Abstract
Several studies have reported the coexistence of chronic subdural hematoma (CSDH) and dural arteriovenous fistula (DAVF); however, the association between these two entities remains unknown. A case of coexisting CSDH and DAVF that was successfully treated with burr hole surgery and middle meningeal artery (MMA) embolization is reported herein. We visualized the positional relationship between CSDH and DAVF by fusion three-dimensional computer graphics images reconstructed from multimodal imaging studies, which revealed that the shunt point of the DAVF was far from the burr hole and was in contact with the CSDH membrane at the center of the CSDH. Additionally, the chronological development of CSDH in the presence of DAVF and the complete disappearance of both DAVF and CSDH after MMA embolization were also demonstrated. This study suggests a possible association between recurrent CSDH and DAVF.
Introduction
Chronic subdural hematoma (CSDH) is a common disease in neurosurgical practice and is characterized by the collection of blood products in the subdural space, along with the formation of membranes with abnormal neovessels.1,2) Meanwhile, dural arteriovenous fistula (DAVF) is a vascular entity that consists of direct pathologic connections between meningeal arteries and dural venous sinuses or leptomeningeal veins.3-5) Several studies have presented cases of coexisting CSDH and DAVF. However, the association between both entities remains unclear. Herein, we report a case of coexisting CSDH and DAVF. The imaging findings and clinical course indicate that the DAVF contributed to the formation of CSDH, and this study provides insights into the pathogenesis and treatment of both CSDH and DAVF.
Case Report
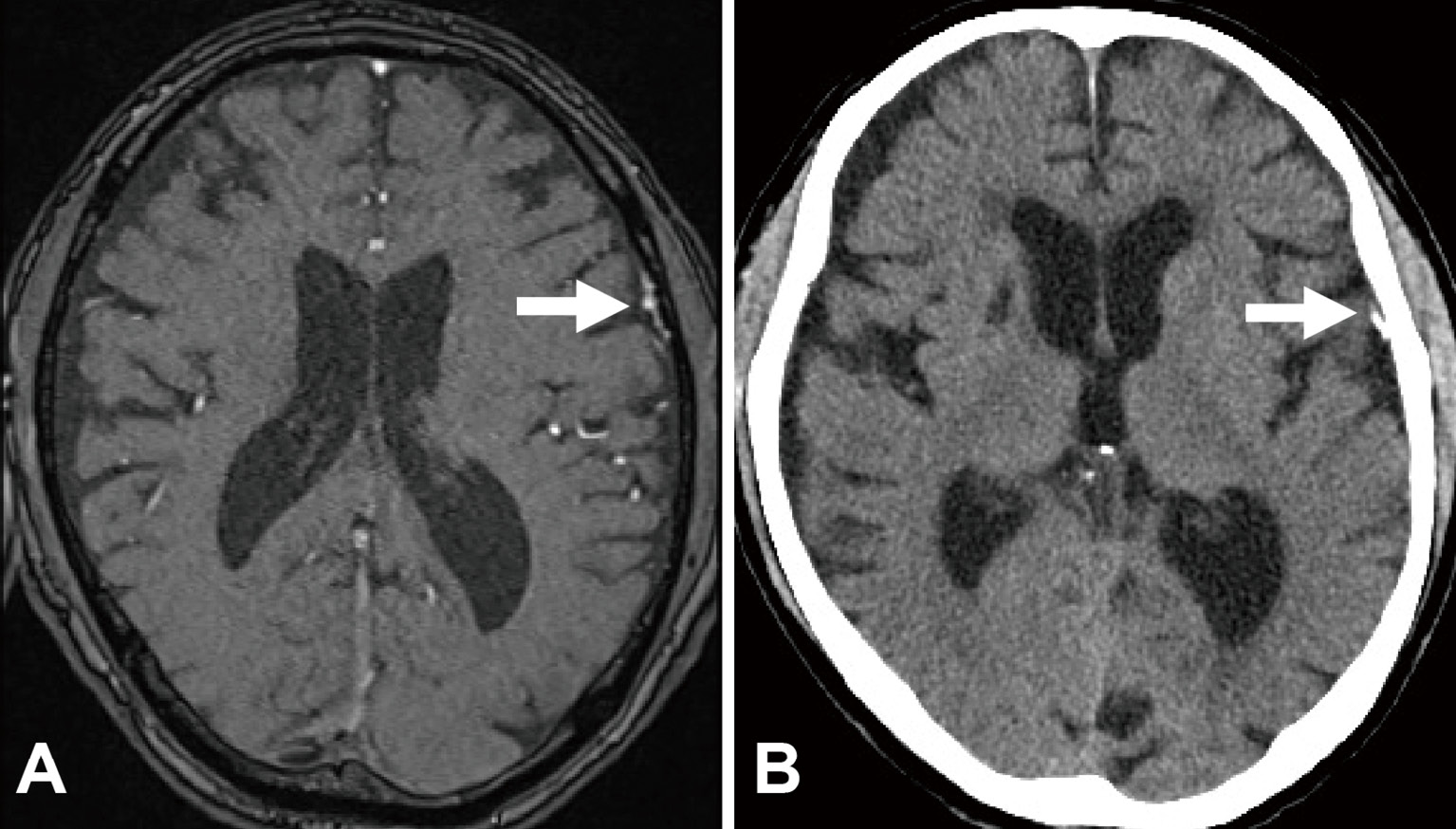
An 81-year-old man without a specific history of head trauma was incidentally diagnosed with asymptomatic left CSDH (Fig. 1A) and conservatively observed. However, his CSDH increased in size with mild right hemiparesis one month later, and he underwent burr hole irrigation and drainage for the left CSDH (Fig. 1B). He was discharged without any neurological deficit; however, deep vein thrombosis (DVT) of the lower extremity was detected based on a high D-dimer level during admission for CSDH. Anticoagulant therapy was recommended to prevent pulmonary thromboembolism, but it was postponed due to the risk of CSDH recurrence. However, he experienced mild right hemiparesis again one month after the initial surgery, and computed tomography (CT) revealed recurrence of the left CSDH (Fig. 1C). The patient underwent second burr hole irrigation and drainage procedure (Fig. 1D). Considering the need for systemic anticoagulation for DVT, we scheduled left middle meningeal artery (MMA) embolization the next day to prevent CSDH recurrence.

