抄録
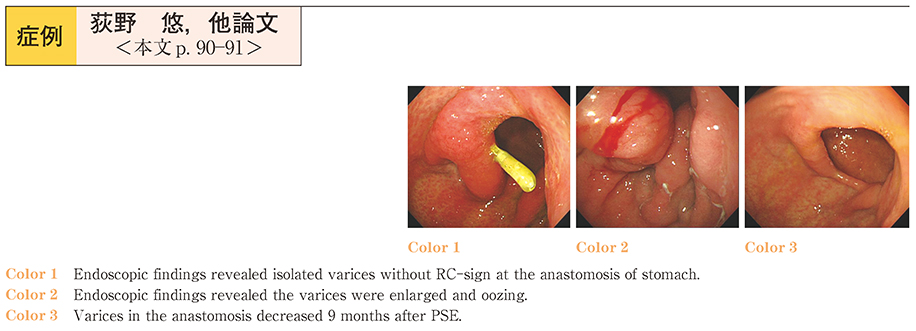
We report the case of a 70-year-old man who was admitted to another hospital with a chief complaint of hematochezia. He had undergone total gastrectomy 15 years ago. Abdominal computed tomography (CT) showed complete obstruction of the splenic vein by a tumor in the head of the pancreas. He was then referred to our hospital for further management of anemia and the pancreatic tumor. Upper gastrointestinal endoscopy revealed isolated varices lacking the red color sign in the region of the gastric anastomosis. We made the diagnoses of pancreatic head cancer based on the findings on the cytological specimens obtained by endoscopic retrograde cholangiopancreatography, and left-sided portal hypertension due to splenic vein invasion of the tumor based on the CT findings. Because we could not conclude that the bleeding was caused by the varices, we started the patient on chemotherapy and kept her under observation. During the hospitalization, however, the hematochezia recurred repeatedly, and two blood transfusions were required. Upper gastrointestinal endoscopy performed a second time revealed enlarged and oozing varices, and we performed partial splenic artery embolization (PSE) to reduce the blood ooze from the site of bleeding. Well-developed collateral circulation was seen at the splenic hilum and we performed 80% embolization using Gelfoam and metallic coils. The PSE reduced the varices in the anastomosis, and nine months later, the varices had almost disappeared entirely. Left-sided portal hypertension complicated by pancreatic cancer is comparatively rare. In the present case, PSE was effective for stemming the bleeding from the gastric varices.