CASE REPORT
Spontaneous Regression of Rathke's Cleft Cysts: A Report of Three Cases
2025 Volume 12 Pages 79-84
Details
2025 Volume 12 Pages 79-84
Herein, we present 3 cases of Rathke's cleft cysts that shrank spontaneously within a short period. In addition, we present a literature review, discussing the characteristics and of action mechanisms of rapid Rathke's cleft cyst regression. Case 1 was that in a 17-year-old boy diagnosed with an Rathke's cleft cyst on the basis of magnetic resonance imaging. The Rathke's cleft cysts had expanded to compress the optical chiasm. Therefore, surgical intervention was planned. However, without any medical treatment, magnetic resonance imaging performed 3 months later revealed a spontaneous reduction in size, and surgery was canceled. Case 2 was in a 10-year-old boy who presented with a severe headache. Surgery was planned for a sellar cystic lesion; however, magnetic resonance imaging performed 2 months later revealed spontaneous shrinkage without any treatment. The patient's symptoms disappeared, and the surgery was canceled. Case 3 was in a 25-year-old man who presented with a headache. Magnetic resonance imaging at presentation revealed a cystic lesion in the sella turcica, but repeat magnetic resonance imaging 4 months later revealed spontaneous shrinkage. Fifty-nine cases of spontaneously shrinking Rathke's cleft cysts, initially characterized by severe headache (54.2%), have been reported; of these, 57% of cases were in patients younger than 39 years. Furthermore, 64% of patients showed evidence of cyst reduction on magnetic resonance imaging within 6 months. Type 1-weighted magnetic resonance imaging scans showed isointensity or high signal intensity in 91% of cases. In conclusion, spontaneous shrinkage of Rathke's cleft cysts can occur within a few months. Type 1-weighted images are characterized by high signal intensity, and episodic headaches may indicate shrinkage. The possibility of short-term regression of Rathke's cleft cyst should be considered before scheduled surgery.
Rathke's cleft cysts (RCCs) are benign cystic lesions that originate from remnants of the epithelial lining of Rathke's pouch and are often found incidentally in patients with no symptoms.1) However, some patients present with headaches, visual dysfunction, and endocrine disorders that require surgical treatment.2) Imaging findings inside the cyst and its natural history can also vary.3) In the present study, we describe 3 cases of RCCs that shrank spontaneously in a short period. In addition, we provide a literature review discussing the characteristics and mechanisms of the rapid regression of RCCs.
A 17-year-old boy presented with headache and was diagnosed with RCC on the basis of magnetic resonance imaging (MRI) performed at a hospital (Fig. 1A and B). Four years later, severe headache and eye pain suddenly developed in the patient. He visited his previous physician, who identified an enlarged lesion on MRI and referred him to our hospital. The patient had no neurologic abnormalities but reported poor vision. Blood test results revealed a low prolactin level (PRL) of 0.30 ng/mL (normal range: 2-18); however, other parameters, including growth hormone (GH) of 0.85 ng/mL (<2.48), adrenocorticotropic hormone (ACTH) of 20.3 pg/mL (7.2-63.3), luteinizing hormone (LH) of 0.92 mIU/mL (1.8-8.6), follicle stimulating hormone (FSH) of 2.14 mIU/mL (1.5-12.4), cortisol of 10.6 μg/dL,3-16) and thyroid stimulating hormone (TSH) of 1.72 mIU/mL (0.35-4.94) showed no abnormalities at baseline. MRI at our institute revealed a mass in the sellar region compressing the optic chiasm. The mass showed a high signal on Type 1 (T1)-weighted imaging and a low signal on Type 2-weighted imaging, indicative of an intracystic nodule with high-signal content. Contrast-enhanced T1-weighted imaging revealed a pituitary stalk, normal gland, and no internal contrast effect. These findings are consistent with those of RCC (Fig. 1C and D). Compared with the MRI performed 4 years prior, the cyst had increased in size from 15 to 19 mm. Surgery was scheduled to relieve the compression of the optic chiasm. Three months later, the patient was admitted to the hospital for surgery, and MRI was performed again. The mass was revealed to be markedly reduced in size, and the optic chiasm was no longer compressed (Fig. 1E and F). The patient's headaches disappeared, and the surgery was canceled. Two years later, follow-up MRI showed no re-enlargement of the cyst, whereas blood tests showed no endocrine deterioration.

