ABSTRACT
Objective: The aim of this study was to demonstrate the non-inferiority of
S-flurbiprofen plaster (SFPP) monotherapy for treating knee osteoarthritis compared with
the combination of conventional oral and topical non-steroidal anti-inflammatory drugs
(NSAIDs).
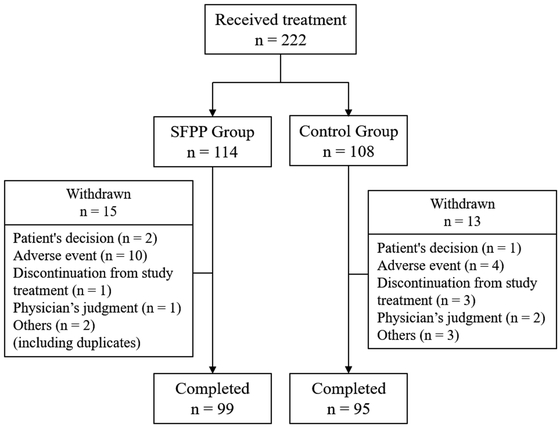
Methods: A total of 222 participants (114, SFPP group; 108, control group)
were treated for 4 weeks. The primary endpoint was the change in the degree of pain felt
while rising from a chair after 2 and 4 weeks of treatment as determined using the visual
analog scale (VAS) . The secondary endpoint was the change in functional scores and test
results. Safety was evaluated in terms of the adverse effects.
Results: The VAS score significantly decreased in both groups after 2 and 4
weeks of treatment. Non-inferiority in the VAS score was established only at 2 weeks.
There were no significant differences in the secondary endpoints between the groups. Skin
disorders were more frequent in the SFPP group; however, there was no difference in
gastrointestinal (GI) adverse effects.
Conclusions: The therapeutic efficacy of SFPP monotherapy for knee OA, with
respect to changes in the VAS, was not shown to be non-inferior to conventional treatment
at 4 weeks; however, non-inferiority was established at 2 weeks. The functional
improvement in the SFPP group was comparable to that of the control group. No severe GI
adverse effects associated with SFPP administration were observed; however, it is
necessary to pay more attention to the occurrence of skin disorders with SFPP than with
conventional topical NSAIDs.
INTRODUCTION
Knee osteoarthritis (OA) is commonly seen in middle-aged and elderly people. It results
from the regression of articular structures, such as articular cartilage.1) The main symptoms of knee OA include
chronic pain, inflammation, and motor dysfunction; overall, these significantly reduce the
quality of life (QOL)2) and
constitute a risk factor of locomotive syndrome.3,4)
Currently, land-based exercise, weight management, and mind–body exercise are core
treatments for knee OA, and core treatments alone or in combination with interventions are
recommended as multimodal treatments.5) Pain control is important when performing exercise, and it was
revealed that about half of the patients receiving physical therapy used non-steroidal
anti-inflammatory drugs (NSAIDs).6) Topical NSAIDs are the most strongly recommended treatment
modality according to the latest Osteoarthritis Research Society International (OARSI)
guidelines, whereas oral NSAIDs are conditionally recommended.5)
S-Flurbiprofen plaster (SFPP), which contains the primary active NSAID S-flurbiprofen, was
launched in Japan in January 2016. S-Flurbiprofen is highly skin permeable and reaches a
significantly higher concentration in the synovium than topical flurbiprofen does.7) The usage of SFPP is limited to two
patches (total 80 mg/day), and the systemic effects of NSAIDs can be anticipated. Pain
relief with SFPP is superior to that obtained with topical flurbiprofen.8) In a previous study on the efficacy
of long-term SFPP administration, a marked improvement in the total clinical symptoms score
was observed 2–4 weeks after application; moreover, the improvement continued for 52
weeks.9) The major adverse
effects observed were skin disorders.9) Furthermore, the incidence of severe gastrointestinal (GI)
adverse effects was relatively low; the tolerability of SFPP was confirmed in a previous
long-term study.9)
In conventional interventions for knee OA, oral and topical NSAIDs have been used in
various combinations. Additionally, the concomitant use of prophylactic medicine for GI
adverse effects is required when administrating non-selective NSAIDs.5) The issue of polypharmacy in elderly
patients has also become prominent in recent years.10) Considering this social background, SFPP is anticipated to
be a beneficial option in the multimodal treatment of knee OA; however, clinical data on
SFPP use remain insufficient. Yataba et al.8) conducted a comparative study between SFPP and conventional
flurbiprofen patches and concluded that the pain relief was greater in the SFPP group. To
the best of our knowledge, no clinical study has compared the efficacy of SFPP monotherapy
with that of combined oral and topical NSAIDs. The objective of the current study was to
determine whether the efficacy of SFPP monotherapy was non-inferior to that of the
combination of conventional oral and topical NSAIDs in patients with knee OA. We
hypothesized that the efficacy of SFPP monotherapy would not be inferior to that of
combination therapy.
