ABSTRACT
Objectives: The aim of this study was to translate the Cumulated Ambulation
Score (CAS) from English into Japanese in cooperation with different types of healthcare
providers and to investigate its inter-rater reliability and internal consistency.
Methods: Two physical therapists at each of three general hospitals in Japan
measured the mobility of 50 consecutive post-operative hip fracture patients on two
occasions between 2 and 6 days after surgery using the Japanese version of the CAS
(CAS-JP). We analyzed the inter-rater reliability and agreement using both the linear
weighted kappa and the interclass correlation coefficient; we also analyzed the internal
consistency using Cronbach’s alpha coefficient.
Results: The mean age of patients was 81 (SD: 11.6) years and 82% were
women. Approximately half of the patients had severe cognitive impairment. Kappa was ≥
0.93 for the three mobility activities and for the total CAS-JP score, the percentage
agreement was ≥ 0.98, the ICC was ≥ 0.95, and Cronbach’s alpha coefficient was 0.85.
Conclusions: We found that the CAS-JP possessed good inter-rater
reliability, agreement, and internal consistency. The CAS-JP is a reliable and easy-to-use
evaluation tool suitable for daily clinical practice across different healthcare providers
to monitor mobility in older hip fracture patients in Japan. We suggest that CAS-JP be
evaluated in future studies for use in younger patients and in other patient groups with
mobility problems.
INTRODUCTION
Post-operative hip fracture patients experience a loss of mobility.1,2) To reduce morbidity, mortality, and improve physical
function, early mobilization and rehabilitation after surgery is recommended.3) Because a large majority of patients
who undergo hip fracture surgery are elderly and less physically active in general,
healthcare providers need valid and reliable measurement methods to monitor the level and
improvement of mobility of individual patients. Not only patients with hip
fracture,4,5,6,7) but also geriatric patients,8,9) patients with community-acquired pneumonia,10) and patients who undergo acute
high-risk abdominal surgery or knee-arthroplasty experience different levels of in-hospital
mobility problems.11,12) Therefore, by monitoring the early
mobility function after admission or surgery, healthcare providers will be able to better
plan and optimize patient care.
The Cumulated Ambulation Score (CAS) is a valid and reliable evaluation tool for assessing
a patient’s mobility by observing three basic activities3): (1) getting in and out of bed, (2) sitting and rising from
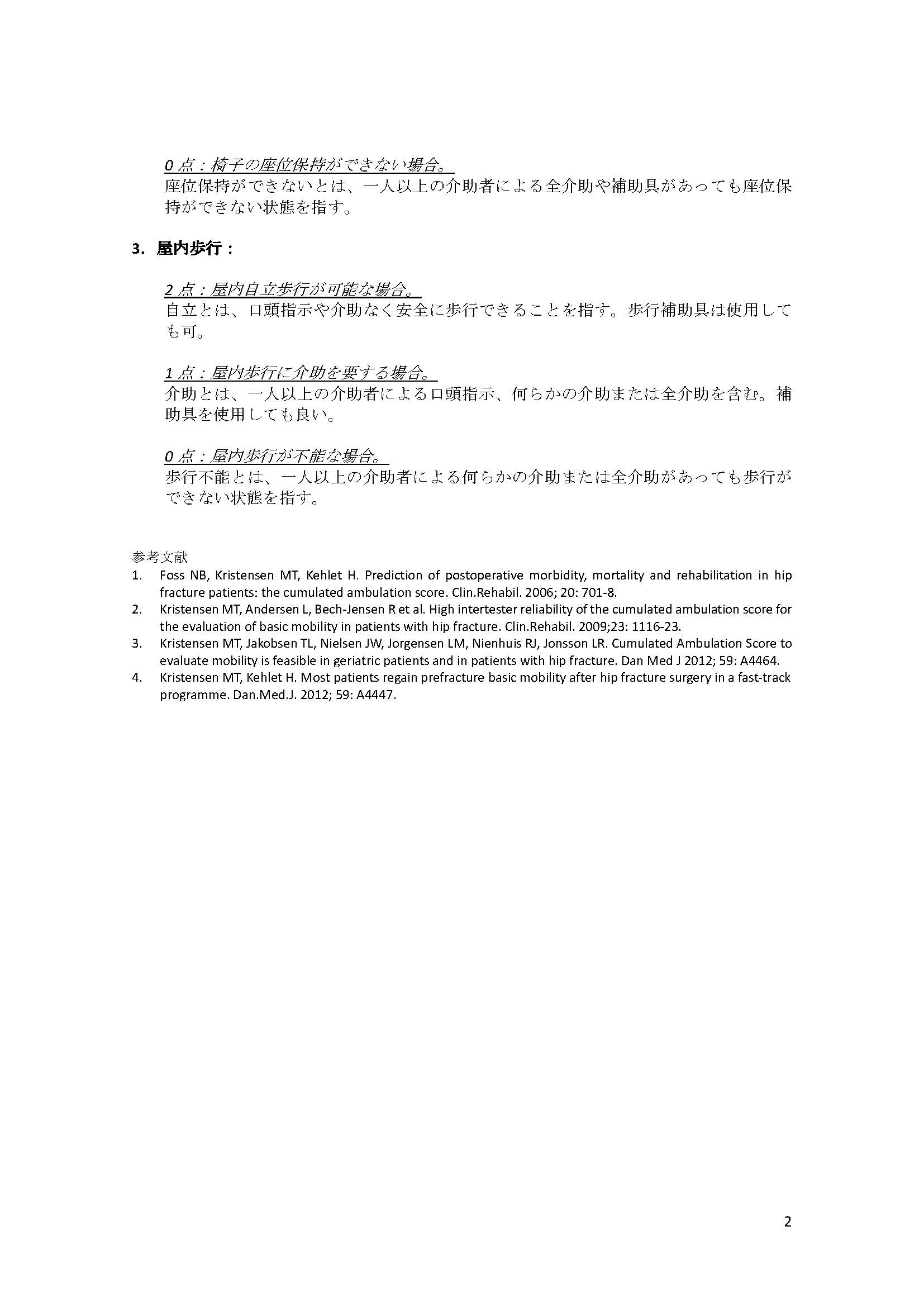
