ABSTRACT
Objectives: This study aimed to identify a position for core muscle activation (core activate position) for a seated subject and to design an exercise method using this position for rehabilitation during the daily maintenance or maintenance stages.
Methods: Thirteen young men participated as subjects in this study. We manufactured a chair in which the seat had an adjustable forward tilt angle. The subjects underwent ultrasonographic measurements of the thickness of the transversus abdominis, internal oblique, and external oblique muscles while sitting in the chair with the seat angle adjusted to 0°, 6°, or 12°. Further, we conducted image analysis to determine the positional relationships of these muscles using the following four points as landmarks: the anterior superior iliac spine, the posterior superior iliac spine, the fourth lumbar vertebra, and the seventh thoracic vertebra.
Results: Significant increases in the thickness of the transversus abdominis and external oblique muscles were observed when the seat forward tilt angle was adjusted to 12° (P <0.05). In the core activate position (which demonstrated effective activation of the transversus abdominis), the posterior superior iliac spine, the fourth lumbar vertebra, and the seventh thoracic vertebra were aligned in a straight line that was nearly perpendicular to the line connecting the anterior superior iliac spine and the posterior superior iliac spine.
Conclusions: This postural guidance can be applied to core exercise methods during maintenance rehabilitation.
INTRODUCTION
Whereas care during the acute and convalescent stages of rehabilitation in Japan is provided during the hospital stay, at the maintenance stage of rehabilitation, daily maintenance care is provided to patients undergoing the transition to living in a nursing-care facility or at home. In particular, a major goal of rehabilitation in the chronic phase is the improvement of the quality of life (QOL) in addition to expansion of activities of daily living (ADL) at a time when patients are faced with changes in physical function, the effects of sequelae, and aging. In the field that focuses on the prevention of nursing-care dependence, advances have been made in recent years in research on, and measures against, locomotive syndrome resulting from sarcopenia1) and frailty. However, reduced activities of the deep trunk muscles, in addition to weakness of the limb muscles, are likely to underlie these conditions; moreover, subjective symptoms such as “decreased walking speed” and “deteriorating balance” are difficult to detect early. Trunk stability is essential for movements of the limbs and also affects the accuracy of these movements. In particular, the transversus abdominis (TrA), which constitutes a deep layer of the trunk muscles, possesses a feed forward mechanism and contracts before limb movement, thereby increasing the activity of the multifidus muscles via the thoracolumbar fascia and stabilizing the vertebral segments together with the multifidus muscles.2) Moreover, delayed initiation or loss of contraction of the TrA reportedly results in motor control defects3); furthermore, functional deterioration of core muscles affects defensive responses to loss of balance and results in a decreased speed of movement. However, conventional methods of core muscle activation, such as those described by Sapsford and Hodges 4) and abdominal hollowing and bracing,5) are not sufficient as exercise in relation to overall bodily movements because the TrA contracts only for a few seconds. This short contraction results from the instructions that are given to rehabilitation patients, meaning that this contraction is not carried out in a persistent manner. To maintain and improve independence in ADL and physical functioning, an important goal of exercise in maintenance rehabilitation is to find tasks that each patient wants to do and is able to do and for the patient to repeat them every day as ADL. To achieve this goal, it is necessary to identify a posture that promotes persistent contraction of the TrA in an antigravity position and to activate the TrA as part of everyday life. This concept is different from the conventional method of training performed by individuals who visit a specific facility or instructor. Consequently, we propose that this core muscle activation exercise during maintenance rehabilitation be considered as a new method. The new approach of posture control during ADL extends the period in which people can live independently without long-term dependence on medical care. As a result, posture control during ADL has the potential not only to increase the fullness of each person’s life but also to contribute to the reduction of social costs in Japan, a country with a super-aged population.
In this study, we focused on both local and global muscles6) to propose a new exercise as part of maintenance rehabilitation. In particular, we identified a position for core muscle activation (the core activate position; CAP) in which the TrA (a muscle that is active immediately before limb movement) can be contracted persistently; the CAP can be used as a proposed method of exercise that can be performed during daily life activities.
This study aimed to establish the CAP posture in a simple and accurate manner and, consequently, to propose a new chronic-stage exercise method. The CAP posture is a position ideal for persistent contraction of the TrA, a deep-layered trunk muscle, and was established by posture analysis and core muscle thickness measurements in subjects sitting in a chair, the seat of which had a readily adjustable forward tilt angle.
