison, the latest robotic stapler (SF) has a wider range of motion and improved
operability. Therefore, the use of two 12-mm ports might not always be necessary.5 However, among the many stapler options,
including use of the hand-held ELS, inventory management could be simplified by exclusive
use of the SF45C, which has superior maneuverability. These issues motivated us to
investigate the feasibility of using a single type of stapler (SF45C) from a single 12-mm
port for robotic lobectomy. The following results were obtained:
-
1. In all lobectomies, it was possible to complete the divisions of all hilar vascular
and bronchial structures, and interlobar fissures, using the robotic stapler (SF45C)
inserted from the designated single anterior inferior 12-mm stapler port.
-
2. Adding a 60-mm stapler (SF60) for interlobar division, especially in cases with
fused fissures, might be more cost effective than a 45-mm stapler (SF45C) alone. We also
found that it was less expensive to use the SF60 if more than six SF45C reloads were
needed for interlobar division. Nevertheless, in our series, only 1 of the 135 cases
(0.7%) met this requirement. The expected cost reduction was 15,000 yen ($100), which is
not large considering the advantages of the simplified surgical procedure and
inventory.
In conclusion, using a single type of stapler (SF45C) inserted through a single 12-mm port
is a technically feasible means of performing robotic lobectomies, and it is more cost
effective than added use of the SF60 for interlobar fissure in most cases. This approach may
be expected to provide surgical simplification, minimize the risk of postoperative pain, and
reduce inventory costs.
This study had some limitations. It was a retrospective single-arm study, and only an
initial small number of cases were enrolled after the introduction of robotic surgery. Case
selection was delegated to each institution. Consequently, cases with a complete fissure and
were technically easy tended to be selected. However, an additional 60-mm stapler (SF60) may
be less expensive in cases of a largely fused fissure, which would seldom have been selected
in our series. Further research will be needed to determine the appropriate use of the
SF60.
In terms of postoperative pain, we assume that our single 12-mm port strategy is superior
to a multiple 12-mm port strategy. However, there is no evidence as to whether the number or
location of intercostal 12-mm ports is related to postoperative pain. A detailed comparative
study using a large sample size will be needed to determine whether postoperative pain is
related to the number and location of intercostal ports.
Conflicts of Interest
Makoto Oda has delivered lectures on behalf of Intuitive Surgical Inc. (Sunnyvale, CA,
USA). The remaining authors declare no conflict of interest.
References
- 1. Veronesi G, Cerfolio R, Cingolani R, Rueckert JC,
Soler L, Toker A, Cariboni U, Bottoni E, Fumagalli U, Melfi F, Milli C, Novellis P, Voulaz
E, Alloisio M: Report on first international workshop on robotic surgery in thoracic
oncology. Front Oncol 2016; 24: 214. https://doi.org/10.3389/fonc.2016.00214. PMID:
27822454; PMCID: PMC5075745.
- 2. Pearlstein DP: Robotic lobectomy utilizing the
robotic stapler. Ann Thorac Surg 2016; 102: e591–e593. PMID:27847093
https://doi.org/10.1016/j.athoracsur.2016.05.105
- 3.Galetta D, Casiraghi M, Pardolesi A, Borri A,
Spaggiari L. New stapling devices in robotic surgery. J Vis Surg 2017; 10 : 45.
https://doi.org/10.21037/jovs.2017.02.03. PMID: 29078608; PMCID:
PMC5637468.
- 4. Oh DS, Tisol WB, Cesnik L, Crosby A, Cerfolio RJ:
Port strategies for robot-assisted lobectomy by high-volume thoracic surgeons: a
nationwide survey. Innovations (Phila) 2019; 14: 545–552. PMID:31739719
https://doi.org/10.1177/1556984519883643
- 5. Zervos M, Song A, Li Y, Lee SH, Oh DS: Clinical
and economic outcomes of using robotic versus hand-held staplers during robotic lobectomy.
Innovations (Phila) 2021; 16: 470–476. PMID:34488486
https://doi.org/10.1177/15569845211040814
- 6. Cerfolio R, Louie BE, Farivar AS, Onaitis M, Park
BJ: Consensus statement on definitions and nomenclature for robotic thoracic surgery. J
Thorac Cardiovasc Surg 2017; 154: 1065–1069. PMID:28623099
https://doi.org/10.1016/j.jtcvs.2017.02.081