MATERIALS AND METHODS
This open-label, multicenter, prospective, randomized study was approved by the Ethics
Committee of Hirosaki University (#09H29003). A total of 222 participants with knee OA were
enrolled between November 2017 and July 2019 (173 women; 49 men; mean age ± standard
deviation (SD), 69.2 ± 9.9 years; mean height ± SD, 155.2 ± 8.6 cm; mean weight ± SD, 60.7
±11.6 kg). Participants with no pain in the non-target knee were included, and the quality
of pain (acute or chronic, severity of inflammation, central sensibilization) was not
considered in this study. The injection of hyaluronic acid or steroids was prohibited during
the study period. The commencement of new physical therapy during the study period was also
prohibited; however, patients who had already started physical therapy when participating in
this study were allowed to continue physical therapy. The inclusion and exclusion criteria
are shown in Table 1. The patients were randomly
assigned in a 1:1 ratio to either the SFPP group or the control group. The randomization
factors included gender (male and female), visual analog scale (VAS) score (≥60 and
<60 mm), Kellgren-Lawrence grade (II and III), current smoking (yes and no), and body
mass index (≥25 and <25 kg/m2). The assignment procedure was performed at the
data center, and the attending physicians were blinded to the process. The allocation system
used in this study was created by the data center. After obtaining informed consent from the
patients, the principal investigator accessed the website for allocation and entered the
randomization factors. Allocation was done by the minimization method. The allocation data
were stored on a server at the data center that was not accessible by the principal
investigator.
Table 1.
Inclusion and exclusion criteria of this study
| Inclusion criteria |
Exclusion criteria |
| · Age ≥20 years |
· History of knee arthroplasty in the target knee |
| · Kellgren-Lawrence Grade II or III knee osteoarthritis
in the target knee |
· Other knee pain or comorbidity (neuropsychiatric
diseases, dementia, severe hypertension, peptic ulcer, or skin disease) |
| · No treatment of the target knee osteoarthritis within
14 days prior to the start of the study (medications were allowed if needed) |
· History of dermatitis requiring treatment by any patch
formulation |
| · VAS score of ≥40 mm at the baseline |
· History of allergy to NSAIDs |
| · No pain in the non-target knee |
· Aspirin-induced asthma (induction of asthmatic attack
by NSAIDs) or a similar experience following treatment with other drugs (enoxacin
hydrate, lomefloxacin, norfloxacin, or prulifloxacin) |
|
· Pregnant or potentially pregnant women |
|
· Presence of other contraindications as per the product
document |
This study was conducted in compliance with the study protocol, the Declaration of
Helsinki, and the Ethical Guideline for Clinical Research and the Clinical Trials Act of the
Ministry of Health, Labour and Welfare of Japan, with the approval of the Ethics Committee
at each study institution. Written consent was obtained from the patients after an
appropriate explanation by the physicians.
The patients assigned to the SFPP group had SFPP applied once daily to the affected area,
and those assigned to the control group were treated with a combination of oral and topical
NSAIDs. The dose of SFPP was not specified in this study design and was determined by the
attending physician according to the patient’s symptoms. The oral NSAIDs used in the control
group included celecoxib 100 mg twice daily or loxoprofen 60 mg three times daily. NSAID
patches (40 mg ketoprofen or 100 mg loxoprofen) were applied to the affected area once daily
using tape. The treatment period was set at 4 weeks after referring to previous studies
examining the efficacy and safety of other topical NSAIDs including diclofenac11) and eltenac.12) The use of prophylactic
medications for gastritis was allowed at the discretion of the physician.
The primary endpoint of this study was the change in VAS scores (0−100 mm) for pain levels
while rising from a chair at 2 and 4 weeks after the start of treatment (or at the time of
discontinuation). The secondary endpoints included the changes in the Knee Injury and
Osteoarthritis Outcome Score (KOOS) for pain,13) the Japanese Orthopaedic Association (JOA) score,14) the two-step test,15) the 25-question Geriatric
Locomotive Function Scale (GLFS-25) score,16) and the EuroQOL 5 dimensions 5-level
(EQ-5D-5l) score,17) after 2 and 4 weeks of treatment. The safety endpoints were
the adverse effects that occurred during the 4-week treatment period and the administration
of gastric medications.
