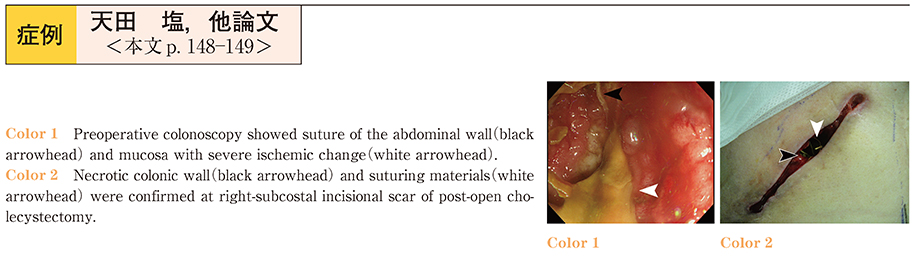
A 76-year-old man was admitted to our hospital with the complaint of stool discharge from a right subcostal incisional scar following open cholecystectomy performed 23 days earlier. He had undergone distal gastrectomy 20 years ago and partial small-intestinal resection 17 years ago. Hematological examination showed elevation of the inflammatory reaction markers (WBC 11,700/μl, serum CRP 10.1 mg/dl) . CT showed an enteroctaneous fistula between the transverse colon and subcostal scar. Preoperative colonoscopy showed a small perforation with overhanging mucosa and severe ischemic change at the transverse colon near the hepatic flexure. Absorbable suturing materials of the abdominal wall were also recognized. Fistulography was performed and the fistula and scar were visualized. Laparotomy was performed 28 days after the open cholecystectomy. The transverse colon around the fistula showed segmental necrosis. Right hemicolectomy and ileo-colostomy were performed. The patient was discharged from the hospital 24 days after the surgery. Preoperative colonoscopy was useful to determine the operative procedure with colectomy.