a chair (with armrests), and (3) indoor walking (with or without a walking aid).13) Each of these three CAS activities
is scored from 0 (unable to perform) to 1 (assistance required) to 2 (independent) and the
scores are summed to provide a one-day total CAS score of 0–6 points, with 6 points
indicating an independent ambulatory status.13) The CAS is routinely used in other countries for patients
with hip fracture,3,4,5) for those undergoing joint replacement,14,15) and for other elderly health disorders.11) CAS scores cumulated for
postoperative days 1–3 (3-day CAS) has proven valid as a prediction of the short-term
clinical outcome of patients after hip fracture surgery.3) Moreover, the CAS shows a lower floor effect than the de
Morton Mobility Index and the Chair Stand Test for physically frail populations, such as
patients with hip fracture.16)
Therefore, the CAS can be used to monitor the trajectory of a patient’s mobility function,
especially in the crucial early stage after hip fracture surgery.
The CAS was developed in Denmark; it was subsequently translated into several languages
including English, Italian, Spanish, and Turkish and is now used in many
countries.17,18,19) Approved versions are also available in Swedish,
Norwegian, Indonesian-Bahasa, and French, and the CAS is used at the national level in the
Danish and Irish multidisciplinary hip fracture database. In Japan, the mean age of patients
with hip fracture has been increasing, as has also been seen in other countries.20,21) Furthermore, the life expectancy of people in
Japan is one of the highest worldwide. Consequently, healthcare providers in Japan need
valid and reliable measurements to monitor and guide the rehabilitation needs of the aged
population.
The CAS already has been used in Japan and has proven to be valid in reflecting the
association of surgery within 24 h of hospital admission and the ambulatory status after hip
fracture surgery.4) However,
although the CAS used in that study was in Japanese and was based on the first English
version of the CAS,3) that
Japanese version was not translated according to international guidelines. Consequently,
there is a need for an official Japanese version of the CAS. By translation and
cross-cultural validation of the CAS into an official Japanese version, the CAS can be used
in Japan as an easily applicable measurement of patients with basic mobility problems,
thereby further promoting use of the CAS as an international multidisciplinary outcome
measurement. The aim of this study was to translate and cross-culturally validate the
English version of the CAS into Japanese and to investigate the inter-rater reliability,
agreement, and internal consistency of the Japanese version of the CAS (CAS-JP).
