ABSTRACT
Background: Descending necrotizing mediastinitis is a potentially fatal
polymicrobial infection that often leads to dysphagia after treatment. Such dysphagia is
likely the result of fibrosis and scarring from inflammatory changes in the fascial space.
A case is presented in which the mechanism of dysphagia was verified using two-dimensional
analysis of the muscle lengths of the suprahyoid and infrahyoid muscles.
Case: A 57-year-old woman presented with a hyoid and laryngeal movement
disorder with pharyngeal residue secondary to descending necrotizing mediastinitis. To
treat this disorder, the chin-down maneuver was performed, and it immediately improved
hyoid and laryngeal elevation and reduced pharyngeal residue at the epiglottic valleculae
and pyriform sinus. Analysis of the mechanism of these improvements revealed that combined
head and neck flexion, compared with neck flexion, decreased the distance between the
origin and insertion (DOI) of the sternohyoid muscle (SM) and increased the muscle
contraction rate and the maximum contraction duration of the geniohyoid muscle (GM) during
swallowing. Discussion: In the present case, the patient had restrictions in
extension of the SM that applied resistance to GM contraction. Compensation of this
condition was achieved by combined head and neck flexion, which decreased the DOI of the
SM, thereby improving the contractile function of the GM.
INTRODUCTION
Cervical necrotizing fasciitis, commonly of pharyngeal, tonsillar, or odontogenic origins,
is a rare polymicrobial infection. Reports show that in 40–45% of cases, cervical
necrotizing fasciitis spreads rapidly to the mediastinum, often becoming fatal.1) Prompt diagnosis and treatment of
descending necrotizing mediastinitis (DNM), e.g., securing the airway, administering
antibiotics, performing drainage, and providing intensive care for sepsis, can contribute to
improved survival. Complications include a compromised airway, jugular vein thrombosis,
suppurative jugular thrombophlebitis (Lemierre’s syndrome), carotid artery erosion and
rupture, septic shock, empyema, and a bronchocavitary fistula.2)
Dysphagia can persist after DNM treatment. Such dysphagia is thought to be caused by
movement disorder of the hypopharyngeal muscle and hyoid/thyroid cartilage that develops as
a result of fibrosis and scarring caused by the inflammatory changes in the fascial
space.3,4) However, the mechanism remains a
matter of speculation. There are very few reports on rehabilitation for this
condition,5) probably
because of the absence of detailed swallowing evaluations. This report describes the
intensive rehabilitation and videofluorographic swallowing study (VFSS) performed after DNM
diagnosis. The chin-down procedure was successful in treating dysphagia in the present
patient; however, no similar reports have been published to date. Consequently, a
two-dimensional analysis of the lengths of the suprahyoid muscles (SHMs) and infrahyoid
muscles (IHMs) was conducted to determine whether the chin-down compensation mechanism is
consistent with the hyoid and laryngeal movement disorder caused by fibrosis and scarring,
as suggested by previous reports.
CASE
A 57-year-old woman visited her local physician because of severe throat pain, a swollen
neck, and a high fever that had persisted for several days. Ten days before the visit, dried
anchovy became lodged in the patient’s throat. The patient did not have a medical history
suggestive of a high risk of infection (e.g., diabetes mellitus) or decreased swallowing
function (e.g., stroke). Computed tomography showed a deep bilateral neck abscess and
inflammation from the neck to the mediastinum, along with gas formation. With the diagnosis
of DNM, the patient was transported and admitted to an emergency hospital. On the same day,
bilateral cervical drainage and thoracic surgical drainage with video-assisted thoracoscopy
from the left thoracic cavity were performed. Postoperatively, antibiotic treatment, sepsis
management, and peripheral parenteral nutrition were continued. One week after admission,
tracheostomy was performed, and nasogastric tube feeding and physical therapy, including
respiratory function training, were started. Four weeks after admission, the inflammatory
response, neck abscess, and mediastinitis improved. A jelly diet was started, but the
patient developed mild hoarseness (breathy/wet) and showed bilateral vocal cord paresis on
laryngoscopy. The patient’s oral intake was level 3 on the Functional Oral Intake Scale
(FOIS).6) A VFSS showed poor
hyoid and laryngeal elevation. To avoid water aspiration, thickening of the diet was
required. With a paste diet, significant pharyngeal residue was present at the epiglottic
valleculae and bilateral pyriform sinuses, and several swallows were required to remove the
residue. Five weeks after admission, swallowing exercises (i.e., neck range of motion
exercise, Shaker exercise, and effortful swallow) were started with a speech-language
pathologist. The FOIS improved to level 4, and the patient achieved independent activities
of daily living, including gait, and was transferred to our hospital 6 weeks after admission
for dysphagia rehabilitation. At the start of swallowing exercises and at the time of
hospital transfer, undernutrition was not evident, based on nutrition management screening,
such as blood test results.