During MMA embolization, cerebral angiography revealed a left convexity DAVF immediately beside the CSDH cavity. The feeders of the DAVF were the anterior convexity branches of the MMA, and the drainers were the sylvian veins (Fig. 2A). The DAVF was diagnosed as Borden type III and Cognard type III. Furthermore, cerebral angiography revealed faint staining at the shunt point of the DAVF (Fig. 2B). Considering the possibility that the DAVF could increase meningeal blood flow and could therefore cause CSDH recurrence after burr hole surgery, the DAVF was selectively embolized with N-butyl-2-cyanoacrylate. The shunt point of the DAVF was adequately occluded (Fig. 2C, D). The patient's past magnetic resonance imaging findings after embolization was retrospectively reviewed, and DAVF was confirmed in the image obtained five years before the appearance of CSDH (Fig. 3A).

Systemic anticoagulation with apixaban for DVT was initiated on postoperative day 1. The patient recovered well and was discharged without complications. A follow-up CT examination at five months post-embolization showed complete disappearance of both the DAVF and CSDH, and the patient remained symptom-free (Fig. 3B). To intricately investigate the spatial relationship between the DAVF and CSDH, fusion three-dimensional computer graphics (3DCG) images were reconstructed using GRID 1.1 software (Kompath Inc., Tokyo, Japan). This application provides automatic image registration for multiple imaging studies using normalized mutual information.6) The 3DCG examinations revealed that the shunt point of the DAVF was far from the burr hole (Fig. 4A); moreover, it was in contact with the outer membrane of CSDH (Fig. 4B). The DAVF was almost at the center of the CSDH; however, there was no hematoma at the shunt point.
Discussion
A case of coexisting CSDH and DAVF successfully treated with MMA embolization after burr hole surgery and providing unique imaging findings was reported. The cause and significance of these unique imaging findings are discussed with respect to the clinical course. Through analysis of the fusion 3DCG images, we infer the putative association between CSDH and DAVF.