METHODS
Translation Process
We followed the recommendations of Ramada-Rodilla et al.22) to translate the English version of the CAS
manual and score-sheet into Japanese.23) Two Japanese physical therapists, one who is fluent in
English (HH) and one who uses English in daily clinical practice in the U.S. (FI),
independently translated the English version of the CAS manual and score-sheet into
Japanese, taking the Japanese culture and language into consideration while maintaining
the original intention of the test. A CAS-JP committee synthesized these two Japanese
translations of CAS. A back translation of the synthesized version was conducted by a
third person (JM) who is a native speaker of American English, holds a U.S. nursing
license, and has experience in U.S. hospital wards, without knowledge of the original
version of the CAS. This back translated English version was forwarded to Dr. Kristensen,
who is one of the original developers of CAS, to ensure that the core concepts of the
score remained intact.3,13) We subsequently modified the Japanese CAS with some word
corrections to retain the original CAS scoring procedure. Two physical therapists from
each institution conducted pilot measurements with the provisional Japanese CAS; one of
these physical therapists communicated with Dr. Kristensen, and the other was a novice CAS
user. First, these two raters preliminarily measured CAS-JP to confirm all measurements.
If additional comments were presented during this process, they were shared and described
on the CAS-JP score manual with Dr. Kristensen’s agreement. Once the modification process
was complete, the final version of the Japanese CAS (CAS-JP) was approved by CAS-JP
committee members. CAS-JP is available as a supplement (Appendix 1).
The Cumulated Ambulation Scores
The CAS is a composite measurement that consists of the following three basic mobility
activities: (i) getting in and out of bed with the sequence of events as follows: the
patient starts in the supine position on the bed, moves to sitting, stands or transfers to
a chair next to the bed, then returns to sitting on the bed, and then to the supine
position on the bed (with or without assistance or aids); (ii) sit to stand to sit from a
chair with armrests (with or without assistance or aids), and (iii) walking indoors (with
or without walking aids).13,23) These three basic activities are each allocated 0–2 points
and the three scores are combined for a total one-day CAS score ranging from 0 (minimum)
to the maximum of 6 points. A CAS score of 0 indicates total dependence, whereas 6 points
indicates complete independence in mobility activities. A score of 2 was given to patients
who could perform the activity without verbal or physical assistance, a score of 1 was
given to those who required verbal or physical assistance by one or more persons, and a
score of 0 was given for patients who were unable to do the activity despite human
assistance.13,23)
Study Population
A total of 50 consecutive hip fracture patients who underwent reparative surgery and were
admitted between January and June 2020 to three general hospitals (one urban, one
suburban, and one rural hospital: 18, 12, and 20 patients, respectively) in Japan were
analyzed. We included patients with hip fracture (trochanteric fracture or femoral neck
fracture) aged 65 years and older. Patients with multiple trauma, loss of consciousness,
or immobility before injury were excluded. The following descriptive information was
extracted from each patient’s medical chart: weight, height, type of fracture, and type of
surgery. Additionally, the following baseline demographics were evaluated at hospital
admission: age, sex, body mass index (BMI), walking ability before injury, walking aid use
before injury, the affected side, the type of fracture, the surgical procedure, and the
results of the Pfeiffer short portable mental state questionnaire (SPMSQ, 0–10
points24)). The patient’s
walking ability and walking aid use was obtained from the patient or from the patient’s
family if the patient had cognitive impairment. Walking ability was then classified into
one of four categories: able to walk outside for 15 min or more, able to walk outside for
less than 15 min, able to walk only inside, or unable to walk. Walking aid was categorized
as: no aid use, use of a cane or walker outside only, or use of a cane or walker both
inside and outside. The fracture type was assessed as a femoral neck fracture or a
trochanteric fracture according to the fracture site. The surgical procedure was
categorized as open reduction with internal fixation or hemiarthroplasty. With respect to
cognitive function, we assessed the SPMSQ score between 7 and 14 days post-surgery to
avoid possible acute delirium that would have influenced the evaluation. SPMSQ scores were
categorized as follows: 0–2 points as no cognitive impairment, 3–4 points as mild
cognitive impairment, 5–7 points as moderate cognitive impairment, and >8 points as
severe cognitive impairment.13,23,24)
Inter-rater Reliability
Inter-rater reliability for the CAS-JP was evaluated according to the Guidelines for
Reporting Reliability and Agreement.25) The inter-rater reliability of the CAS-JP was assessed
between two physical therapy raters at each of the three general hospitals (six physical
therapists in total); each therapist did the first measurement of half of the consecutive
hip fracture patients who had undergone surgery at their respective hospital. The first
assessment of each patient by a rater from physical therapist group A was made as part of
clinical practice before rehabilitation within postoperative days 2–6 and was followed by
assessment by the other rater (physical therapist group B) on the same day. To reduce
possible bias resulting from fluctuations in patients’ daily mobility function, the second
rater measured the same patient 2 h after the first rater; the raters performed the
measurements independently. No discussion of the ratings was allowed until the end of the
study.26) Two days after
the first assessment, all patients were evaluated again using the same procedure.