The change in VAS score after 2 and 4 weeks was based on a covariant model, with the
baseline VAS as a covariate and the treatment group as the independent variable, to
calculate the 95% confidence interval of the inter-group adjusted mean (control group minus
test group). In a previous study that used SFPP and a placebo, the standard deviation of the
change in VAS score was 17.1 mm.8,9)
As a principle of statistical analysis, one-third of the standard deviation can be set as
the non-inferiority margin if the evaluation value is normally distributed. Therefore, the
non-inferiority margin of the VAS score was defined as 6 mm in this study. Consequently, if
the upper limit of the inter-group 95% confidence interval is <6 mm, the study drug group
is considered to be non-inferior to the control drug group. The other endpoints were
compared between the groups using covariance analysis at baseline. The paired
t-test was used for comparing the pre- and post-treatment results between
the groups. Fisher’s exact test was performed to compare the incidence of adverse effects
between the groups and the number of subjects in which prophylactic medications for
gastritis were taken orally during the study. A total of 105 subjects were required in each
group to statistically demonstrate non-inferiority with a common standard deviation of
15.5 mm, a difference between the control and SFPP groups of 0 mm, a one-sided significance
level of 0.025, and a power of detection of 0.8. The single-sided significance level was
2.5% for the primary endpoint and 5% on both sides for the secondary endpoints and safety
assessment. All analyses were performed using R version 3.4.0.
RESULTS
In this study, 114 participants (mean age, 68.7 ± 10.2 years) were assigned to the SFPP
group and 108 (mean age, 69.7 ± 9.5 years) were assigned to the control group (Table 2). A total of 28 participants dropped out
during the investigation period for the following reasons: patient’s decision (n=3), adverse
events (n=14), discontinuation of study treatment (n=4), physician’s judgment (n=3), and
others (n=5) (including duplications) (Fig.
1).
Table 2.
Baseline characteristics
|
SFPP group
(n=114) |
Control group
(n=108) |
| Age [years] |
68.7 ± 10.2 |
69.7 ± 9.5 |
| Sex (male:female) |
25:89 |
24:84 |
| Height [cm] |
154.9 ± 7.7 |
155.5 ± 9.5 |
| Body weight [kg] |
60.7 ± 11.2 |
60.7 ± 12.1 |
| BMI [kg/m2] |
25.2 ± 4.0 |
25.0 ± 3.6 |
| Disease duration [days] |
581.8 ± 1388.4 |
610 ± 1400.1 |
| Comorbidity (n) |
60 |
50 |
| Gastrointestinal disorders |
|
|
| Gastritis |
4 |
2 |
| Others |
6 |
5 |
| Cardiovascular diseases |
|
|
| Hypertension |
39 |
39 |
| Arrhythmia |
2 |
1 |
| Ischemic heart disease |
0 |
1 |
| Others |
1 |
0 |
| Chronic kidney disease |
0 |
1 |
| Metabolic endocrine disease |
|
|
| Diabetes mellitus |
10 |
7 |
| Others |
17 |
13 |
The data are mean ± SD or n.
BMI: body mass index.
In the SFPP group, the VAS score changed from 58.3 ± 13.8 mm to 28.3 ± 22.5 mm at 2 weeks
(P<0.001) and to 26.4 ± 23.2 mm at 4 weeks (P<0.001). In the control group, the VAS
score changed from 59.6 ± 14.4 mm to 31.2 ± 20.9 mm at 2 weeks (P<0.001) and to 20.7 ±
18.4 mm at 4 weeks (P<0.001) (Figs. 2 and 3). The change in VAS score was determined using a
covariate model with the VAS score at baseline, which resulted in a change of −30.5 mm in
the SFPP group and −28.0 mm in the control group after 2 weeks, and −32.4 mm in the SFPP
group and −38.3 mm in the control group after 4 weeks (Table 3). After 2 weeks, the mean difference was −2.4 mm with a 95% confidence
interval of −8.4 to 3.6 mm. The upper limit of the 95% confidence interval did not exceed
the non-inferiority margin of 6 mm, and non-inferiority was therefore established. However,
after 4 weeks, the mean difference in the VAS score of 5.9 mm yielded a 95% confidence
interval of 0.1–11.7 mm and, consequently, non-inferiority was not established (Table 3).
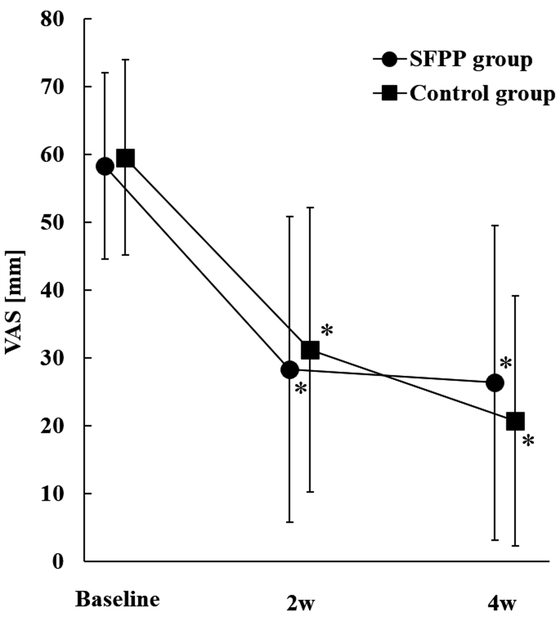
Table 3.