Similar exercises and the jelly diet established by the previous physician were continued,
and the tracheal cannula (button type) was removed 7 weeks after admission. No obvious
restrictions in the range of motion of the head and neck were observed. On laryngoscopy,
vocal cord atrophy was evident, but vocal cord paralysis had improved. A VFSS done 8 weeks
after admission showed that water without thickening could be swallowed without aspiration,
and residue in the epiglottic valleculae was reduced with the paste diet. However, poor
hyoid and laryngeal elevation was evident, and multiple swallows were required to remove the
residue. The FOIS improved to level 5. A VFSS performed 10 weeks after admission also did
not show changes in hyoid and laryngeal elevation or residue at the epiglottic valleculae
and pyriform sinus. There were no obvious differences in the pharyngeal passage between the
left and right sides, and head rotation had no effect.
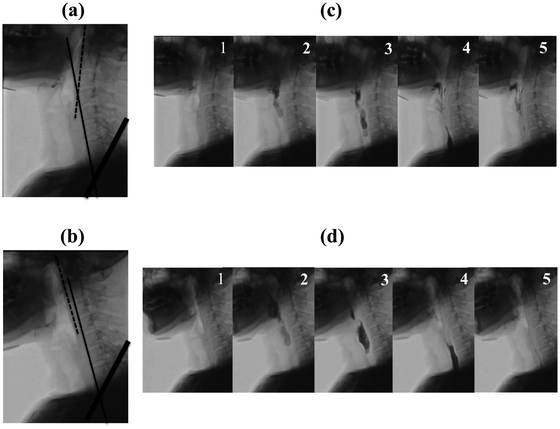
However, when a reduction in pharyngeal residue was attempted with the chin-down maneuver,
immediate improvement was achieved with combined head and neck flexion (CHNF), a finding not
observed with neck flexion (NF) alone. In other words, hyoid and laryngeal elevation
improved, and the paste diet could be swallowed without residue in the epiglottic valleculae
and pyriform sinuses. With such progress, after discharge, the patient was able to
transition stepwise from a jelly diet (FOIS: level 4) to a soft diet (FOIS: level 6).
Indeed, by discharge, the patient was already dropping her head voluntarily in a chin-down
posture when swallowing. Patient information about this case of dysphagia was shared among
the transdisciplinary team to determine whether to step up or maintain the food form.
However, undernutrition was not evident, and nutritional concerns were not raised by the
attending physician’s team.
We postulated that the impairment of IHM extension resulting from fibrosis and scarring
caused the dysphagia, compensation for which could be immediately achieved by the chin-down
maneuver. In other words, CHNF shortened the distance between the origin and the insertion
(DOI) of the IHMs, resulting in a relative relaxation of resting IHMs, thereby immediately
compensating for the impaired contraction of the SHMs.
To test this hypothesis, we proposed a measurement method from an integrated perspective to
simultaneously analyze the lengths of SHMs and IHMs in two-dimensions and conducted the
following validation study using VFSS. Informed consent to publish this case study was
obtained from the patient.