Case 1. Sagittal T1-weighted MRI showing a high intensity mass in the sellar region (A). After Gd administration, the pituitary stalk and normal pituitary gland became enhanced (B). Sagittal T1-weighted MRI with Gd enhancement performed at the onset of severe headache showing enlargement of the mass (C). Coronal T2-weighted image showing the mass compressing the optic chiasm (D). Sagittal (E) and coronal (F) T1-weighted MRI with Gd enhancement showing a shrinkage of the mass 3 months after symptom onset.
Gd: gadolinium; MRI: magnetic resonance imaging; T1: type 1; T2: type 2
A 10-year-old boy was found to have vision deterioration after scoring significantly lower on a vision test than 1 year before presentation. Visual acuity testing revealed that his vision had deteriorated (20/25 in right, 20/4 in left) from 20/20 in both eyes a year earlier, and visual field testing indicated superior temporal quadrantanopia (Fig. 2). At the end of the same year, episodic headache and nausea led to a referral to a local doctor for examination. No other abnormal neurological findings were identified. Blood test results showed a high GH of 4.66 ng/mL, but other hormones (ACTH 22.3 pg/mL, LH 1.1 mIU/mL, FSH 2.4 mIU/mL, cortisol 10.3 μg/dL, TSH 2.56 mIU/mL, and PRL 6.36 ng/mL) showed no abnormalities. MRI showed a cystic mass in the sellar region. With gadolinium administration, T1-weighted images showed the pituitary stalk and gland with no internal contrast effect, consistent with RCC (Fig. 3A and B). The patient was deemed a candidate for surgery owing to the evidence of optic chiasmatic compression, visual symptoms, and headache. Two months later, the patient was admitted to our hospital for surgery. When another MRI scan was performed, the mass had spontaneously shrunk (Fig. 3C and D). Because there were no headaches or visual disturbances, the surgery was canceled. Three years later, MRI showed no re-enlargement of the cyst, and blood tests showed no endocrine deterioration.
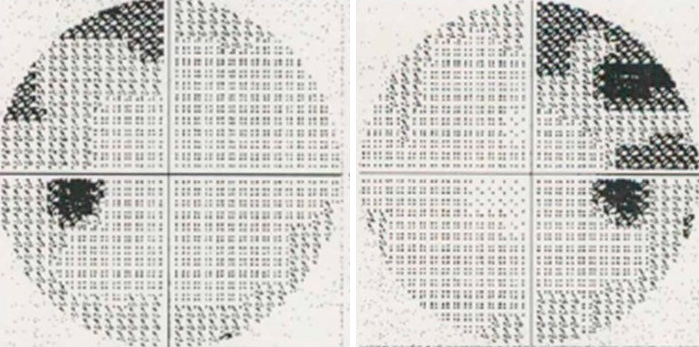
Case 2. Visual field testing indicated superior temporal quadrantanopia.

Case 2. Sagittal and coronal T1-weighted MRI with Gd enhancement showing a cystic mass in the sellar region (A and B). Follow-up MRI showing shrinkage of the mass (C and D).
Gd: gadolinium; MRI: magnetic resonance imaging; T1: type 1
A 25-year-old man presented with sudden severe headache, after which he was found to have a pituitary lesion on MRI at a hospital. The patient reported that his bilateral corrected vision had deteriorated 6 months earlier and that his glasses had to be adjusted. The following month, he began to experience difficulty focusing his eyes and was subsequently referred to our hospital for examination. No neurological abnormalities were observed at this point. MRI showed a cystic mass in the sellar region, with a high signal intensity on T1-weighted imaging (Fig. 4A). The patient was deemed to be a candidate for surgery owing to optic chiasmatic compression and visual symptoms. Four months later, the patient was admitted to our hospital for surgery. When the MRI was repeated, the mass had shrunk spontaneously (Fig. 4B). The visual impairment observed 3 months earlier had also been alleviated, and surgery was discontinued. Almost 3 years later, MRI showed no re-enlargement of the cyst, whereas blood tests showed no evidence of endocrine dysfunction.

Case 3. Coronal T1-weighted MRI showing an isointensity mass causing optic chiasm compression (A). Coronal T1-weighted MRI with Gd administration performed 4 months after the onset of severe headache, showing a shrinkage of the mass (B).