MATERIALS AND METHODS
This study was designed in accordance with the Declaration of Helsinki. The subjects provided signed written consent after they and their parents received an adequate written explanation of the study outline and methods. This study was approved by the Research Ethics Review Committee of the Teikyo University of Science (# 18014).
SubjectsThe subjects were 13 healthy young men who exercised regularly; their mean age, body height, and body weight were 15.9 ± 0.7 years (range, 15–16 years), 168.6 ± 6.9 cm (156.0–183.0cm), and 59.3 ± 8.7 kg (50.0–77.0 kg).
MethodsTo examine the CAP limb position that facilitates persistent contraction of the TrA, we manufactured a chair in which the forward tilt angle of the seat was adjustable to 0°, 6°, and 12°. The height of the anterior end of the seat was 40 cm, which is the same as for an everyday chair.
The subjects adopted a natural sitting position in the chair with the seat angle adjusted to 0°, 6°, or 12°. They then underwent measurements with the three seat angles occurring in a random order. All measurements were completed within a day, with an interval of at least 30 min between tasks. The subjects were instructed to keep their feet shoulder-width apart, to look at a marker placed 2 m ahead at a height of 120 cm, to keep both upper limbs at the respective sides of their body, and to try to maintain a natural position. For each task, the subjects were instructed to sit and remain motionless for a minimum of 10 s before muscle thickness was measured at the time of exhalation. One reason for having subjects sit still for at least 10 s was to allow confirmation of whether continuous contraction was being maintained. In each seat position, ultrasound equipment (MicroMax, manufactured by SonoSite) was used with an 8-MHz linear probe for surface imaging to measure the thickness of the TrA, the obliquus internus abdominis, and the obliquus externus abdominis on the axis side (contralateral to the dominant hand) during the expiration phase. Muscle thickness was measured using the marking device of the ultrasound equipment with the fascia as a reference point; the displayed values were used as measured values. The sites of measurement were ~10 cm laterally to the navel with the probe placed on the short axis in the anteromedial area from the intersection of the infra-axillary line with the horizontal line at the umbilical level. The thicknesses of the three muscles were measured by a single skilled investigator with appropriate measures taken to ensure reproducibility. In this study, noninvasive measurement using an ultrasonic measuring device was performed to reduce the burden on the subjects. Regarding the relationship between the muscle thickness measured using the ultrasonic diagnostic device and muscle contraction, we referred to a previous study7) that reported a strong correlation between increased muscle thickness and increased muscle activity.
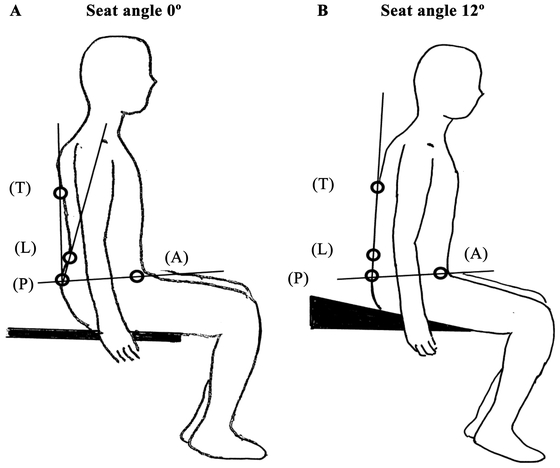
To analyze the subject’s posture during muscle thickness measurement, reflective markers were attached directly to the skin at the following four points: the anterior superior iliac spine (A), the posterior superior iliac spine (P), the L4 spinous process (L) located using the Jacoby line, and the Th7 spinous process (T) located using the line connecting the inferior angles of the scapula. A camera was placed 2 m laterally with the lens height adjusted to the navel height of the subject in a sitting position, and photographs were taken with flash. The data acquired were imported into Form Finder (Four Assist) software, and1) the angle formed by the line connecting A and P and the line connecting P and T,2) the angle formed by the line connecting A and P and the line connecting P and L, and3) the angle formed by AP and PT and AP and PL were calculated using a personal computer.
After the measurements were complete, subjects underwent an interview survey in which the following two questions were asked: “At which seat angle did you most feel trunk muscle contraction?” and “Which part of the buttocks supported your weight?”