Outcome Measurements
A VFSS was performed 10 weeks after admission. As shown in Fig. 1, the patient sat in a comfortable 60° reclining position to
stabilize the chin-down posture. She was asked to swallow 3 ml of barium water or barium
paste with NF or CHNF on command. This was repeated six times, and lateral-view images
were recorded.
Recorded frame-by-frame images (30 frames per second) of the following four endpoints
were evaluated using two-dimensional motion analysis software (DIPP-Motion PRO 2D, DITECT
Corporation, Tokyo, Japan).
1) DOI of the Sternohyoid Muscle
Because the origin and insertion of both the right and left sternohyoid muscles (SMs)
run parallel to the midline of the anterior neck, we postulated that the outcome measure
would be similar to the actual muscle length even when measured as a virtual muscle
length on the VFSS lateral view. The DOI of the SM (DOI-SM) was measured as the distance
between the upper end of the manubrium of the sternum and the central portion of the
hyoid bone [Fig. 2(a)].
2) DOI of the Geniohyoid Muscle
In the lateral view of the VFSS, the hyoid bone during oropharyngeal swallowing
typically moves in the superior direction from the resting position, followed by
displacement in the anterior direction and a subsequent return to the resting position.
It has been reported that, of the SHMs, the mylohyoid muscle has the greatest potential
to displace the hyoid bone in the superior direction, and the GM has the greatest
potential to displace the hyoid bone in the anterior direction.7)
Because the origin and insertion of both the right and left GMs run parallel to the
midline of the lower jaw, we postulated that the outcome measure would be similar to the
actual muscle length, even when measured as a virtual muscle length on the VFSS lateral
view. This distance was measured with the hyoid in the anterior displacement start
position (b) and the anterior displacement end position (c) [Fig. 2(b), (c)].
3) Muscle Contraction Rate of the GM
The DOI-GM was converted to the muscle contraction rate (MCR). The MCR of the DOI-GM
was calculated as: MCR={[(b) minus (c)] divided by (b)}×100.
4) Maximum Contraction Duration of the GM
Using the first frame at the hyoid anterior displacement end position as a reference
(zero), stationary frames of the hyoid at that position over time were counted and
added: the maximum contraction duration (MCD) of the GM (s)=Total number of frames ×
1/30
Data Analysis
All statistical analyses were performed using the Statistical Package for the Social
Sciences (SPSS) version 20.0 (IBM, Armonk, NY, USA), with P values <0.05 indicating
significance. Normality was confirmed for the data of all groups using the Shapiro-Wilk
test. The t-test was used to compare each parameter before and after the
chin-down posture.
Results
Table 1 shows the DOI, MCR, and MCD values
for NF and CHNF.
Table 1.
Comparison of effects of NF and CHNF
|
|
NF |
CHNF |
|
|
|
Mean (SD) |
95% CI |
Mean (SD) |
95% CI |
P |
| DOI of the SM (mm) |
|
|
|
|
|
|
| 3 ml liquid |
|
77.9 (0.9) |
77.0–78.9 |
68.1 (1.2) |
66.8–69.3 |
0.000* |
| 3 ml paste |
|
77.5 (0.6) |
76.9–78.2 |
67.0 (1.2) |
65.7–68.2 |
0.000* |
| DOI of the GM (mm) |
|
|
|
|
|
|
| 3 ml liquid |
A |
35.3 (0.4) |
34.9–35.7 |
35.6 (0.3) |
35.1–36.0 |
0.274 |
|
B |
26.5 (0.3) |
26.2–26.8 |
25.3 (0.3) |
24.9–25.7 |
0.000* |
| 3 ml paste |
A |
35.5 (0.6) |
34.9–36.1 |
35.1 (0.5) |
34.6–35.7 |
0.226 |
|
B |
27.1 (0.6) |
26.5–27.7 |
24.3 (0.4) |
23.9–24.7 |
0.000* |
| MCR of the GM (%) |
|
|
|
|
|
|
| 3 ml liquid |
|
24.9 (0.9) |
24.0–25.8 |
28.8 (1.3) |
27.4–30.1 |
0.000* |
| 3 ml paste |
|
23.6 (0.9) |
22.6–24.6 |
31.1 (1.3) |
29.7–32.5 |
0.000* |
| MCD of the GM (s) |
|
|
|
|
|
|
| 3 ml liquid |
|
0.78 (0.17) |
0.60–0.96 |
1.34 (0.31) |
1.02–1.66 |
0.001* |
| 3 ml paste |
|
0.89 (0.17) |
0.71–1.07 |
1.67 (0.30) |
1.35–1.98 |
0.005* |
CHNF: combined head and neck flexion, DOI: distance between the origin and insertion,
GM: geniohyoid muscle, MCD: maximum contraction duration, MCR: muscle contraction
rate, NF: neck flexion, SM: sternohyoid muscle, A: hyoid in the anterior displacement
start position, B: hyoid in the anterior displacement end position.