Changes in the VAS score
|
Baseline |
2 weeks |
4 weeks |
|
SFPP group
(n=114) |
Control group
(n=107) |
SFPP group
(n=99) |
Control group
(n=91) |
SFPP group
(n=107) |
Control group
(n=97) |
| VAS [mm] |
58.3 ± 13.8 |
59.6 ± 14.4 |
28.3 ± 22.5* |
31.2 ± 20.9* |
26.4 ± 23.2* |
20.7 ± 18.4* |
| Magnitude of change (covariate model) [mm] |
– |
– |
–30.5 |
–28.0 |
–32.4 |
–38.3 |
| Difference in the mean change (95% CI) [mm] |
– |
|
–2.4
(−8.4, 3.6) |
|
5.9
(0.1, 11.7) |
|
The data are mean ± SD.
*P<0.001 (paired t-test vs. baseline).
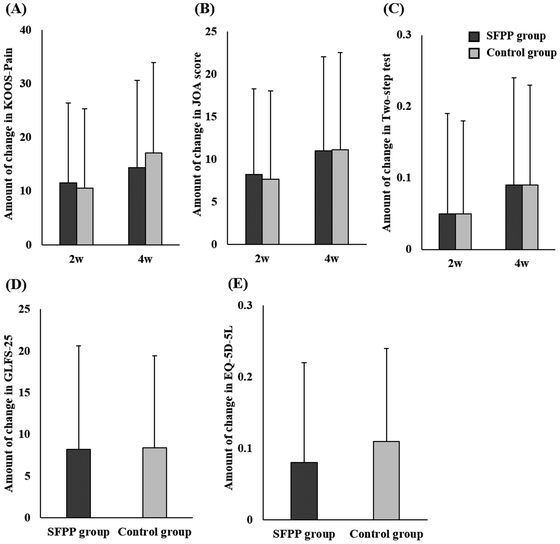
After treatment, the KOOS-Pain score, JOA score, two-step test, GLFS-25 score, and the
EQ-5D-5l score changed significantly in both the SFPP and control groups
(Table 4). There was no significant difference
in the size of the change in the KOOS-Pain score, JOA score, two-step test, GLFS-25, and
EQ-5D-5l between the groups (Fig.
4).
Table 4.
Other efficacy endpoints
|
SFPP group |
Control group |
| KOOS-Pain |
|
|
| Baseline |
56.9 ± 14.9 |
54.3 ± 15.5 |
| 2 weeks |
68.1 ± 16.8* |
64.9 ± 14.6* |
| 4 weeks |
71.3 ± 16.2* |
71.9 ± 14.3* |
| JOA score |
|
|
| Baseline |
74.7 ± 12.9 |
73.9 ± 12.9 |
| 2 weeks |
82.9 ± 14.6* |
81.7 ± 12.5* |
| 4 weeks |
85.8 ± 15.0* |
85.1 ± 11.7* |
| Two-step test |
|
|
| Baseline |
1.01 ± 0.21 |
0.96 ± 0.21 |
| 2 weeks |
1.06 ± 0.23* |
1.03 ± 0.22* |
| 4 weeks |
1.11 ± 0.24* |
1.06 ± 0.22* |
| GLFS-25 |
|
|
| Baseline |
23.2 ± 14.1 |
25.9 ± 15.8 |
| 4 weeks |
16.3 ± 13.7* |
16.8 ± 12.8* |
| EQ-5D-5l |
|
|
| Baseline |
0.74 ± 0.14 |
0.71 ± 0.15 |
| 4 weeks |
0.81 ± 0.12* |
0.82 ± 0.12* |
The data are mean ± SD.
*P<0.001 (paired t-test vs. baseline).
A total of 31 adverse events occurred during the study period (25 in the SFPP group, and 6
in the control group) (Table 5). The incidence
of adverse events was significantly higher in the SFPP group (P<0.001). The main adverse
events noted in the SFPP group were skin disorders, such as dermatitis, erythema, and
eczema. The incidence of these adverse events was significantly higher in the SFPP group
than in the control group (P<0.001). Three GI adverse effects in the SFPP group and two
in the control group were noted, with no significant difference between the groups
(P=1.000).
Table 5.
List of adverse effects
|
Total
(n=222) |
SFPP group
(n=114) |
Control group
(n=108) |
P-value |
| Total number of adverse events |
31 (14.0) |
25 (21.9) |
6 (5.6) |
<0.001 |
| Skin disorders |
|
|
|
<0.001 |
| Dermatitis |
7 (3.2) |
7 (6.1) |
– |
| Erythema |
6 (2.7) |
4 (3.5) |
2 (1.9) |
| Eczema |
4 (1.8) |
4 (3.5) |
– |
| Itching |
3 (1.4) |
2 (1.8) |
1 (0.9) |
| Contact dermatitis |
3 (1.4) |
3 (2.6) |
– |
| Gastrointestinal disorders |
|
|
|
1.000 |
| Abdominal discomfort |
3 (1.4) |
1 (0.9) |
2 (1.9) |
| Nausea |
2 (0.9) |
2 (1.8) |
– |
| Oral ulcer |
2 (0.9) |
1 (0.9) |
1 (0.9) |
1.000 |
| Palpebral swelling |
1 (0.5) |
1 (0.9) |
– |
1.000 |
The data show the number of cases (%).