Statistical analyses were performed to compare the thicknesses of the obliquus externus abdominis, obliquus internus abdominis, and TrA muscles with subjects in the sitting position for seat angles of 0°, 6°, and 12°1–3) and to compare the angles obtained from the posture analysis experiments. One-way analysis of variance was used initially and, if significance was found in the initial test, multiple comparison tests (Bonferroni) were performed with a significance level of 5%.
RESULTS
Comparison of the Thickness of the Obliquus Externus Abdominis, Obliquus Internus Abdominis, and TrA Muscles for Different Seat AnglesTable 1 shows the thickness of the TrA, obliquus internus abdominis, and obliquus externus abdominis measured at seat angles of 0°, 6°, and 12°. Statistical analyses indicated significant increases in the thickness of the TrA and obliquus externus abdominis (by 15% and 13%, respectively) at a seat angle of 12°, compared with those at 0° (P <0.05).
Table 1. Thickness measurements (cm) of the transversus abdominis, obliquus internus abdominis, and obliquus externus abdominis muscles in subjects sitting in a chair with the seat adjusted to different tilt angles
| Seat angle 0° | Forward tilt seat angle 6° | Forward tilt seat angle 12° |
| Transversus abdominis | 1.44 ± 0.18 | 1.57 ± 0.26 | 1.66 ± 0.30* |
| Obliquus internus abdominis | 3.10 ± 0.53 | 3.22 ± 0.79 | 3.30 ± 0.70 |
| Obliquus externus abdominis | 1.55 ± 0.17 | 1.67 ± 0.23 | 1.76 ± 0.34* |
*P <0.05 compared with the value at a seat angle of 0°.
The posture analysis results of 12 subjects were analyzed after the data for 1 subject were excluded because of missing images. No significant differences were found in the angle formed by the line connecting A and P and the line connecting P and T between seat angles of 0°, 6°, and 12°. However, a significant difference was found in the angle formed by the line connecting A and P and the line connecting P and L between seat angles of 0° and 12° (82.6 ± 11.2° versus 90.7 ± 8.2°; P <0.01). AP and PL were in a near-perpendicular relationship. Moreover, a significant difference was found in the angle formed by AP and PT and that formed by AP and PL between seat angles of 0° and 12° (4.4 ± 10.5° versus −2.7 ± 9.6°; P <0.05). T and L were in a linear positional relationship with P as the axis (Table 2).
Table 2. Angles in degrees formed by the P-L4 line and the P-Th7 line with the anterior superior iliac spine and the posterior superior iliac spine as the reference line
| Seat angle 0° | Forward tilt seat angle 6° | Forward tilt seat angle 12° |
| Angle formed by AP and PT | 87.0 ± 4.2 | 90.2 ± 7.4 | 88.1 ± 6.8 |
| Angle formed by AP and PL | 82.6 ± 11.2 | 87.7 ± 10.3 | 90.7 ± 8.2* |
| Difference in the angle formed by AP/ PT and that formed by AP/PL | 4.4 ± 10.5 | 2.5 ± 9.2 | −2.7 ± 9.6* |
*P <0.05 compared with the value at a seat angle of 0°.
See Fig. 1 for detailed angle definitions.
In response to the question “At which seat angle did you most feel trunk muscle contraction?” 85% the subjects answered that they “felt muscle movements between the umbilicus and the pubis when the seat had a forward tilt angle of 12°,” whereas 15% of the subjects answered, “not sure.” Palpation to confirm the answers to “Which part of the buttocks supported the weight?” revealed that the supporting region was the ischial region in 75% of the subjects.
DISCUSSION
In this study, we measured trunk muscle thickness and analyzed postures to establish the CAP (i.e., the posture at which the TrA is activated) in subjects sitting in a chair with a forward tilting seat. The highest increase in TrA thickness was observed when the seat had a forward tilt angle of 12°, at which angle the subjects’ postures were characterized by a near-perpendicular positional relationship between the line connecting A and P and the line connecting L and T with P as the axis; these results suggested that this posture represents the CAP (Fig. 1). To achieve CAP, the spinal column should be set to an intermediate position to minimize the anterior and posterior curvatures of the lumbar spine resulting from the posterior pelvic tilt, and the lumbar spine should be in a neutral position involving the pelvis/lumbar spine/thoracic spine.8) Maintenance of this posture allows for persistent contraction of the TrA. This position was deemed to be the CAP because the TrA and multifidus muscles cooperate to stabilize the neutral position.
