Abstract
PulseRider (Cerenovus, Irvine, CA, USA) is a relatively novel device used for the treatment of wide-neck aneurysms with a coil-assisted effect. However, treatment options for recurrent aneurysms after PulseRider-assisted coil embolization remain controversial. Here we report a case of recurrent basilar tip aneurysm (BTA) treated with Enterprise 2 after PulseRider-assisted coil embolization. A woman in her 70s underwent coil embolization for a subarachnoid hemorrhage with ruptured BTA 16 years ago. Recurrence was detected at 6-year follow-up, and an additional coil embolization was performed. Nevertheless, gradual recurrence still occurred, and PulseRider-assisted coil embolization was performed without any complications 9 years after the second treatment. However, recurrence was detected once more at 6-month follow-up. Thus, stent-assisted coil embolization using Enterprise 2 (Cerenovus) through PulseRider was selected for angular remodeling. Enterprise 2 was deployed between the right P2 segment of the posterior cerebral artery (PCA) and basilar artery (BA) after an effective coil embolization, which achieved effective angular remodeling between the right PCA and BA. The patient's postoperative course was uneventful, and no recanalization was detected after half a year. Although PulseRider is effective for wide-neck aneurysm treatment, recurrence remains a possibility. Additional treatment using Enterprise 2 is safe and effective with the expectation of angular remodeling.
Introduction
Remarkable advances have been made in the endovascular treatment of unruptured cerebral aneurysms, with several devices available for treatment. PulseRider (Cerenovus, Irvine, CA, USA) is one such device used for aneurysm neck reconstruction. It is a relatively new device that has been available in Japan since 2020. Some reports have shown that this device achieves adequate occlusion (Raymond occlusion classification classes I and II) in 87.5%-92.7% of patients at 6-24 months follow-up, with a postoperative complication rate of 0%-8.8%.1-6) Thus, PulseRider use is becoming increasingly popular because of its efficacy and safety. Conversely, a certain number of recurrent aneurysms have been identified after PulseRider-assisted coil embolization, and there is no established treatment for these cases.1,3-6) Here, we report a case of a recurrent basilar tip aneurysm (BTA) treated with Enterprise 2 (Cerenovus) after PulseRider treatment.
Case Report
A 77-year-old woman with a history of hypertension and smoking habits underwent coil embolization 16 years ago for subarachnoid hemorrhage (SAH) caused by a ruptured BTA. She had an uneventful postoperative course and a modified Rankin Scale score (mRS) of 1 at the time of discharge due to the intraoperative complication of visual disturbance. Recurrence occurred 6 years later, and coil embolization was performed again. Despite additional coil embolization, gradual aneurysm recurrence was detected, and she was referred to our hospital 9 years after the second treatment. Digital subtraction angiography (DSA) at our hospital revealed a large BTA with an anterior bleb, which had maximum diameters of 16 mm at the dome and 8.5 mm at the neck (Fig. 1A, B). The previous coils were compacted upward and backward (Fig. 1C, D). We scheduled PulseRider-assisted coil embolization for this aneurysm. Dual antiplatelet therapy (aspirin 100 mg/day and clopidogrel 75 mg/day) was initiated 2 weeks before the treatment. Informed consent was obtained from the patient for the case report.

A microcatheter (Prowler Select Plus, Cerenovus) was guided from the left vertebral artery (VA) to the basilar artery (BA), and a T-shaped PulseRider was successfully deployed in a hybrid-type configuration: the right leaf in the right posterior cerebral artery (PCA) and the left leaf in the aneurysm (Fig. 1C, D). For coiling, two microcatheters (Excelsior SL-10, Stryker, Fremont, CA, USA, and Headway17, Terumo, Tokyo, Japan) were inserted into the aneurysm via the leaf of the PulseRider from the right VA. Thus, we performed an effective PulseRider-assisted coil embolization. The PulseRider was detached after coiling. Postoperative DSA showed appropriate occlusion, which was equivalent to Raymond occlusion classification class II (Fig. 1E, F). No intraprocedural complication occurred, and the patient had an uneventful postoperative course with an mRS score of 1 at discharge. Dual antiplatelet therapy was gradually decreased after 3 months.
Second treatment
Magnetic resonance angiography at 6-months follow-up revealed the fourth recurrence of the aneurysm, which required additional treatment (Fig. 1G, H). Therefore, we performed a double-catheter technique and stent-assisted coil embolization using Enterprise 2 for angular remodeling. Dual antiplatelet therapy was restarted 2 weeks before the treatment. Because the BA tip is narrow for triple catheters, a microcatheter for stenting (Prowler Select Plus) was guided from the left VA to the lower BA, and only a micro-guide wire (Synchro2 soft, Stryker, Fremont, CA, USA) was guided to the right PCA (Fig. 2A, B). Crossing the lesion with the micro-guide wire through the PulseRider was easy. Subsequently, two microcatheters were inserted for coiling to the aneurysm through the PulseRider from the right VA (Fig. 2C). Finally, a microcatheter for stenting (Prowler Select Plus) was navigated to the right PCA, and Enterprise 2 was deployed between the right P2 segment of the PCA and BA after coil embolization (Figs. 2D, E, F and 3A, B). After stenting, apposition of Enterprise 2 was assessed with cone-beam computed tomography. Postoperative DSA showed appropriate occlusion equivalent to Raymond occlusion classification class II, and no complications such as the displacement of the PulseRider or sagging were observed (Fig. 3C, D). Angular remodeling between the right PCA and BA was observed after the treatment (Fig. 4). The patient had no complications and was discharged with an unchanged mRS score. DSA after 6 months showed no obvious recurrence, and the dose of dual antiplatelet therapy was tapered off thereafter (Fig. 3E, F).

Discussion
BTAs account for 5% of all intracranial aneurysms and have a slightly higher recurrence rate after coil embolization than that of aneurysms at other sites.7,8) There are several indicators for predicting the recurrence of BTAs: larger size, dome/neck ratio ≤2, posterior dome orientation, angle between BA and BTA of 160°-180°, symmetrical PCA on both sides, and cranial BTA.9) Furthermore, in the embolization method itself, stent-embolized aneurysms have a lower recurrence rate than that of nonstented aneurysms, and Y-stent placement has been reported to have a lower recurrence rate than that of single-stent placement.10) However, the drawbacks of Y-stenting include difficulty in positioning at a steep angle, the procedure is technically complex, and there are relatively frequent complications.11) PulseRider is known to be easier to use in cases of steep angulation of bifurcation branches and has lower metal coverage than Y-stenting.1) Therefore, it is likely to be advantageous for procedural ischemic events.4,6,11,12) Long-term therapeutic effects have been reported to be similar to those of Y-stenting, but larger aneurysms are more likely to recur than in Y-stents.6,11) This may be explained by a reduced flow diversion effect, and direct flow to the aneurysm cannot be changed in a large terminal-type aneurysm like that in our case.1,6)