Consequently, each patient was evaluated twice by each rater, which sums to a total of 200
CAS assessments conducted by the six raters. Therefore, reliability estimates were based
on comparison of 100 CAS evaluations by rater group A and 100 by rater group B. If the
planned day of assessment was a national holiday or an out-of-service day, the measurement
day was adjusted accordingly.
Statistical Analysis
Continuous variables are presented as means with standard deviations (SDs) or as medians
with interquartile ranges according to their distributions; categorical variables are
described as numbers with percentages. We estimated linear weighted kappa values to assess
the inter-rater reliability for the three mobility activities and the total CAS-JP
score.27) A kappa value
less than 0.2 was considered as slight agreement, between 0.21 and 0.40 as fair agreement,
between 0.41 and 0.60 as moderate agreement, between 0.61 and 0.80 as substantial
agreement, and more than 0.80 as almost perfect agreement.28) The percentage agreement between the two raters
and the prevalence of CAS-JP scores for the three mobility activities and the total CAS-JP
scores were described. To evaluate the measurement error for the three mobility activities
and the total CAS-JP score, we also calculated the interclass correlation coefficient
(ICC) with a two-way mixed model based on consistency measurement.29) The ICC ranges from 0 to 1, and
cut off values were assessed as follows: poor agreement for ICC lower than 0.40, fair
agreement for ICC ranging from 0.40 to 0.59, good agreement for ICC ranging from 0.60 and
0.74, and excellent agreement for more than 0.75.30) ICC values were used to calculate the standard error of
measurement [SEM=SD × √(1-ICC)] and the smallest real difference (SRD=SEM × √2 × 1.96) to
allow comparison of the measurement error with previous original CAS research performed in
English.13,27,31) The score differentiation between the two raters
was also visualized using a Bland-Altman plot. To test for internal consistency,
Cronbach’s alpha coefficient was estimated.32) Cronbach’s alpha coefficient ranges from 0 to 1, and values
lower than 0.70 were regarded as unacceptable, values between 0.70 and 0.80 as acceptable,
and values higher than 0.80 as good.33,34) The sample size was calculated according to the criteria of
Nunnally and Hoskins et al. A total of 45 to 50 study patients were planned.35,36) Written informed consent was obtained from
patients or their relatives. Study approval was obtained from the institutional review
board (E19HS-010, 19-R097). The type I error probability was set to 0.05 for all analyses.
All statistical analyses were performed using Stata version 16.1 (Stata Corp, College
Station, TX, USA).
RESULTS
During the translation process, there were two major considerations: one was the difference
of language use and the other was the discrepancy in bedside settings across hospitals.
First, when we translated the original English version of CAS into Japanese (CAS-JP), the
phrase “get in/out of bed” was freely translated into Japanese, resulting in the implication
of different mobility actions. Therefore, we prioritized the original meaning rather than
the technical term used in the physical therapeutic field, rishou, which
mainly means getting out of bed but does not include getting into bed. The second
challenging point was the concept of independence when it comes to putting on footwear.
Different hospitals used different types of footwear, such as slippers or shoes. The
original version of the CAS did not include any variance in footwear such as room shoes or
slippers for the measurement of independence. Therefore, to maintain consistency across
hospitals, we did not include putting on footwear in evaluating independence and added this
point to the manual.
A total of 50 consecutive hip fracture patients were evaluated twice (with an interval of 2
h) on two separate occasions (200 measurements in total) using the CAS-JP. Evaluations were
carried out by six physical therapists independently in three general hospitals in Japan
(Table 1). All patients were evaluated between
2 and 10 days post-surgery.
Table 1.