Medication for gastritis was administered prophylactically at the start of treatment for
none of the patients in the SFPP group and for 25 patients in the control group
(P<0.001). Medications for gastritis were prescribed prophylactically or therapeutically
for adverse events for 5 patients in the SFPP group and 39 patients in the control group
(P<0.001) at 2 weeks, and for 4 patients in the SFPP group and 34 patients in the control
group (P<0.001) at 4 weeks (Table 6).
Table 6.
The use of medication for gastrointestinal disorders and reasons
|
Baseline |
2 weeks |
4 weeks |
|
SFPP group
(n=114) |
Control group
(n=108) |
P-value |
SFPP group
(n=112) |
Control group
(n=101) |
P-value |
SFPP group
(n=100) |
Control group
(n=96) |
P-value |
| Total number of uses of medication |
0 |
25 (23.1) |
<0.001 |
5 (4.5) |
39 (38.6) |
<0.001 |
4 (4.0) |
34 (35.4) |
<0.001 |
| Preventive administration |
0 |
25 (23.1) |
<0.001 |
4 (3.6) |
37 (36.6) |
<0.001 |
3 (3.0) |
32 (33.3) |
<0.001 |
| Gastric coating agent |
0 |
19 |
|
1 |
30 |
|
0 |
28 |
|
| PPI |
0 |
5 |
|
2 |
7 |
|
2 |
5 |
|
| H2-blocker |
0 |
1 |
|
0 |
2 |
|
0 |
1 |
|
| Acid suppressant |
0 |
0 |
|
0 |
0 |
|
1 |
0 |
|
| Others |
0 |
0 |
|
1 |
2 |
|
0 |
2 |
|
| Treatment of gastrointestinal adverse event |
– |
– |
– |
1 (0.9) |
2 (2.0) |
0.605 |
1 (1.0) |
2 (2.1) |
0.615 |
| Gastric coating agent |
– |
– |
|
1 |
1 |
|
1 |
1 |
|
| PPI |
– |
– |
|
0 |
1 |
|
0 |
1 |
|
| H2-blocker |
– |
– |
|
0 |
0 |
|
0 |
0 |
|
| Acid suppressant |
– |
– |
|
0 |
0 |
|
0 |
0 |
|
| Others |
– |
– |
|
0 |
0 |
|
0 |
0 |
|
The data show the number of cases (%).
Fisher's exact test was performed.
Some subjects were prescribed more than one of medicine.
H2 blocker: histamine type 2 receptor antagonist.
DISCUSSION
In this study, the treatment efficacy of SFPP monotherapy was found not to be non-inferior
to conventional treatment at 4 weeks following the initiation of treatment. However, VAS
score results within the non-inferiority margin were exhibited at 2 weeks, and there were no
significant differences in the secondary endpoints between the two groups. The incidence of
skin disorders was significantly higher in the SFPP group; in contrast, the incidence of GI
adverse effects in the SFPP group (without prophylactic administration) was similar to that
in the control group.
Yataba et al.9) demonstrated
that the number of patients with marked improvement continuously increased from 2 to 52
weeks after SFPP application in the patients’ global assessment. Moreover, their study
suggested that the improvement in the clinical symptom score was apparent in the early
phase, especially during the first 2 weeks. In a phase 3 randomized controlled trial, the
superiority of SFPP to conventional topical NSAIDs, in terms of efficacy, was
demonstrated.8) The
improvement in VAS scores following rising from a chair was 40.9 mm in the SFPP group and
30.6 mm in the flurbiprofen patch group, the difference being significantly higher in the
SFPP group.8) Considering the
recommendation of the OARSI guideline,5) SFPP may play a crucial role as an initial treatment for knee
OA because its non-inferiority was established at 2 weeks in this study, but not at 4
weeks.
The incidence of skin disorders was 17.5% in the SFPP group and 2.8% in the control group.
In a previous study investigating the safety of SFPP, drug-related skin symptoms were
observed in 46.8% of application sites.9) A systematic review demonstrated that adverse effects of
conventional topical NSAIDs on the application site were found in up to 39.3%
patients.18) In the current
study, skin disorders were observed in 17.5% of patients in the SFPP group. Although it has
been suggested that topical NSAIDs are relatively effective and safe for OA,19) skin disorders cannot be ignored
from the viewpoint of compliance. Physicians should be aware of the incidence of skin
disorders and obtain informed consent from the patient when treating OA with SFPP.
Although it is well known that oral NSAIDs display a superior effect on pain, the greatest
challenges with their administration are the numerous adverse effects, such as GI
symptoms,20) cardiovascular
diseases,21) and renal
dysfunction.22) Because the
absorption of oral drugs increases the incidence of these adverse effects, the OARSI
guidelines recommend using non-selective NSAIDs with a proton pump inhibitor (PPI) or a
COX-2 inhibitor while administering oral NSAIDs.5) A systematic review by Sardana et al.23) examined 3619 patients with knee
OA and found that topical ketoprofen was associated with fewer adverse GI events than oral
celecoxib and had a similar frequency of adverse GI events to that of a topical placebo.
Yataba et al.9) reported the
incidence of GI adverse events as 3 in 101 patients treated with SFPP 40 mg/day and 9 in 100
patients treated with SFPP 80 mg/day over the 52-week treatment period. They also reported
no cardiovascular complications associated with SFPP. Regarding renal function, no
clinically significant increase compared to the baseline in blood urea nitrogen or
creatinine was reported after the start of treatment.9,24) In the current study, GI adverse events were confirmed at a
rate of 2.6% in the SFPP group and 1.9% in the control group, with no significant
difference. The combination of prophylactic medications for gastritis was allowed in this
study design. In fact, significantly more patients were administered with prophylactic
medications in the control group than in the SFPP group. Consequently, these results
suggested that the risk of GI adverse events during treatment with SFPP was just as low as,
if not lower than, that with conventional treatment.
This study had some limitations. First, the therapeutic agents used in the control group
were not uniform, and the use of prophylactic medication for gastritis was allowed at the
discretion of the physician. The OARSI guideline recommends the use of non-selective NSAIDs,
preferably with the addition of a proton pump inhibitor, or a selective COX-2 inhibitor as a
conditional recommendation (Level 1B).5) In clinical practice, the type of NSAID is selected according
to the patient characteristics or comorbidities. Similarly, the prophylactic prescription of
anti-gastritis medication could differ among the attending physicians. This multicenter
study was designed to be generalized to actual clinical practice by comparing the efficacy
of SFPP and conventional NSAIDs, which many surgeons currently prescribe. Therefore, the
choice of NSAID and prophylactic administration for gastritis was flexible in this study.
Second, the dose of SPFF was not specified. When 80 mg of SFPP was applied, the dose equaled
that of an oral flurbiprofen preparation. To evaluate the systemic analgesic effect of SFPP
absorbed through the skin, it may have been better to standardize the dose of SFPP at
80 mg/day. However, this study was designed so that the therapeutic effects could be
examined by using drug administration methods that were as close as possible to the actual
clinical situation. This approach was taken because the analgesic effect of SFPP might have
been overestimated if the dose of SFPP specified as 80 mg/day did not match actual clinical
situation. Third, physical activity, muscle mass, and the walking ability of the patients at
baseline were not collected in this study. Differences in levels of physical activity might
influence the objective and subjective outcomes of the treatment for knee OA patients.
Fourth, the application time of topical NSAIDs might affect the incidence of skin adverse
events. Although the SFPP group demonstrated higher numbers of skin adverse events, the
application time of the compress could not be investigated in this study and was left to
principal physicians to decide. Finally, the treatment intervention period was only 4 weeks.
Previously, the analgesic effects of SFPP were observed early after
administration.8) However,
because our results revealed that the incidence of skin disorders was relatively high, it
was considered that a longer-term clinical study would be necessary to evaluate the
tolerability and safety of SFPP treatment.
CONCLUSIONS
The therapeutic efficacy of SFPP monotherapy in knee OA was not shown to be non-inferior to
conventional treatment at 4 weeks; however, its non-inferiority was established at 2 weeks
with respect to changes in the VAS score following rising from a chair. The functional
improvements in the SFPP group were comparable to those in the control group. No severe GI
adverse effects associated with SFPP administration were observed; however, it will be
necessary to pay more attention to the occurrence of skin disorders with SFPP than with
conventional topical NSAIDs.
ACKNOWLEDGMENTS
We thank the following facilities for their participation in the study: Aomori Rosai
Hospital, Odate Municipal General Hospital, Japan Community Health Care Organization Akita
Hospital, Hirosaki Municipal Hospital, Hirosaki National Hospital, Kuroishi General
Hospital, Towada Municipal Central Hospital, Noheji General Hospital, Kishiya Seikei−Geka
Clinic Murakami Hospital, Yokoyama Orthopedic Clinic, Takamori Orthopedics, Internal
Medicine and Dental Clinic Kobose Hospital, Ikeda Kinen Hospital, Chihaya Hospital,
Yoshimura Orthopedic Clinic, Urata Orthopedic Clinic, Nanko Hospital, Koenji Orthopedic
Clinic, Machiya Orthopedic Clinic, Matsumoto Hospital, Ozawa Orthopedic Clinic, and
Sannomiya Clinic.