P calculated by the t-test; *P <0.05.
Compared with NF, CHNF resulted in a significantly lower DOI-SM for both liquid
(77.9 mm vs. 68.1 mm) and paste (77.5 mm vs. 67.0 mm).
2) DOI of the Geniohyoid Muscle
Compared with NF, CHNF had a similar DOI-GM at the hyoid anterior displacement start
position, but significantly lower DOI-GM at the hyoid anterior displacement end position
for both liquid (26.5 mm vs. 25.3 mm) and paste (27.1 mm vs. 24.3 mm).
3) MCR of the Geniohyoid Muscle
Compared with NF, CHNF resulted in a significantly higher MCR-GM for both liquid (24.9%
vs. 28.8%) and paste (23.6% vs. 31.1%).
4) MCD of the Geniohyoid Muscle
Compared with NF, CHNF resulted in a significantly longer MCD-GM for both liquid (0.78
s vs. 1.34 s) and paste (0.89 s vs. 1.67 s).
DISCUSSION
The chin-down maneuver is a postural technique widely used in dysphagia treatment.
According to Logemann,8) one of
the primary effects of the chin-down posture is the proximity of the tongue base and
epiglottis to the posterior pharyngeal wall. This was corroborated in the present case, and
a reduction in residue at the epiglottic valleculae with the chin-down posture was confirmed
on VFSS.
Recently, Okada et al. reported that head flexion (HF), NF, and CHNF produce different
effects on the anteroposterior dimensions of the valleculae and the pharyngeal
lumen.9) Specifically, they
showed that the changes in the relationship between the food pathway and the airway caused
by the difference in the position of the head and neck explain the multifaceted effects of
the chin-down posture.
Nevertheless, there is only one report, by Matsubara et al., that verified the swallowing
pressure with three types of chin-down maneuvers (HF, NF, and CHNF).10) According to this report, NF was
the position that lowered the upper esophageal sphincter swallowing pressure to the greatest
and longest extent in healthy individuals. However, in the present study, NF, which was
anticipated to reduce hypopharyngeal residue, was not effective. The addition of HF (CHNF)
showed immediate improvement, indicating that swallowing pressure alone may not be
appropriate to explain this effect.
To the best of our knowledge, there are no previous reports describing hyoid and laryngeal
movement that classifies the chin-down maneuver into HF, NF, and CHNF categories. Leigh et
al. reasoned that the horizontal hyoid movement of healthy subjects was suppressed by a
chin-tuck because the submental muscles were compressed by the mandible, and the submental
muscle was shorter than it was in a neutral position.11) However, the chin-down maneuver did not significantly
affect hyoid movement. In other words, a comfortable chin-down position that does not change
the length of resting SHMs does not affect the hyoid movement in healthy individuals. In the
present study, both NF and CHNF were comfortable, and the length of the GM before
contraction was not significantly different between the two positions.