Patient demographics (n=50) and observed scores of the Japanese version of the
Cumulated Ambulation Score
|
Total (N=50) |
| Age (years) |
80.68 (11.55) |
| Sex |
|
| Female |
41 (82) |
| Male |
9 (18) |
| Body mass index (kg/m2) |
20.44 (3.19) |
| Pre-fracture walking ability |
|
| Able to walk outside for 15 min or more |
20 (40) |
| Able to walk outside less than 15 min |
11 (22) |
| Able to walk inside only |
19 (38) |
| Unable to walk |
0 (0) |
| Pre-fracture use of walking aid |
|
| No use |
18 (36) |
| Use only outside (cane or walker) |
19 (38) |
| Use both inside and outside (cane or walker) |
13 (26) |
| Fracture side |
|
| Right |
23 (46) |
| Left |
27 (54) |
| Fracture type |
|
| Femoral neck |
34 (68) |
| Trochanteric |
16 (32) |
| Surgical procedure |
|
| Open reduction with internal fixation |
25 (50) |
| Hemiarthroplasty |
25 (50) |
| Short portable mental state questionnaire |
|
| No cognitive impairment |
6 (12) |
| Mild cognitive impairment |
6 (12) |
| Moderate cognitive impairment |
11 (22) |
| Severe cognitive impairment |
27 (54) |
| Cumulated Ambulation Score (CAS) |
|
| Getting in and out of bed (0–2) |
1.10 (0.48) |
| Sit-to-stand-to-sit from chair with armrests (0–2) |
1.30 (0.56) |
| Walking indoors with or without an aid (0–2) |
0.63 (0.72) |
| Total one-day CAS (0–6) |
3.02 (1.50) |
Values are given as the number of patients with the percentage of the cohort in
parentheses, with the exception of age, body mass index (BMI), short portable mental
state questionnaire (SPMSQ), and cumulated ambulation score (CAS) which are given as the
mean and standard deviation. The total number of CAS observations was 200 because
measurement by raters from groups A and B were taken on two occasions.
The mean age of patients was 81 (SD, 11.6) years and the majority were women (n=41, 82%).
In terms of the pre-fracture mobility, 62% of patients were able to walk outside before
injury, and more than a two-thirds of patients either required no use of a walking aid or
use of a walking aid outside only. With respect to hip fracture, 68% of patients had femoral
neck fracture and half of the patients underwent hemiarthroplasty. Approximately half of the
patients had severe cognitive impairment (Table
1).
Tables 2 and 3 show the results for inter-rater reliability. The weighted
kappa for the three mobility activities (getting in and out of bed, sit-to-stand-to-sit from
an armchair, walking indoors with or without an aid) and the total CAS-JP were excellent
(0.96, 0.93, 0.97, and 0.97, respectively). The corresponding percentage agreement also was
excellent (≥98%) (Table 2).
Table 2.
Inter-rater reliability and agreement of the Japanese version of the Cumulated
Ambulation Score between scores taken by two different physical therapists (1)
| Activity |
Linear weighted
Kappa value
(95%CI) |
Observed
agreement, n (%) |
CAS score 0 to 2, n (%) |
| 0 |
1 |
2 |
| Getting in and out of bed (0–2) |
0.96 (0.81–1.0) |
99 (99) |
15 (7.5) |
144 (72.0) |
41 (20.5) |
Sit-to-stand-to-sit from chair with
armrests
(0–2) |
0.93 (0.77 − 1.0) |
98 (98) |
12 (6.0) |
114 (57.0) |
74 (37.0) |
| Walking indoors with or without an aid (0–2) |
0.97 (0.82 − 1.0) |
99 (99) |
102 (51.0) |
68 (34.0) |
30 (15.0) |
| Total CAS (0–6) |
0.97 (0.84 − 1.0) |
99 (99) |
n/a |
n/a |
n/a |
CI, confidence interval.
The ICC showed an excellent result (≥0.94) for the three mobility activities and the
one-day CAS-JP (Table
3). The SEM and the SRD for the one-day CAS-JP were 0.17 and 0.47. The
largest difference in scores between the two raters was 1 point, and the Bland-Altman plot
indicated that there was no systematic between-rater bias over the three mobility activities
or for the total CAS-JP scores (Figure 1).
Cronbach’s alpha coefficient for the CAS-JP was 0.85.
Table 3.
Inter-rater reliability and agreement of the Japanese version of the Cumulated
Ambulation Score between scores taken by two different physical therapists (2)
| Activity |
ICC (95%CI) |
SEM |
SRD |
| Getting in and out of bed (0–2) |
0.96 (0.95–0.97) |
0.10 |
0.28 |
| Sit-to-stand-to-sit from chair with armrests (0–2) |
0.94 (0.92–0.96) |
0.14 |
0.39 |
| Walking indoors with or without an aid (0–2) |
0.98 (0.97–0.99) |
0.10 |
0.28 |
| Total CAS (0–6) |
0.99 (0.98–0.99) |
0.17 |
0.47 |
ICC, intraclass correlation coefficients; SEM, standard error of measurement; SRD,
smallest real difference.
DISCUSSION
In this study, the English version of the CAS was translated and cross-culturally validated
into Japanese based on the guideline used in previous research in which the CAS was
translated.22) CAS-JP
showed excellent inter-rater reliability, high agreement, and excellent internal consistency
in our research patients. In our analysis, a total of 50 patients were enrolled and 200
measurements in total were carried out by the two physical therapist rater groups (groups A
and B). The patients were evaluated in three hospitals located in urban (Tokyo), suburban
(Saitama), and rural (Nagano) areas. The baseline characteristics of our data represent the
general hip fracture population in Japan.21)
As the age of patients with hip fracture increases in Japan along with the aging of the
population, CAS-JP as applied to the hip fracture population can contribute to geriatric
clinical research. Also, because life expectancy and the incidence of hip fracture are
increasing around the world, the results of clinical research on patients with hip fracture
in Japan can contribute to health care in other countries where there are predictions of a
future increase in the number of hip fractures. Although our patients were slightly older
than those in previous studies in Denmark, Spain, and Turkey, the reliability and
consistency of the translated CAS-JP were consistent with previous studies.17,18,19)
Because the CAS can be used with high reliability by different healthcare providers,
including physical therapists, occupational therapists, and physicians,13,17,18,19) we also included a nurse in the translation process to expand
knowledge of the CAS across healthcare providers. The use of the CAS to monitor the progress
of early recovery after hip fracture surgery and of other patient groups by different
healthcare providers has been demonstrated. There is scope for further application of the
CAS to a wider range of age groups with or without comorbidities across a broad range of
countries.
Strength and Limitations
One strength of this study is that the excellent reliability estimates were based on
evaluations by six physical therapists: two at each of the three hospitals forming rater
groups A and B. Nonetheless, our research also had some limitations. First, we did not
externally validate the CAS-JP, although the original version of the CAS was validated in
previous studies.16,18) Therefore, further study is needed to confirm the validity
of the CAS-JP and to compare results with previous studies. Second, our study was
restricted to general hospitals in Japan, although we achieved some diversification by
selecting study sites in urban, suburban, and rural hospitals. Even so, these study sites
may not represent all hospital settings across Japan. Finally, the number of patients with
a CAS score of 0 was relatively small, whereas patients with a CAS score of 1 or 2 were
sufficiently covered. Our data collection started from post-operative day 2, which
explains the low number of patients with a CAS score of 0. However, a CAS score of 0,
which means the inability to perform any mobility activity (e.g., a completely bedridden
patient), should be relatively easy to evaluate and we assumed it to be reasonable to draw
conclusions without a larger number of patients with a CAS score of 0.
We translated the original English version of the CAS into Japanese and demonstrated its
excellent inter-rater reliability and consistency based on robust methods. The CAS is
reliable and easy to use in daily clinical practice to monitor mobility by different
healthcare providers. We therefore suggest that the CAS-JP be measured broadly for older
patients with hip fracture in Japan and that it be evaluated throughout hospitals in Japan
for use in younger patients and in other patient groups with mobility problems.
ACKNOWLEDGMENTS
We thank Yasuhiro Yamamoto, Junya Kubo, and Yuya Nagasawa for help with participant
recruitment and the measurement of the CAS-JP. We also thank Fumiaki Isshiki for help with
the translation process of the CAS-JP.
CONFLICTS OF INTEREST
The authors declare that there are no conflicts of interest.
APPENDIX

APPENDIX 1

APPENDIX 2
APPENDIX 2
REFERENCE
- 1. Ariza-Vega P, Jiménez-Moleón JJ, Kristensen MT:
Change of residence and functional status within three months and one year following hip
fracture surgery. Disabil Rehabil 2014;36:685–690. PMID:23919643,
DOI:10.3109/09638288.2013.813081
- 2. Bower ES, Wetherell JL, Petkus AJ, Rawson KS,
Lenze EJ: Fear of falling after hip fracture: prevalence, course, and relationship with
one-year functional recovery. Am J Geriatr Psychiatry 2016;24:1228–1236. PMID:27726939,
DOI:10.1016/j.jagp.2016.08.006
- 3. Foss NB, Kristensen MT, Kehlet H: Prediction of
postoperative morbidity, mortality and rehabilitation in hip fracture patients: the
cumulated ambulation score. Clin Rehabil 2006;20:701–708. PMID:16944827,
DOI:10.1191/0269215506cre987oa
- 4. Ogawa T, Aoki T, Shirasawa S: Effect of hip
fracture surgery within 24 hours on short-term mobility. J Orthop Sci 2019;24:469–473.