CONFLICTS OF INTEREST
Yasuyuki Ishibashi is on the speakers’ bureaus for Taisho Pharmaceutical Co., Ltd. and
Teijin Pharma Ltd. The other authors declare that there are no conflicts of interest.
REFERENCES
- 1. Lawrence RC, Felson DT, Helmick CG, Arnold LM,
Choi H, Deyo RA, Gabriel S, Hirsch R, Hochberg MC, Hunder GG, Jordan JM, Katz JN, Kremers
HM, Wolfe F, National Arthritis Data Workgroup: Estimates of the prevalence of arthritis
and other rheumatic conditions in the United States: Part II. Arthritis Rheum
2008;58:26–35. PMID:18163497, DOI:10.1002/art.23176
- 2. Michaud CM, McKenna MT, Begg S, Tomijima N,
Majmudar M, Bulzacchelli MT, Ebrahim S, Ezzati M, Salomon JA, Gaber Kreiser J, Hogan M,
Murray CJ: The burden of disease and injury in the United States 1996. Popul Health Metr
2006;4:11. PMID:17049081, DOI:10.1186/1478-7954-4-11
- 3. Chiba D, Tsuda E, Wada K, Kumagai G, Sasaki E,
Nawata A, Nakagomi S, Takahashi I, Nakaji S, Ishibashi Y: Lumbar spondylosis, lumbar
spinal stenosis, knee pain, back muscle strength are associated with the locomotive
syndrome: rural population study in Japan. J Orthop Sci 2016;21:366–372. PMID:27021251,
DOI:10.1016/j.jos.2016.02.006
- 4. Sasaki E, Ishibashi Y, Tsuda E, Ono A, Yamamoto
Y, Inoue R, Takahashi I, Umeda T, Nakaji S: Evaluation of locomotive disability using
loco-check: a cross-sectional study in the Japanese general population. J Orthop Sci
2013;18:121–129. PMID:23114857, DOI:10.1007/s00776-012-0329-2
- 5. Bannuru RR, Osani MC, Vaysbrot EE, Arden NK,
Bennell K, Bierma-Zeinstra SM, Kraus VB, Lohmander LS, Abbott JH, Bhandari M, Blanco FJ,
Espinosa R, Haugen IK, Lin J, Mandl LA, Moilanen E, Nakamura N, Snyder-Mackler L, Trojian
T, Underwood M, McAlindon TE: OARSI guidelines for the non-surgical management of knee,
hip, and polyarticular osteoarthritis. Osteoarthritis Cartilage 2019;27:1578–1589.
PMID:31278997, DOI:10.1016/j.joca.2019.06.011
- 6. Khoja SS, Almeida GJ, Freburger JK:
Recommendation rates for physical therapy, lifestyle counseling, and pain medications for
managing knee osteoarthritis in ambulatory care settings: a cross‐sectional analysis of
the National Ambulatory Care Survey (2007–2015). Arthritis Care Res 2020;72:184–192.
PMID:31595710, DOI:10.1002/acr.24064
- 7. Yataba I, Otsuka N, Matsushita I, Kamezawa M,
Yamada I, Sasaki S, Uebaba K, Matsumoto H, Hoshino Y: Plasma pharmacokinetics and synovial
concentrations of S-flurbiprofen plaster in humans. Eur J Clin Pharmacol 2016;72:53–59.
PMID:26438533, DOI:10.1007/s00228-015-1960-6
- 8. Yataba I, Otsuka N, Matsushita I, Matsumoto H,
Hoshino Y: Efficacy of S-flurbiprofen plaster in knee osteoarthritis treatment: results
from a phase III, randomized, active-controlled, adequate, and well-controlled trial. Mod
Rheumatol 2017;27:130–136. PMID:27168463,
DOI:10.1080/14397595.2016.1176624
- 9. Yataba I, Otsuka N, Matsushita I, Matsumoto H,
Hoshino Y: The long-term safety of S-flurbiprofen plaster for osteoarthritis patients: an
open-label, 52-week study. Clin Drug Investig 2016;36:673–682. PMID:27229525,
DOI:10.1007/s40261-016-0412-0
- 10. Kojima T, Matsui T, Suzuki Y, Takeya Y, Tomita N,
Kozaki K, Kuzuya M, Rakugi H, Arai H, Akishita M: Risk factors for adverse drug reactions
in older inpatients of geriatric wards at admission: multicenter study. Geriatr Gerontol
Int 2020;20:144–149. PMID:31829506, DOI:10.1111/ggi.13844
- 11. Bookman AA, Williams KS, Shainhouse JZ: Effect of
a topical diclofenac solution for relieving symptoms of primary osteoarthritis of the
knee: a randomized controlled trial. CMAJ 2004;171:333–338. PMID:15313991,
DOI:10.1503/cmaj.1031793
- 12. Ottillinger B, Gömör B, Michel BA, Pavelka K,
Beck W, Elsasser U: Efficacy and safety of eltenac gel in the treatment of knee