Based on these findings, we postulated that the impaired extension of IHMs as a result of
fibrosis and scarring was the cause of dysphagia, compensation for which could be
immediately achieved in the present case by the chin-down maneuver. In other words, we
hypothesized that CHNF shortens the DOIs of IHMs, resulting in a relative relaxation of
resting IHMs, thereby immediately compensating for the contraction impairment of SHMs.
Mepani et al. used VF images of the thyrohyoid muscle,12) and Shimizu et al. used echo images of the GM13) for the two-dimensional analysis
of muscle lengths. However, to the best of our knowledge, there are no studies in which
simultaneous two-dimensional analysis of the lengths of SHMs and IHMs was performed from an
integrated perspective. The measurement method in the present study was a two-dimensional
analysis of the muscle length of SHMs and IHMs using lateral VF images; however, extensive
use of this method will require additional studies to determine its reliability.
For CHNF compared with NF, we found that the DOI before the start of anterior hyoid
displacement was similar for the GM but smaller for the SM. Furthermore, MCR and MCD of GM
was higher for CHNF than for NF when swallowing liquid and paste.
In other words, fibrosis and scarring restrict the extension of the SM, which resists GM
contraction. Compensation for this could be achieved by CHNF, which decreases DOI-SM,
thereby improving the contractile function of the GM during swallowing. Although surgical
invasion from cervical drainage and tracheostomy may have contributed to the fibrosis and
scarring, it is likely that the above compensatory mechanism led to appropriate
cricopharyngeal muscle opening and maintenance, thereby reducing residue at the pyriform
sinus.
As described here, a movement disorder of the SHMs during swallowing can develop after DNM
treatment because of extension impairment of the IHMs. The present report is the first to
verify the mechanism by which compensation of this condition can be achieved by CHNF.
The way in which the DOI of IHMs is affected by flexion should be studied for all positions
(HF, NF, and CHNF). We postulate, however, that the compensatory effect may work better in
the chin-down posture with a deeper flexion than with a shallow flexion. The patient in the
present case swallowed meals with CHNF, achieved by voluntarily dropping her head. In
addition, we surmised that the patient swallowed in a head-dropped position without using
the muscles around the neck to avoid contractions of the IHMs during the chin-down posture
and simultaneous contractions of SHMs and IHMs during swallowing, especially since
contraction of the IHMs plays a role in neck flexion.
However, in the present case, the high compensatory effect of CHNF may have been achieved
because of the absence of obvious functional problems such as fibrosis and scarring of the
SHMs. In the future, it will be necessary to examine the effects in a broader range of
conditions, not limited to DNM, such as in inflammatory diseases or surgical procedures that
may result in fibrosis, scarring, or shortening of the IHMs, as well as hypertonia of these
muscles.
CONCLUSION
Dysphagia after DNM was successfully treated in this case with the chin-down procedure. The
lengths of the SHMs and IHMs were analyzed in two dimensions using VFSS images to assess
whether the compensation achieved by the chin-down maneuver is consistent with the
previously-suggested hyoid and laryngeal movement disorder being caused by fibrosis and
scarring. The present patient may have developed restrictions in extension of the SM, which
applies resistance to GM contraction, and compensation for this condition was achieved by
CHNF through the decreased DOI of the SM, thereby improving the contractile function of the
GM.
ACKNOWLEDGMENTS
The authors would like to thank Mr. Yukio Morohoshi, Radiological Technologist of Tokai
University Oiso Hospital, for providing comments on our data. Furthermore, the authors would
like to thank Ms. Emi Tada, Speech Language Pathologist of Tokai University Hospital, for
providing detailed patient information.
CONFLICTS OF INTEREST
No conflicts of interest have been reported by the authors or by any individuals in
control of the content of this study.