PMID:30502228, DOI:10.1016/j.jos.2018.11.001
- 5. Kristensen MT, Öztürk B, Röck ND, Ingeman A, Palm
H, Pedersen AB: Regaining pre-fracture basic mobility status after hip fracture and
association with post-discharge mortality and readmission – a nationwide register study in
Denmark. Age Ageing 2019;48:278–284. PMID:30615060,
DOI:10.1093/ageing/afy185
- 6. Fitzgerald M, Blake C, Askin D, Quinlan J,
Coughlan T, Cunningham C: Mobility one week after a hip fracture – can it be predicted?
Int J Orthop Trauma Nurs 2018;29:3–9. PMID:29602677,
DOI:10.1016/j.ijotn.2017.11.001
- 7. Hulsbæk S, Larsen RF, Troelsen A: Predictors of
not regaining basic mobility after hip fracture surgery. Disabil Rehabil
2015;37:1739–1744. PMID:25350664, DOI:10.3109/09638288.2014.974836
- 8. Aagesen M, Kristensen MT, Vinther A: The
cumulated ambulation score is superior to the new mobility score and the de Morton
Mobility Index in predicting discharge destination of patients admitted to an acute
geriatric ward; a 1-year cohort study of 491 patients. Disabil Rehabil 2020;1–8.
PMID:32757865, DOI:10.1080/09638288.2020.1802522
- 9. Kristensen MT, Jakobsen TL, Nielsen JW, Jørgensen
LM, Nienhuis RJ, Jønsson LR: Cumulated Ambulation Score to evaluate mobility is feasible
in geriatric patients and in patients with hip fracture. Dan Med J
2012;59:A4464.
- 10. Melgaard D, Baandrup U, Bøgsted M, Bendtsen MD,
Kristensen MT: Early mobilisation of patients with community-acquired pneumonia reduce
length of hospitalisation – a pilot study. J Phys Ther Sci 2018;30:926–932. PMID:30034100,
DOI:10.1589/jpts.30.926
- 11. Jønsson LR, Ingelsrud LH, Tengberg LT, Bandholm
T, Foss NB, Kristensen MT: Physical performance following acute high-risk abdominal
surgery: a prospective cohort study. Can J Surg 2018;61:42–49. PMID:29368676,
DOI:10.1503/cjs.012616
- 12. Gkagkalis G, Pereira LC, Fleury N, Luthi F,
Lécureux E, Jolles BM: Are the Cumulated Ambulation Score and Risk Assessment and
Prediction Tool useful for predicting discharge destination and length of stay following
total knee arthroplasty? Eur J Phys Rehabil Med 2019;55:816–823.
- 13. Kristensen MT, Andersen L, Bech-Jensen R, Moos M,
Hovmand B, Ekdahl C, Kehlet H: High intertester reliability of the Cumulated Ambulation
Score for the evaluation of basic mobility in patients with hip fracture. Clin Rehabil
2009;23:1116–1123. PMID:19923208, DOI:10.1177/0269215509342330
- 14. Andersen KV, Bak M, Christensen BV, Harazuk J,
Pedersen NA, Søballe K: A randomized, controlled trial comparing local infiltration
analgesia with epidural infusion for total knee arthroplasty. Acta Orthop 2010;81:606–610.
PMID:20860447, DOI:10.3109/17453674.2010.519165
- 15. Holm B, Kristensen MT, Myhrmann L, Husted H,
Andersen LØ, Kristensen B, Kehlet H: The role of pain for early rehabilitation in fast
track total knee arthroplasty. Disabil Rehabil 2010;32:300–306. PMID:20055568,
DOI:10.3109/09638280903095965
- 16. Hulsbæk S, Larsen RF, Rosthøj S, Kristensen MT:
The Barthel Index and the Cumulated Ambulation Score are superior to the de Morton
Mobility Index for the early assessment of outcome in patients with a hip fracture
admitted to an acute geriatric ward. Disabil Rehabil 2019;41:1351–1359. PMID:29334273,
DOI:10.1080/09638288.2018.1424951
- 17. Ariza-Vega P, Mora-Traverso M, Ortiz-Piña M, Ashe
MC, Kristensen MT: Translation, inter-rater reliability, agreement, and internal
consistency of the Spanish version of the cumulated ambulation score in patients after hip
fracture. Disabil Rehabil 2019;1–6. PMID:30907173,
DOI:10.1080/09638288.2019.1577499
- 18. Çolak İ, Mete E, Kristensen MT, Kuru Çolak T:
Translation, reliability, agreement and validity of the Turkish version of Cumulated
Ambulation Score in patients with hip fracture. Eklem Hastalik Cerrahisi 2020;31:346–352.