osteoarthritis. Osteoarthritis Cartilage 2001;9:273–280. PMID:11300751,
DOI:10.1053/joca.2000.0385
- 13. Roos EM, Engelhart L, Ranstam J, Anderson AF,
Irrgang JJ, Marx RG, Tegner Y, Davis AM: ICRS Recommendation Document: patient-reported
outcome instruments for use in patients with articular cartilage defects. Cartilage
2011;2:122–136. PMID:26069575, DOI:10.1177/1947603510391084
- 14. Okuda M, Omokawa S, Tanaka Y, Okahashi K, Akahane
M: Validity and reliability of the Japanese Orthopaedic Association score for
osteoarthritic knees. J Orthop Sci 2012;17:750–756. PMID:22868702,
DOI:10.1007/s00776-012-0274-0
- 15. Ogata T, Muranaga S, Ishibashi H, Ohe T, Izumida
R, Yoshimura N, Iwaya T, Nakamura K: Development of a screening program to assess motor
function in the adult population: a cross-sectional observational study. J Orthop Sci
2015;20:888–895. PMID:26008771, DOI:10.1007/s00776-015-0737-1
- 16. Seichi A, Hoshino Y, Doi T, Akai M, Tobimatsu Y,
Iwaya T: Development of a screening tool for risk of locomotive syndrome in the elderly:
the 25-question Geriatric Locomotive Function Scale. J Orthop Sci 2012;17:163–172.
PMID:22222445, DOI:10.1007/s00776-011-0193-5
- 17. Herdman M, Gudex C, Lloyd A, Janssen MF, Kind P,
Parkin D, Bonsel G, Badia X: Development and preliminary testing of the new five-level
version of EQ-5D (EQ-5D-5L). Qual Life Res 2011;20:1727–1736. PMID:21479777,
DOI:10.1007/s11136-011-9903-x
- 18. Makris U, Kohler MJ, Fraenkel L: Adverse effects
of topical nonsteroidal antiinflammatory drugs in older adults with osteoarthritis: a
systematic literature review. J Rheumatol 2010;37:1236–1243. PMID:20360183,
DOI:10.3899/jrheum.090935
- 19. Zeng C, Wei J, Persson MS, Sarmanova A, Doherty
M, Xie D, Wang Y, Li X, Li J, Long H, Lei G, Zhang W: Relative efficacy and safety of
topical non-steroidal anti-inflammatory drugs for osteoarthritis: a systematic review and
network meta-analysis of randomised controlled trials and observational studies. Br J
Sports Med 2018;52:642–650. PMID:29436380,
DOI:10.1136/bjsports-2017-098043
- 20. Bhatt DL, Scheiman J, Abraham NS, Antman EM, Chan
FK, Furberg CD, Johnson DA, Mahaffey KW, Quigley EM, Harrington RA, Bates ER, Bridges CR,
Eisenberg MJ, Ferrari VA, Hlatky MA, Kaul S, Lindner JR, Moliterno DJ, Mukherjee D,
Schofield RS, Rosenson RS, Stein JH, Weitz HH, Wesley DJ, American College of Cardiology
Foundation Task Force on Clinical Expert Consensus Documents: ACCF/ACG/AHA 2008 expert
consensus document on reducing the gastrointestinal risks of antiplatelet therapy and
NSAID use: a report of the American College of Cardiology Foundation Task Force on
Clinical Expert Consensus Documents. J Am Coll Cardiol 2008;52:1502–1517. PMID:19017521,
DOI:10.1016/j.jacc.2008.08.002
- 21. Trelle S, Reichenbach S, Wandel S, Hildebrand P,
Tschannen B, Villiger PM, Egger M, Jüni P: Cardiovascular safety of non-steroidal
anti-inflammatory drugs: network meta-analysis. BMJ 2011;342(jan11 1):c7086.
PMID:21224324, DOI:10.1136/bmj.c7086
- 22. Zhang J, Ding EL, Song Y: Adverse effects of
cyclooxygenase 2 inhibitors on renal and arrhythmia events: meta-analysis of randomized
trials. JAMA 2006;296:1619–1632. PMID:16968832,
DOI:10.1001/jama.296.13.jrv60015
- 23. Sardana V, Burzynski J, Zalzal P: Safety and
efficacy of topical ketoprofen in transfersome gel in knee osteoarthritis: a systematic
review. Musculoskelet Care 2017;15:114–121. PMID:27778435,
DOI:10.1002/msc.1163
- 24. Otsuka N, Yataba I, Matsushita I, Matsumoto H,
Hoshino Y, Terada Y: A minimal impact of long-term S-flurbiprofen plaster application on
kidney function in osteoarthritis patients. Clin Exp Nephrol 2017;21:1060–1067.
PMID:28378068, DOI:10.1007/s10157-017-1406-9
