Identification of the Exercise Load When Using a Balance Exercise Assist Robot
2021 年 6 巻 論文ID: 20210053
詳細
2021 年 6 巻 論文ID: 20210053
Objectives: The Balance Exercise Assist Robot (BEAR) is a boarding-type robot developed to improve users’ balance performance. However, the exercise load experienced by users of the BEAR remains unclear. Therefore, this study aimed to identify the exercise load of BEAR users.
Methods: Recruited healthy participants were fitted with an expiratory gas analyzer, and instructed to control the avatar displayed on the computer monitor by shifting their weight on the BEAR. Three types of activity (tennis, skiing, and rodeo) were prepared for the BEAR, and the difficulty of each activity had 40 levels. Each balance exercise for each level lasted for 90 s. The BEAR was administered at levels 1, 5, 10, and then up to 40 in steps of 5 for each activity. The major parameters that were evaluated were oxygen consumption (grossVO2, netVO2), metabolic equivalents (METs), and heart rate (HR). Two-way analysis of variance with Tukey’s post hoc test was applied to each level of each activity.
Results: Fourteen healthy participants were recruited. For the rodeo activity, netVO2 and MET values were significantly higher than those for tennis and skiing at level 20 (tennis vs. skiing vs. rodeo: netVO2 114.0±59.7 vs. 160.6±71.1 vs. 205.6±82.9, METs 1.47±0.22 vs. 1.72±0.37 vs. 1.90±0.29) and higher. Furthermore, comparisons within activity types showed that at level 40, netVO2 and MET were significantly higher than for level 1. The exercise intensity was found to increase along with the exercise level for all three activity types, with rodeo being the highest at 2.74 METs.
Conclusions: The current findings show that the BEAR can be used for balance practice without generating excessive cardiopulmonary stress.
New types of robotics technologies have been recently introduced to assist medical rehabilitation.1,2,3) Some of these devices are used to support the patient’s body4,5) and to assist the user’s motions mechanically.6,7) