ABSTRACT
Background: Osteochondritis dissecans (OCD) of the humeral capitellum presents most typically in adolescent athletes who perform repetitive overhead activities. Earlier studies have demonstrated that conservative treatment of OCD is appropriate for patients with an open capitellar growth plate from the standpoint that spontaneous healing can be expected.
Case: A 12-year-old male baseball player with two years of experience with a local team participated in our medical check that included screening for capitellar OCD using ultrasonography. The subject experienced elbow pain when throwing, and ultrasonographic elbow examination indicated OCD of the capitellum, detected as irregularity of the subchondral bone of the capitellum. The initial radiograph, taken with the elbow at 45° of flexion, identified new bone formation in the lateral aspect of the OCD lesion; however the epiphyseal lines of the capitellum and lateral epicondyle were closed. We advised the patient to stop heavy use of the elbow, e.g., throwing and batting, and started conservative treatment in anticipation of spontaneous healing. Physiotherapy focusing on the shoulder girdle, core, and hip and lower limb stretches were performed to resolve general tightness. The OCD lesion had healed completely 12 months after the start of conservative treatment.
Discussion: Conservative treatment for young baseball players might be worth considering if lateral new bone formation within the OCD lesion is detected on radiographic findings, even if the epiphyseal lines of the capitellum and lateral epicondyle are closed.
INTRODUCTION
Osteochondritis dissecans (OCD) of the humeral capitellum is an elbow disorder related to sports activities such as baseball and gymnastics in immature athletes. The etiology of capitellar OCD in young baseball players is believed to be microtrauma caused by highly repetitive axial loading and the shearing force from radiocapitellar articulation during pitching.1,2,3) OCD of the humeral capitellum detected in the early stage of the disease can be treated conservatively.4,5) However, many patients with the earlier stages of OCD are asymptomatic. Previous studies have demonstrated that conservative treatment of OCD is appropriate for patients with an open capitellar growth plate from the standpoint that spontaneous healing can be expected.2,3,4,5) However, patients who do not respond to nonoperative treatment or who have advanced disease with unstable fragments could be indicated for surgical treatment.6,7,8,9) The earliest possible detection of OCD of the humeral capitellum is crucially important to prevent further radiohumeral joint degeneration. Portable ultrasonography equipment has been used to detect OCD of the humeral capitellum. This modality has good potential for detecting asymptomatic or minimally symptomatic OCD.10,11,12) Elbow OCD screening systems using ultrasonography are extremely useful for adolescent baseball players. This report describes the successful conservative treatment for OCD of the humeral capitellum in a 12-year-old baseball player with closed capitellum and lateral epicondyle growth plates who was diagnosed during an OCD ultrasound screening program.
CASE
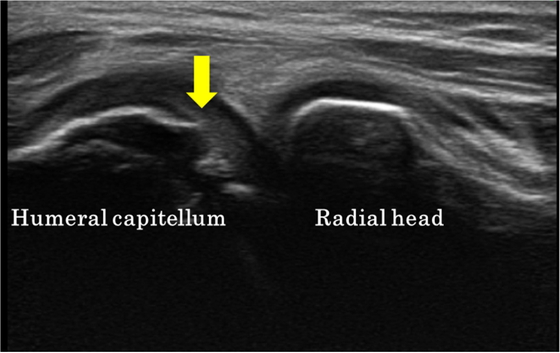
A 12-year-old male baseball player with 2 years of experience with a local team participated in our medical ultrasound screening program for capitellar OCD. The patient felt elbow pain on the throwing side when throwing and had mild tenderness of the humeroradial joint at the time of the medical check. The patient had visited an osteopathic clinic but had never visited a medical institution. During clinical examination, no tenderness of the lateral aspect of the right elbow or subjective elbow pain when moving was found. Active elbow flexion was up to 134°and extension was −4° with no instability on the throwing side, and active extension was 4° and flexion was 143° on the non-throwing side. The forearm range of motion was 90° for pronation and 90° for supination bilaterally. Sagittal-plane sonographic images of the humeral capitellum showed irregularity and discontinuity of the subchondral bone (Fig. 1).