In our previous research, we observed a point at which significant, persistent activation of the TrA could occur during front forward exercise. This type of exercise promotes a forward movement in which the subject gripped a rope hanging from the ceiling in a sitting position with both shoulder joints kept at 90° and both elbow joints in an extended position.9,10) However, this posture occurs during the course of motion and requires the skills of specialized staff to give the subject instruction/guidance. The current method to induce core activation using the CAP posture identified in this study is likely to be more accessible.
The seats of everyday chairs commonly have an approximate backward tilt angle of −3° to –5°, which induces a posterior pelvic tilt. Consequently, it is difficult to induce abdominal stimulation and attain core activation in such a chair; therefore, chairs of this type were excluded from our experiments. We manufactured a simple chair, the seat of which was adjustable to achieve forward tilt angles of 6° and 12°, in addition to that of 0°. The maximum forward tilt angle was set at 12° because the seated person may slip off the chair if the seat angle is >12°; the point midway between the maximum forward tilt angle and 0° (i.e., a forward tilt angle of 6°) was included among the measurement points. The thickness of the TrA and the positional relationship between the pelvic tilt angle and the spinal column were examined at these seat angles. The analysis of sitting positions at different forward tilt seat angles revealed a significant difference in the angle formed by AP and PL between seat angles of 0° and 12°, whereas no differences in the angle formed by AP and PT were found among seat angles of 0°, 6°, and 12°. In addition, there was a significant difference in the angles formed by AP and PT and AP and PL. PT indicates the positional relationship between the lower scapula and the posterior pelvis, whereas PL reflects the degree of lumbar lordosis. The angle between PT and PL was analyzed with respect to AP to clarify the degree of lordosis of the lumbar spine, which is informative for posture guidance.
As shown in the right panel of Fig. 1, the data suggest that, in CAP, the ischial bone supports the body weight, the pelvis is leveled, and the positional relationship between L and T is virtually linear with P as the axis. Being able to obtain persistent contraction of the TrA in subjects sitting in this chair with a seat angle of 12° and identifying the posture at that time should facilitate the design of a new technique for daily exercise.
In everyday life, chairs with a forward leaning angle of 12° are rare. Although sufficient care is needed while using this method if the spinal column is deformed or degenerated and pain is present, CAP can be achieved by adjusting the positions of AP and PL to achieve an angle close to 90°, with P as the axis in a sitting position. In this posture, AP is positioned parallel to the floor surface and sufficient ischial support of weight is possible. The persistent contraction of the TrA in the sitting position demonstrated in this study provides a condition suited for proper functioning of the diaphragm and pelvic floor muscles and elevation of intra-abdominal pressure for prolonged duration. As a result, it is expected to serve as a new exercise method as a part of maintenance rehabilitation to help prepare for exercise at home and to improve ADL and QOL. Conventional local muscle training is widely used not only for the training of elderly people in day care service centers, care prevention classes, and other settings, but also for training in sports facilities and health promotion facilities. However, many people cannot contract the TrA properly with these methods. Furthermore, even among those who can, contraction of the TrA is instantaneous and does not persist in some individuals, whereas, in other individuals, global muscles contract excessively Therefore, conventional exercise methods are not satisfactory in terms of activation of the TrA. In a previous study,11) we demonstrated that the thickness of TrA in the elderly was significantly lower than that in young subjects and suggested that the feed forward function of the TrA is insufficient because of decreased muscle activity. Based on those results, we discussed the insufficient feed forward function of the TrA as a possible factor responsible for the delayed initiation of limb movement, slow bodily movement, and accidents such as falls. Therefore, core muscle activation exercise as a part of maintenance rehabilitation may help elderly people to deal with various problems. This is particularly true if the exercise can impart the ability to predict the reaction force produced by limb movement and thereby induce contraction of the TrA and the multifidus muscles for persistent spinal stabilization.