Gd: gadolinium; MRI: magnetic resonance imaging; T1: type 1
RCCs are benign lesions that constitute 1.8% of all tumors in the sella.4) Most RCCs remain asymptomatic and do not require intervention.2) However, follow-up through routine imaging is recommended for asymptomatic RCCs, which can undergo spontaneous regression in rare cases.3-10) The findings of 3 cases we experienced are summarized in Table 1. All patients showed cystic masses on MRI with no calcification. The cyst contents showed a high signal-to-iso-signal ratio on T1-weighted images. In addition, only the normal pituitary stalk and gland showed contrast, consistent with RCC. All 3 patients were young males with headache and visual symptoms. The headaches were sudden and intense. The maximum diameter ranged from 16 to 19 mm, which is relatively small. The lesions were in contact with the optic nerve and caused visual symptoms. Spontaneous regression occurred in a short period of 2 to 4 months without any treatment. Reduction rates ranged from 91% to 97%.

Summary of three cases of spontaneous regression of RCC
We searched the PubMed databases for past reports using the keywords "Rathke's cleft cyst," "RCC," "involution," "shrinkage," "vanishing," "reduction," and "regression," identifying 59 cases of spontaneously shrinking RCCs published in 22 papers from 1991 to the present, including autologous cases.1-23) The common features of these reports were as follows: Episodic and severe headaches were reported by 54.2% of the patients. Indeed, headache has been reported as the most common symptom in the past literature,11) which subsides at the time of reduction. Subjects younger than 39 years accounted for 57% of cases, and in many cases, lesions shrank without treatment.3,5,7,9,19) The time to spontaneous regression varied from 0.5 to 27 months, but in 64% of cases, lesions shrank within 6 months. T1 MRI images showed an iso-to-high signal in 91% of the cases. These features were common to all 3 cases. Surgery was canceled in several of the reported cases.5,12) Several reports described cases showing hypopituitarism,1,5,7,11-16) with hormonal replacement required in some;11) however, this feature was not observed in our cases.
The exact mechanisms underlying the spontaneous regression of RCCs are unknown, but several hypotheses have been proposed, including an imbalance between secretion and absorption within the cyst due to inflammation.5) RCCs contain inflammatory secretions in the cyst wall. Many cysts with a reduced size are depicted as hyperintense areas on T1-weighted images, reflecting a high protein content that may occur because of inflammation. Saeki et al.17) also reported that RCCs with high signal intensity on T1-weighted images are smaller than cysts with low signal intensity and cause more clinical symptoms. These MRI signals indicate that chronic inflammation may be involved in the pathogenesis of several cases of pituitary dysfunction, although no pituitary dysfunction was observed in our cases. Other studies have suggested that cyst rupture may be a factor influencing cyst regression, with intracystic hypersecretion or minor hemorrhage possibly preceding rupture.6,11) Cheng et al.8) also hypothesized that headache is a sign of increased intrasellar pressure. In our case, headaches triggered MRI, which led to the diagnosis. During follow-up, the symptoms disappeared, and spontaneous regression of the cyst was observed on reevaluation of the images. Maruyama et al.13) suggested that the inflammatory nature of RCCs could explain the short-term size changes in response to glucocorticoid administration. Furthermore, Amhaz et al.5) suggested that spontaneous regression may be more prevalent than suggested in previous reports given the natural course of RCCs is not yet fully understood.
In our cases, we observed marked spontaneous regression between 2 and 4 months. Although it is difficult to determine the exact follow-up period, it has been suggested that spontaneous regression may occur within a timeframe shorter than 1 year, as previously reported.8) The management of asymptomatic RCCs is controversial, and given the possibility of spontaneous regression, a conservative approach may be favored among patients presenting with headache-only symptomatic RCCs. RCCs commonly show unpredictable natural tendencies and may later become larger or, as in our case, rarely become smaller. As such, lesions should be re-evaluated clinically or through imaging scans immediately before surgery.
One major limitation of our case report is that no pathological features or findings of intracystic hemorrhage or inflammatory changes could be confirmed because the actual tissue was not obtained. With the increasing trend toward minimally invasive surgery for RCCs, further research on the natural history of symptomatic and asymptomatic RCCs is warranted. Our report may therefore help clinicians to select the appropriate treatment and timing of surgery for RCCs.
This study did not receive any specific grants from funding agencies in the public, commercial, or non-profit sectors.
Subjects provided informed consent to disclose information and images about their experiences.
Author Nakada Mitsutoshi is one of the Editorial Board members of the Journal. This author was not involved in the peer-review or decision-making process for this paper.
Both authors have no conflict of interest.