抄録
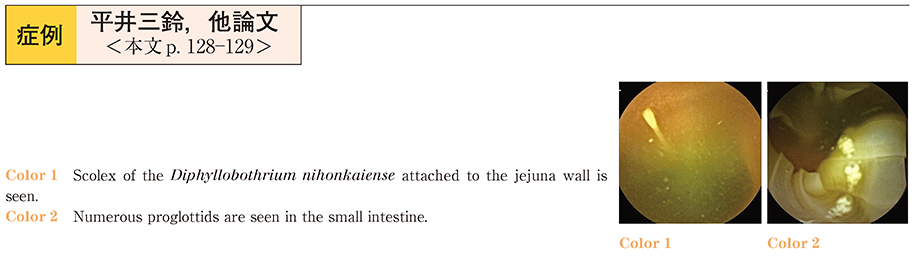
A 40-year-old man presented to our hospital with the complaint of long white string-like discharges from the anal. No significant abnormality was noted on physical examination. He had history of diabetes mellitus, thus, the laboratory tests revealed a markedly increased HbA1c level (13.3%) . The serum IgE level was slightly increased (645 IU/ml) . Other laboratory values were within normal range. He gave a history of eating raw Oncorhynchus masou 2 months earlier, and had been diagnosed as having Diphyllobothrium nihonkaiense by evaluation of the expelled proglottids. Therefore, vermifuge treatment with gastrografin was started, however, we could not identify the tape worm and no proglottids were excreted. Therefore, the patient was kept under observation, and 16 months later, he presented again with the same complaint. We performed capsule endoscopy to confirm whether the scolices could be found in the bowel ; this examination revealed scolices of Diphyllobothrium nihonkaiense attached to the jejunal wall, as well as numerous freely floating proglottids in the small intestine. Praziquantel (20 mg/kg) was administered, followed by administration of a cathartic 2 hours later, and the worm was expelled successfully. It was considered that capsule endoscopy was very useful for the diagnosis of the parasites in this case.