The method of inducing persistent contraction of the TrA by maintaining a defined posture, as in the current study, is distinct from the approach used in the conventional method. Once CAP is acquired, step-by-step acquisition of exercise skills, such as confirmation of voluntary contraction of the TrA and multifidus muscles in coordination with global muscles, and the ability to contract the TrA at any site and in any posture, is achievable. Moreover, among individuals with chronic low back pain (a condition involving an uncoordinated relationship between local muscles and global muscles) those presenting with delay or loss of contraction of the TrA have been shown to have excessive activities of the internal and external oblique muscles.12) Because the vertebral segments are likely to be unstable in these patients, our newly proposed method could further be tested for application as home exercise for patients with low back pain.
In summary, we conclude that the CAP achieved by sitting in a chair with a forward tilt seat angle of 12° is effective and is expected to have a significant impact on core stability training.13) A positional relationship in which the line connecting A and P and the line connecting L and T are nearly perpendicular, with P as the axis, can be induced by sitting in a chair with the seat tilted forward at an angle of 12°. This posture can be applied to rehabilitation exercises to activate core muscles. Although appropriate care is needed while using this method, we propose the incorporation of CAP as part of ADL as a new exercise method that can be performed by people of any age and sex while eating, watching TV, or communicating. Aiming to expand the range of persistent contraction of the TrA could also contribute to the improvement of QOL.
ACKNOWLEDGMENTS
This study was supported by a Grant-in-Aid for Scientific Research (JP 18K12153) from JSPS.
CONFLICTS OF INTEREST
The authors declare that there are no conflicts of interest.
REFERENCES
- 1. Ikezoe T: Exercise for preventing physical disability in older people based on sarcopenia study [in Japanese]. Nippon Ronen Igakkai Zasshi 2013;50:770–772. PMID:24622222, DOI:10.3143/geriatrics.50.770
- 2.Hodges PW, Richardson CA: Contraction of the abdominal muscles associated with movement of the lower limb. Phys Ther 1997;77:132–142. .DOI:10.1093/ptj/77.2.132
- 3. Hodges PW, Richardson CA: Inefficient muscular stabilization of the lumbar spine associated with low back pain. A motor control evaluation of transversus abdominis. Spine 1996;21:2640–2650. PMID:8961451, DOI:10.1097/00007632-199611150-00014
- 4. Sapsford RR, Hodges PW: Contraction of the pelvic floor muscles during abdominal maneuvers. Arch Phys Med Rehabil 2001;82:1081–1088. PMID:11494188, DOI:10.1053/apmr.2001.24297
- 5. Grenier SG, McGill SM: Quantification of lumbar stability by using 2 different abdominal activation strategies. Arch Phys Med Rehabil 2007;88:54–62. PMID:17207676, DOI:10.1016/j.apmr.2006.10.014
- 6. Bergmark A: Stability of the lumbar spine. A study in mechanical engineering. Acta Orthop Scand 1989;60(sup230):1–54. PMID:2658468, DOI:10.3109/17453678909154177
- 7. McMeeken JM, Beith ID, Newham DJ, Milligan P, Critchley DJ: The relationship between EMG and change in thickness of transversus abdominis. Clin Biomech (Bristol, Avon) 2004;19:337–342. PMID:15109752, DOI:10.1016/j.clinbiomech.2004.01.007
- 8. Panjabi MM: The stabilizing system of the spine. Part II. Neutral zone and instability hypothesis. J Spinal Disord 1992;5:390–397, discussion 397. PMID:1490035, DOI:10.1097/00002517-199212000-00002
- 9. Miyashita S, Wada Y, Suzuki M: Examination of the effective trunk muscle training method – the transversus abdominis muscle and the internal oblique muscle measure muscular thickness of different movement [in Japanese]. Nihonbashi Gakkan Univ Bull 2012:41–51.
- 10. Miyashita S, Hashiguchi T, Ogawa H, Kato H, Miyashita T, Suzuki M, Manabe K, Iwanuma Iwanuma S [in Japanese]. Bull Teikyo Univ Sci 2016;12:17–24.
- 11. Wada Y, Miyashita S: Comparison of the activities of trunk muscles in terms of age and gender [in Japanese]. Redcord Sci 2013;1:31–40.
- 12. Hodges PW, Richardson CA: Delayed postural contraction of transversus abdominis in low back pain associated with movement of the lower limb. J Spinal Disord 1998;11:46–56. PMID:9493770, DOI:10.1097/00002517-199802000-00008
- 13. Willardson JM: Core stability training: applications to sports conditioning programs. J Strength Cond Res 2007;21:979–985. PMID:17685697, DOI:10.1519/00124278-200708000-00054