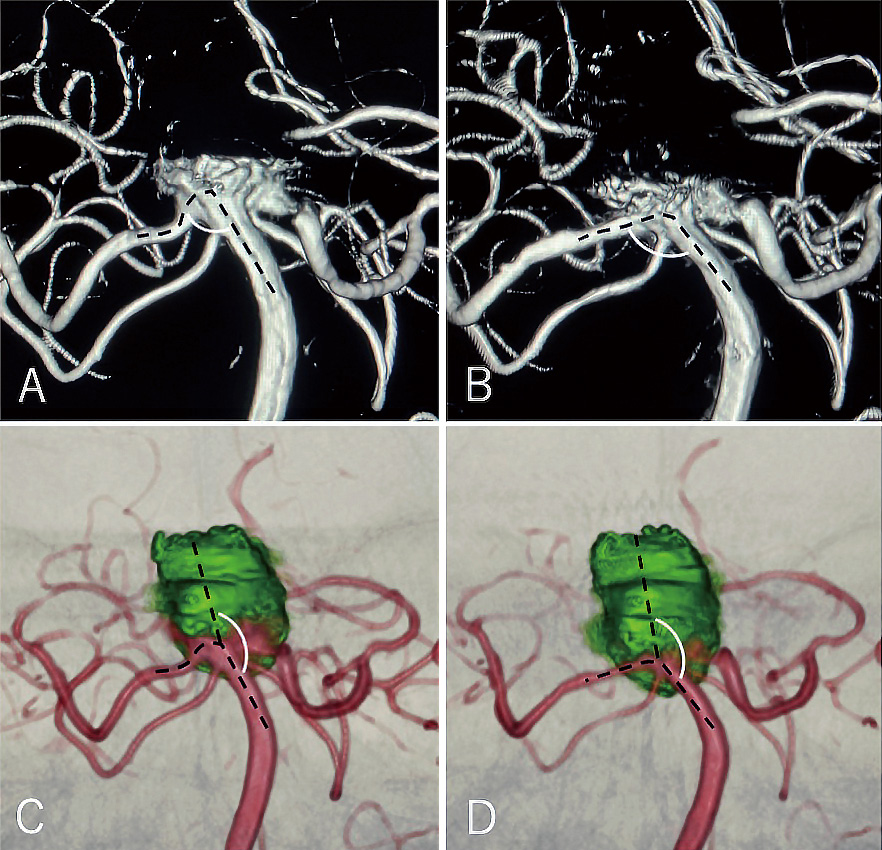
The hemodynamic effects of intracranial bifurcation aneurysms have been reported to be significantly improved by straightening the parent artery with flow diversion by metallic coverage.13) Vascular straightening by stenting dramatically alters apex hemodynamics in a favorable direction by blunting apical pressure, including the narrowing and migration of the flow impingement zone.14) Therefore, straightening the parent artery with a stent may be the optimal way to reduce the recurrence of intracranial bifurcation aneurysms.13) It has also been reported that parent artery straightening is likely to be involved in higher occlusion rates in flow-diverter stents.15) Specifically, it has been shown that a vessel angle of 20° or more likely indicates stable aneurysms, regardless of neck or aneurysm size.16) In our case, the angle actually changed by more than 20° (Fig. 4A, B). In addition, the angle of BA and BTA, the wide angle of which can predict risk of recurrence, decreased from 170° to 150° (Fig. 4C, D).9)
Owing to its relatively open design and low metal loading, PulseRider is known to not preclude further endovascular interventions such as adding coils or placing a stent through the device.3) Similar to our case, very few studies conducted stent placement through PulseRider, and none of these cases reported complications.1,3,17) So far, LVIS/LVIS Jr (Microvention Terumo, Tustin, CA, USA) and Neuroform Atlas (Stryker) have been reported for BTA,1,3) and Enterprise 2 and LVIS Jr for anterior communicating artery aneurysm.3,17) However, there were no reports of Enterprise 2 for BTA. Enterprise 2 is effective in that it can be placed without difficulty for BTA after PulseRider placement and has the potential for better angular remodeling than other stents (Fig. 2).13,18) Therefore, Enterprise 2-induced remodeling of the BTA aneurysm appears to be the better method for decreasing recurrence after PulseRider placement.13) Because PulseRider has low metal coverage, the risk of thrombus formation is low and there is a high possibility that even if a stent is added, it can be treated with the same antiplatelet therapy as that after normal single-stent placement.3,5)
In conclusion, we report a case of recurrent BTA after PulseRider-assisted coil embolization treated with Enterprise 2. Additional coil insertion and stent placement through PulseRider was easy, and angular remodeling was confirmed. Stent-assisted coil embolization using Enterprise 2 after PulseRider placement was a viable and safe option, which prevented further recurrences.
Conflicts of Interest Disclosure
All authors report no conflicts of interest concerning this article.