REFERENCES
- 1. Sarna T, Sengupta T, Miloro M, Kolokythas A:
Cervical necrotizing fasciitis with descending mediastinitis: literature review and case
report. J Oral Maxillofac Surg 2012;70:1342–1350. PMID:21820786,
DOI:10.1016/j.joms.2011.05.007
- 2. Sumi Y: Descending necrotizing mediastinitis: 5
years of published data in Japan. Acute Med Surg 2015;2:1–12. PMID:29123684,
DOI:10.1002/ams2.56
- 3. Glen P, Morrison J: Diffuse descending
necrotising mediastinitis and pleural empyema secondary to acute odontogenic infection
resulting in severe dysphagia. BMJ Case Rep 2016;2016:bcr2015212145. PMID:27013653,
DOI:10.1136/bcr-2015-212145
- 4. Hidaka H, Ozawa D, Kuriyama S, Obara T, Nakano T,
Kakuta R, Nomura K, Watanabe K, Katori Y: Risk factors for delayed oral dietary intake in
patients with deep neck infections including descending necrotizing mediastinitis. Eur
Arch Otorhinolaryngol 2017;274:3951–3958. PMID:28825131,
DOI:10.1007/s00405-017-4716-3
- 5. Ito H, Kato T: A case of dysphagia after the
operation of descending necrotizing mediastinitis [in Japanese]. Nihon Kikan Shokudoka
Gakkai Kaiho 2005;56:495–500. DOI:10.2468/jbes.56.495
- 6. Crary MA, Mann GD, Groher ME: Initial
psychometric assessment of a functional oral intake scale for dysphagia in stroke
patients. Arch Phys Med Rehabil 2005;86:1516–1520. PMID:16084801,
DOI:10.1016/j.apmr.2004.11.049
- 7. Pearson WG, Jr, Langmore SE, Zumwalt AC:
Evaluating the structural properties of suprahyoid muscles and their potential for moving
the hyoid. Dysphagia 2011;26:345–351. PMID:21069388,
DOI:10.1007/s00455-010-9315-z
- 8. Logemann JA: Evaluation and treatment of
swallowing disorders. Pro-Ed, Austin, 1998;197–201.
- 9. Okada S, Saitoh E, Palmer JB, Matsuo K, Yokoyama
M, Shigeta R, Baba M: What is the chin-down posture? A questionnaire survey of speech
language pathologists in Japan and the United States. Dysphagia 2007;22:204–209.
PMID:17436041, DOI:10.1007/s00455-006-9073-0
- 10. Matsubara K, Kumai Y, Kamenosono Y, Samejima Y,
Yumoto E: Effect of three different chin-down maneuvers on swallowing pressure in healthy
young adults. Laryngoscope 2016;126:437–441. PMID:26266665,
DOI:10.1002/lary.25552
- 11. Leigh JH, Oh BM, Seo HG, Lee GJ, Min Y, Kim K,
Lee JC, Han TR: Influence of the chin-down and chin-tuck maneuver on the swallowing
kinematics of healthy adults. Dysphagia 2015;30:89–98. PMID:25358491,
DOI:10.1007/s00455-014-9580-3
- 12. Mepani R, Antonik S, Massey B, Kern M, Logemann
J, Pauloski B, Rademaker A, Easterling C, Shaker R: Augmentation of deglutitive thyrohyoid
muscle shortening by the Shaker Exercise. Dysphagia 2009;24:26–31. PMID:18685891,
DOI:10.1007/s00455-008-9167-y
- 13. Shimizu S, Hanayama K, Metani H,Sugiyama TT , Abe
HH , Seki SS , Hiraoka TT , Tsubahara , Tsubahara A. Jpn J Compr Rehabil Sci
2016;7:55–60.
Appendices
APPENDIX: FOIS ITEMS6)
Level 1: Nothing by mouth.
Level 2: Tube dependent with minimal attempts at food or
liquid.
Level 3: Tube dependent with consistent oral intake of food
or liquid.
Level 4: Total oral diet of a single consistency.
Level 5: Total oral diet with multiple consistencies, but
requiring special preparation or compensations.
Level 6: Total oral diet with multiple consistencies without
special preparation, but with specific food limitation