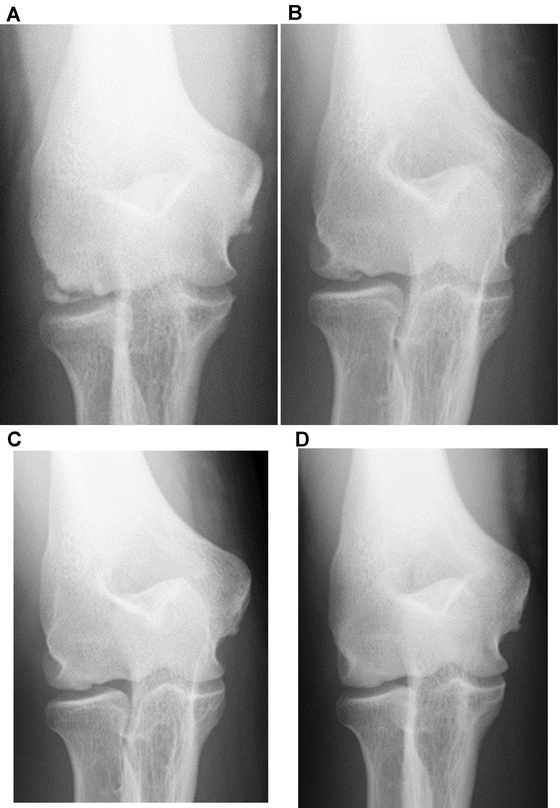
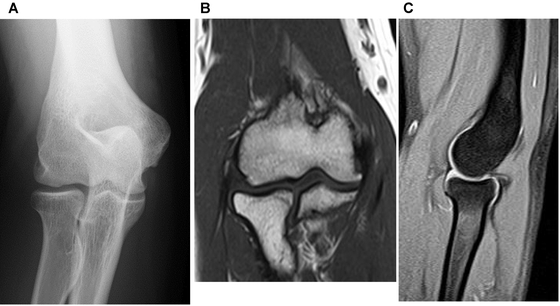
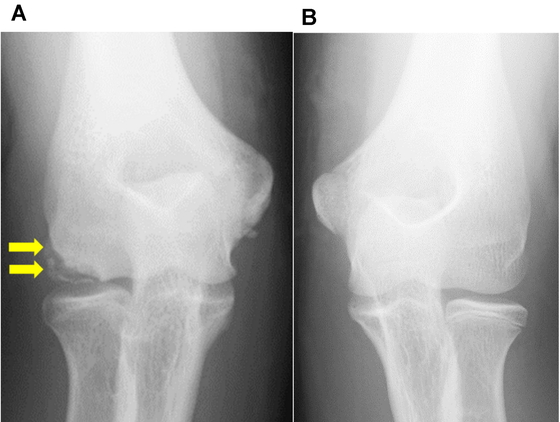
Radiography conducted at the first examination revealed an osteochondral lesion on the lateral side of the capitellum and new bone formation along the lateral side of the capitellum; closed capitellar and lateral epicondyle growth plates were also indicated (Fig. 2A). Radiography of the elbow joint of the non-throwing side at the initial visit also demonstrated that the epiphyseal lines of the capitellum and lateral epicondyle were already closed (Fig. 2B). We diagnosed the patient as having capitellar OCD and instructed him to stop heavy use of elbow, e.g., to avoid throwing and batting, arm wrestling, push-ups, and weightlifting. Posterior shoulder girdle tightness of the throwing side and tightness of the bilateral quadriceps muscle and iliopsoas muscle were observed. Physiotherapy focusing on the shoulder girdle, core, and hip and lower limb stretches were performed to resolve general tightness. Healing developed gradually with growth of the epiphysis of the capitellum and lateral epicondyle: Figure 3 shows radiographs taken at 3, 6, 9, and 12 months. In the current case, we did not conduct magnetic resonance imaging (MRI), which can be useful for evaluating the stability and viability of OCD fragments. 7,8) If conservative treatment had failed and we had eventually switched to surgical treatment, an MRI examination would have been carried out to facilitate selection of the surgical method. The patient returned to baseball activities 13 months after the start of conservative treatment and continued playing without any throwing-related elbow pain. Radiographic and magnetic resonance imaging 5 months after the patient returned to baseball demonstrated no recurrence of OCD (Fig. 4A-C). Written informed consent for the publication of this case report was obtained from the patient and his parent.