References
- 1) Spiotta AM, Derdeyn CP, Tateshima S, et al.: Results of the ANSWER trial using the PulseRider for the treatment of broad-necked, bifurcation aneurysms. Neurosurgery 81: 56-65, 2017
- 2) Suyama K, Nakahara I, Matsumoto S, et al.: Brainstem infarctions caused by a proximal marker of the PulseRider device obstructing the origin of a perforator. J Stroke Cerebrovasc Dis 31: 106332, 2022
- 3) Srinivasan VM, Srivatsan A, Spiotta AM, et al.: Early postmarket results with PulseRider for treatment of wide-necked intracranial aneurysms: a multicenter experience. J Neurol Surg 133: 1756-1765, 2020
- 4) Spiotta AM, Chaudry MI, Turner RD 4th, et al.: An update on the adjunctive neurovascular support of wide-neck aneurysm embolization and reconstruction trial: 1-year safety and angiographic results. AJNR Am J Neuroradiol 39: 848-851, 2018
- 5) Sakai N, Imamura H, Arimura K, et al.: PulseRider-assisted coil embolization for treatment of intracranial bifurcation aneurysms: a single-center case series with 24-month follow-up. World Neurosurg 128: e461-e467, 2019
- 6) Pranata R, Yonas E, Vania R, Sidipratomo P, July J: Efficacy and safety of PulseRider for treatment of wide-necked intracranial aneurysm-A systematic review and meta-analysis. Interv Neuroradiol 27: 60-67, 2021
- 7) Schievink WI, Wijdicks EFM, Piepgras DG, Chu CP, O'Fallon WM, Whisnant JP: The poor prognosis of ruptured intracranial aneurysms of the posterior circulation. J Neurosurg 82: 791-795, 1995
- 8) Raymond J, Guilbert F, Weill A, et al.: Long-term angiographic recurrences after selective endovascular treatment of aneurysms with detachable coils. Stroke 34: 1398-1403, 2003
- 9) Songsaeng D, Geibprasert S, Ter Brugge KG, Willinsky R, Tymianski M, Krings T: Impact of individual intracranial arterial aneurysm morphology on initial obliteration and recurrence rates of endovascular treatments: a multivariate analysis. J Neurosurg 114: 994-1002, 2011
- 10) Chalouhi N, Jabbour P, Gonzalez LF, et al.: Safety and efficacy of endovascular treatment of basilar tip aneurysms by coiling with and without stent assistance: a review of 235 cases. Neurosurgery 71: 785-794, 2012
- 11) Limbucci N, Cirelli C, Valente I, et al.: Y-stenting versus PulseRider-assisted coiling in the treatment of wide-neck bifurcation aneurysms: role of anatomical features on midterm results. Neurosurgery 87: 329-337, 2020
- 12) Fargen KM, Mocco J, Neal D, et al.: A multicenter study of stent-assisted coiling of cerebral aneurysms with a y configuration. Neurosurgery 73: 466-472, 2013
- 13) Wan H, Lu G, Ge L, et al.: Hemodynamic effects of stent-induced straightening of parent artery vs. stent struts for intracranial bifurcation aneurysms. Front Neurol 12: 802413, 2022
- 14) Gao B, Baharoglu MI, Malek AM: Angular remodeling in single stent-assisted coiling displaces and attenuates the flow impingement zone at the neck of intracranial bifurcation aneurysms. Neurosurgery 72: 739-748, 2013
- 15) Janot K, Fahed R, Rouchaud A, et al.: Parent artery straightening after flow-diverter stenting improves the odds of aneurysm occlusion. Am J Neuroradiol 43: 87-92, 2022
- 16) Ishii A, Chihara H, Kikuchi T, Arai D, Ikeda H, Miyamoto S: Contribution of the straightening effect of the parent artery to decreased recanalization in stent-assisted coiling of large aneurysms. J Neurosurg 127: 1063-1069, 2017
- 17) Valente I, Limbucci N, Nappini S, Rosi A, Laiso A, Mangiafico S: Enterprise deployment through PulseRider to treat anterior communicating artery aneurysm recurrence. World Neurosurg 110: 158-161, 2018
- 18) Saied A, Elsaid N, Joshi K, et al.: Factors affecting the degree of angular remodeling in stent-assisted coiling of bifurcation aneurysms. Interv Neurol 8: 220-230, 2020