The CSDH pathogenesis is based on the formation of membranes with abnormal vessel networks promotes a positive feedback cycle of continued hemorrhage, inflammation, and angiogenesis, which results in subdural collection of blood.7,8) The pathogenesis of DAVF remains unclear, but it has been suspected to involve progressive dural venous sinus stenosis or thrombosis with secondary angiogenesis.9) The pathogenesis of both entities involves angiogenesis, but the association between CSDH and DAVF remains uncertain. Several cases of coexisting CSDH and DAVF have been reported, and these have been described as idiopathic or iatrogenic secondary to burr hole surgery.10-15) Tabibian et al. reported that a DAVF was found incidentally in 3 of 30 cases of MMA embolization for CSDH.15) Currently, no study has indicated that a DAVF can contribute to the formation of CSDH.
The mechanism of CSDH enlargement is considered to be repeated bleeding from abnormal vessels in the outer membrane of CSDH. MMA embolization for CSDH could prevent the enlargement and recurrence of CSDH by decreasing the blood supply to abnormal vessels in the CSDH membrane.16,17) Sam et al. reported that MMA embolization also leads to a reduction in the hematoma volume of residual CSDH after burr hole surgery.18) Additionally, the faint staining of abnormal vessels (called cotton wool-like staining) is observed along the CSDH membrane on selective MMA angiography.19-22)
Notably, cerebral angiography and fusion 3DCG in our case revealed that the shunt point of the DAVF was in contact with the outer membrane of CSDH without cotton wool-like staining along the CSDH membrane. Therefore, DAVF may provide abundant feeding to the CSDH membrane. These unique imaging findings suggest that DAVF may be associated with the formation of CSDH. Theoretically, embolization of this abnormal vessel network in the CSDH membrane, including the DAVF, could prevent the enlargement or recurrence of CSDH. Moreover, the CSDH disappeared completely after MMA embolization despite induction of anticoagulant therapy, which was a risk factor for the recurrence of CSDH.23,24) These findings and the clinical course indicated that MMA embolization for DAVF was also potentially effective for CSDH in this case.
In our case, the detailed architecture of DAVF that was in contact with the outer membrane of CSDH could be clearly visualized using fusion 3DCG, which indicated that DAVF may contribute to the recurrence of CSDH. Vascular malformations should be considered in patients with refractory CSDH. Nevertheless, our study was limited by the lack of case series data. Further research is needed to elucidate the association between DAVF and CSDH.
In conclusion, we encountered a case of coexisting CSDH and DAVF, which presented unique imaging findings and clinical course. This case implies that increased meningeal blood flow due to DAVF can contribute to CSDH development and that DAVF embolization may be effective in preventing CSDH recurrence.
Abbreviations
3DCG image, three-dimensional computer graphics image; CSDH, chronic subdural hematoma; CT, computed tomography; DAVF, dural arteriovenous fistula; DVT, deep vein thrombosis; MMA, middle meningeal artery
Author Contributions
SK certifies that all authors have participated and have been involved in the case presented and/or in the elaboration of the present manuscript. All authors contributed to the article and approved the submitted version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflicts of Interest Disclosure
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
- 1) Feghali J, Yang W, Huang J: Updates in chronic subdural hematoma: epidemiology, etiology, pathogenesis, treatment, and outcome. World Neurosurg 141: 339-345, 2020
- 2) Welling LC, Welling MS, Teixeira MJ, Figueiredo EG: Chronic subdural hematoma: so common and so neglected. World Neurosurg 111: 393-394, 2018