DISCUSSION
Using an ultrasound system, we detected symptomatic OCD of the capitellum during an elbow check-up of a young baseball player. Previous studies have demonstrated the usefulness of check-up programs with sonographic examination to detect early-stage OCD.10,11,12) Through sonographic examination, Matsuura et al. reported finding that 22 of 1040 baseball players had OCD of the capitellum.11) In addition, 18 of these 22 players (81.8%) had stage I OCD, which is characterized by radiolucent areas in the radiographic staging system. Furthermore, 7 of the 22 patients (31.8%) with OCD had no experience of elbow pain. Our patient had experienced elbow pain when throwing, but he had not sought medical help. We found irregularity of the subchondral bone of the capitellum on an ultrasonographic medical check. The patient’s initial anteroposterior radiographs, taken with the elbow flexed at 45°, identified new bone formation in the lateral aspect of capitellar OCD lesion. Patient and doctor delay are very common in daily clinical practice involving capitellar OCD, and a high index of suspicion is advised.13) These results suggest that sonographic examination could improve early recognition of OCD among young baseball players, and thereby allow increased opportunities for conservative treatment of OCD. Our conservative treatment regimen involved discontinuance of heavy elbow usage such as throwing, batting, arm wrestling, and carrying heavy loads, as earlier studies have indicated.2,4,5) Compliance with conservative therapy and prolonged patience in postponing the desired activity of playing baseball are crucial for young baseball players with capitellar OCD. Consequently, it is important to foster a trusting relationship with the patient and parents to encourage continuance and completion of the conservative therapy.
Previous studies have described the results of conservative treatment for elbow OCD. Takahara et al. reported that in 6 of 11 baseball players with early detection of OCD, the lesion healed or showed improved radiographic findings.2) They also reported that very early stage OCD lesions can heal spontaneously. Mihara et al. reported an association between the capitellar growth plate and the outcome of radiographic findings in 39 baseball players with elbow OCD in a nonoperative treatment series.5) Of these, 17 patients had an open growth plate, and 16 (94%) of them healed; in contrast, only 11 of 22 patients (50%) with a closed growth plate healed, reflecting a significant difference between the two groups (P= 0.0031). Moreover, Mihara et al. demonstrated a shorter duration of bone formation in patients with an open growth plate than in patients with a closed growth plate. These results suggest that the healing potential of elbow OCD is high in patients with an open growth plate. Funakoshi et al. investigated predictors of unsuccessful conservative treatment of capitellar OCD in a retrospective cohort study that included 245 elbows with capitellar OCD.14) That study revealed that pretreatment radiographic findings of radial head enlargement and advanced skeletal age of the throwing side compared with that of the nonthrowing side were predictors of the absence of spontaneous healing and advanced-stage capitellar OCD. In our patient, initial elbow radiographic examination showed no radial head enlargement, but there was advanced skeletal maturity compared with that of the non-throwing side, which suggested that conservative treatment could end in failure. However, new bone formation in the lateral aspect of the OCD lesion was established on initial radiographic findings. Endochondral ossification based on external bone formation of the OCD lesion progressed chronologically inward in this capitellar OCD lesion. The OCD lesion had healed by 12 months after the start of conservative treatment. During the growth period, the blood supply to the capitellum and the lateral aspect of the trochlea comes from the posterior condylar perforating vessels on the lateral aspect of the distal part of the humerus.15) New bone formation of the external OCD lesion, which benefits from the nutritional blood flow, might represent potential evidence of healing in young baseball players with capitellar OCD lesions, even if the epiphyseal lines of the capitellum and lateral epicondyle are closed.
CONCLUSION
This report describes the successful conservative treatment for OCD of the humeral capitellum of a 12-year-old baseball player with closed capitellum and lateral epicondyle growth plates. Screening for OCD of the humeral capitellum, detecting the disease in its earlier stages, and starting OCD treatment as early as possible are crucially important tenets of the conservative treatment of young baseball players. Conservative treatment for young baseball players could be worth considering if lateral new bone formation within the OCD lesion is detected on radiographic images, even if the epiphyseal lines of the capitellum and lateral epicondyle are closed.
CONFLICTS OF INTEREST
The authors declare that there are no conflicts of interest.