PMID:32584736, DOI:10.5606/ehc.2020.75526
- 19. Grana E, Verzellotti S, Grassi FA, Ferriero G,
Kristensen MT, Cisari C, Invernizzi M: Cross-cultural validation of the Italian version of
the Cumulated Ambulation Score. Int J Rehabil Res 2016;39:160–164. PMID:27028288,
DOI:10.1097/MRR.0000000000000165
- 20. Brauer CA, Coca-Perraillon M, Cutler DM, Rosen
AB: Incidence and mortality of hip fractures in the United States. JAMA
2009;302:1573–1579. PMID:19826027, DOI:10.1001/jama.2009.1462
- 21. Hagino H, Endo N, Harada A, Iwamoto J, Mashiba T,
Mori S, Ohtori S, Sakai A, Takada J, Yamamoto T: Survey of hip fractures in Japan: recent
trends in prevalence and treatment. J Orthop Sci 2017;22:909–914. PMID:28728988,
DOI:10.1016/j.jos.2017.06.003
- 22. Ramada-Rodilla JM, Serra-Pujadas C,
Delclós-Clanchet GL: [Cross-cultural adaptation and health questionnaires validation:
revision and methodological recommendations]. Salud Publica Mex 2013;55:57–66.
PMID:23370259, DOI:10.1590/S0036-36342013000100009
- 23.Kristensen MT, Curtis DJ: Cumulated Ambulation
Score (CAS), English version, manual and score-sheet. 2015.
https://www.researchgate.net/publication/270888051_Cumulated_Ambulation_Score_CAS_English_version_manual_and_score-sheet. Accessed 30 Nov 2020.
- 24. Pfeiffer E: A short portable mental status
questionnaire for the assessment of organic brain deficit in elderly patients. J Am
Geriatr Soc 1975;23:433–441. PMID:1159263,
DOI:10.1111/j.1532-5415.1975.tb00927.x
- 25. Kottner J, Audigé L, Brorson S, Donner A,
Gajewski BJ, Hróbjartsson A, Roberts C, Shoukri M, Streiner DL: Guidelines for reporting
reliability and agreement studies (GRRAS) were proposed. Int J Nurs Stud 2011;48:661–671.
PMID:21514934, DOI:10.1016/j.ijnurstu.2011.01.016
- 26. Kristensen MT, Nielsen AØ, Topp UM,
Holmehave-Brandt J, Petterson CF, Gebuhr P: Development and psychometric properties of the
Basic Amputee Mobility Score for use in patients with a major lower extremity amputation.
Geriatr Gerontol Int 2018;18:138–145. PMID:28858422,
DOI:10.1111/ggi.13156
- 27. Weir JP: Quantifying test-retest reliability
using the intraclass correlation coefficient and the SEM. J Strength Cond Res
2005;19:231–240.
- 28.Landis JR, Koch GG. The measurement of
observer agreement for categorical data. biometrics. Biometrics 1977;33:159–174. ,
DOI:10.2307/2529310
- 29. Farhi D, Falissard B, Dupuy A: Global assessment
of psoriasis severity and change from photographs: a valid and consistent method. J Invest
Dermatol 2008;128:2198–2203. PMID:18418412, DOI:10.1038/jid.2008.68
- 30. Cicchetti DV: Guidelines, criteria, and rules of
thumb for evaluating normed and standardized assessment instruments in psychology. Psychol
Assess 1994;6:284–290. DOI:10.1037/1040-3590.6.4.284
- 31. Beckerman H, Roebroeck ME, Lankhorst GJ, Becher
JG, Bezemer PD, Verbeek AL: Smallest real difference, a link between reproducibility and
responsiveness. Qual Life Res 2001;10:571–578. PMID:11822790,
DOI:10.1023/A:1013138911638
- 32. Bland JM, Altman DG: Statistics notes: Cronbach’s
alpha. BMJ 1997;314:572. PMID:9055718, DOI:10.1136/bmj.314.7080.572
- 33. Tavakol M, Dennick R: Making sense of Cronbach’s
alpha. Int J Med Educ 2011;2:53–55. PMID:28029643,
DOI:10.5116/ijme.4dfb.8dfd
- 34. Streiner DL: Starting at the beginning: an
introduction to coefficient alpha and internal consistency. J Pers Assess 2003;80:99–103.
PMID:12584072, DOI:10.1207/S15327752JPA8001_18
- 35. Nunnally JC: Psychometric Theory, 2nd edn.
McGraw-Hill, New York, 1978.
- 36. Hopkins WG: Measures of reliability in sports
medicine and science. Sports Med 2000;30:1–15. PMID:10907753,
DOI:10.2165/00007256-200030010-00001