- 3) Newton TH, Cronqvist S: Involvement of dural arteries in intracranial arteriovenous malformations. Radiology 93: 1071-1078, 1969
- 4) Kwon BJ, Han MH, Kang HS, Chang KH: MR imaging findings of intracranial dural arteriovenous fistulas: relations with venous drainage patterns. AJNR Am J Neuroradiol 26: 2500-2507, 2005
- 5) Gandhi D, Chen J, Pearl M, Huang J, Gemmete JJ, Kathuria S: Intracranial dural arteriovenous fistulas: classification, imaging findings, and treatment. AJNR Am J Neuroradiol 33: 1007-1013, 2012
- 6) Yoshino M, Kin T, Hara T: Usefulness of high-resolution three-dimensional multifusion medical imaging for preoperative planning in patients with cerebral arteriovenous malformation. World Neurosurg 124: e755-763, 2019
- 7) Ito H, Yamamoto S, Komai T, Mizukoshi H: Role of local hyperfibrinolysis in the etiology of chronic subdural hematoma. J Neurosurg 45: 26-31, 1976
- 8) Edlmann E, Giorgi-Coll S, Whitfield PC, Carpenter KLH, Hutchinson PJ: Pathophysiology of chronic subdural haematoma: inflammation, angiogenesis and implications for pharmacotherapy. J Neuroinflammation 14: 108, 2017
- 9) Reynolds MR, Lanzino G, Zipfel GJ: Intracranial dural arteriovenous fistulae. Stroke 48: 1424-1431, 2017
- 10) Pappas CT, Zabramski JM, Shetter AG: Iatrogenic arteriovenous fistula presenting as a recurrent subdural hematoma. Case report. J Neurosurg 76: 134-136, 1992
- 11) Komiyama M, Yasui T, Tamura K, Nagata Y, Fu Y, Yagura H: Chronic subdural hematoma associated with middle meningeal arteriovenous fistula treated by a combination of embolization and burr hole drainage. Surg Neurol 42: 316-319, 1994
- 12) Kim E: Refractory spontaneous chronic subdural hematoma: a rare presentation of an intracranial arteriovenous fistula. J Cerebrovasc Endovasc Neurosurg 18: 373-378, 2016
- 13) Mewada T, Ohshima T, Yamamoto T, Goto S, Kato Y: Usefulness of embolization for iatrogenic dural arteriovenous fistula associated with recurrent chronic subdural hematoma: a case report and literature review. World Neurosurg 92: 584.e7-584.e10, 2016
- 14) Li G, Zhang Y, Zhao J, Zhu X, Yu J, Hou K: Isolated subdural hematoma secondary to dural arteriovenous fistula: a case report and literature review. BMC Neurol 19: 43, 2019
- 15) Tabibian BE, Liptrap E, Jones J: Incidentally discovered dural arteriovenous fistula during middle meningeal artery embolization for the treatment of chronic subdural hematoma. Surg Neurol Int 12: 438, 2021
- 16) Ban SP, Hwang G, Byoun HS, et al.: Middle meningeal artery embolization for chronic subdural hematoma. Radiology 286: 992-999, 2018
- 17) Fiorella D, Arthur AS: Middle meningeal artery embolization for the management of chronic subdural hematoma. J NeuroIntervent Surg 11: 912-915, 2019
- 18) Ng S, Derraz I, Boetto J, et al.: Middle meningeal artery embolization as an adjuvant treatment to surgery for symptomatic chronic subdural hematoma: a pilot study assessing hematoma volume resorption. J Neurointervent Surg 12: 695-699, 2020
- 19) Hashimoto T, Ohashi T, Watanabe D, et al.: Usefulness of embolization of the middle meningeal artery for refractory chronic subdural hematomas. Surg Neurol Int 4: 104, 2013
- 20) Link TW, Rapoport BI, Paine SM, Kamel H, Knopman J: Middle meningeal artery embolization for chronic subdural hematoma: endovascular technique and radiographic findings. Interv Neuroradiol 24: 455-462, 2018
- 21) Mandai S, Sakurai M, Matsumoto Y: Middle meningeal artery embolization for refractory chronic subdural hematoma. Case report. J Neurosurg 93: 686-688, 2000
- 22) Kim E: Embolization therapy for refractory hemorrhage in patients with chronic subdural hematomas. World Neurosurg 101: 520-527, 2017
- 23) Chon KH, Lee JM, Koh EJ, et al.: Independent predictors for recurrence of chronic subdural hematoma. Acta neurochir (Wien) 154: 1541-1548, 2012
- 24) Torihashi K, Sadamasa N, Yoshida K, Narumi O, Chin M, Yamagata S: Independent predictors for recurrence of chronic subdural hematoma: a review of 343 consecutive surgical cases. Neurosurgery 63: 1125-1129, 2008