REFERENCES
- 1. Douglas G, Rang M: The role of trauma in the pathogenesis of the osteochondroses. Clin Orthop Relat Res 1981;158:28–32. PMID:7273524, DOI:10.1097/00003086-198107000-00005
- 2. Takahara M, Ogino T, Fukushima S, Tsuchida H, Kaneda K: Nonoperative treatment of osteochondritis dissecans of the humeral capitellum. Am J Sports Med 1999;27:728–732. PMID:10569357, DOI:10.1177/03635465990270060701
- 3. Takahara M, Ogino T, Takagi M, Tsuchida H, Orui H, Nambu T: Natural progression of osteochondritis dissecans of the humeral capitellum: initial observations. Radiology 2000;216:207–212. PMID:10887249, DOI:10.1148/radiology.216.1.r00jl29207
- 4. Matsuura T, Kashiwaguchi S, Iwase T, Takeda Y, Yasui N: Conservative treatment for osteochondrosis of the humeral capitellum. Am J Sports Med 2008;36:868–872. PMID:18219050, DOI:10.1177/0363546507312168
- 5. Mihara K, Tsutsui H, Nishinaka N, Yamaguchi K: Nonoperative treatment for osteochondritis dissecans of the capitellum. Am J Sports Med 2009;37:298–304. PMID:19059891, DOI:10.1177/0363546508324970
- 6. Byrd JW, Jones KS: Arthroscopic surgery for isolated capitellar osteochondritis dissecans in adolescent baseball players: minimum three-year follow-up. Am J Sports Med 2002;30:474–478. PMID:12130399, DOI:10.1177/03635465020300040401
- 7. Maruyama M, Takahara M, Harada M, Satake H, Takagi M: Outcomes of an open autologous osteochondral plug graft for capitellar osteochondritis dissecans: time to return to sports. Am J Sports Med 2014;42:2122–2127. PMID:24950681, DOI:10.1177/0363546514538759
- 8. Takahara M, Mura N, Sasaki J, Harada M, Ogino T: Classification, treatment, and outcome of osteochondritis dissecans of the humeral capitellum. J Bone Joint Surg Am 2007;89:1205–1214. PMID:17545422, DOI:10.2106/JBJS.F.00622
- 9. Yamamoto Y, Ishibashi Y, Tsuda E, Sato H, Toh S: Osteochondral autograft transplantation for osteochondritis dissecans of the elbow in juvenile baseball players: minimum 2-year follow-up. Am J Sports Med 2006;34:714–720. PMID:16382006, DOI:10.1177/0363546505282620
- 10. Harada M, Takahara M, Sasaki J, Mura N, Ito T, Ogino T: Using sonography for the early detection of elbow injuries among young baseball players. AJR Am J Roentgenol 2006;187:1436–1441. PMID:17114533, DOI:10.2214/AJR.05.1086
- 11.Matsuura T, Suzue N, Iwame T, Nishio S andSairyo K. Prevalence of osteochondritis dissecans of the capitellum in young baseball players: results based on ultrasonographic findings. Orthop J Sports Med 2014;2: DOI:10.1177/2325967114545298
- 12. Tajika T, Kobayashi T, Yamamoto A, Kaneko T, Shitara H, Shimoyama D, Iizuka Y, Okamura K, Yonemoto Y, Warita T, Ohsawa T, Nakajima I, Iizuka H, Takagishi K: A clinical and ultrasonographic study of risk factors for elbow injury in young baseball players. J Orthop Surg (Hong Kong) 2016;24:45–50. PMID:27122512, DOI:10.1177/230949901602400112
- 13.van Bergen CJ, van den Ende KI, ten Brinke B andEygendaal D. Osteochondritis dissecans of the capitellum in adolescents. World J Orthop 2016;7: 102–108. DOI:10.5312/wjo.v7.i2.102
- 14. Funakoshi T, Furushima K, Miyamoto A, Kusano H, Horiuchi Y, Itoh Y: Predictors of unsuccessful nonoperative management of capitellar osteochondritis dissecans. Am J Sports Med 2019;47:2691–2698. PMID:31348868, DOI:10.1177/0363546519863349
- 15. Haraldsson S: On osteochondrosis deformas juvenilis capituli humeri including investigation of intra-osseous vasculature in distal humerus. Acta Orthop Scand Suppl 1959;38:1–232.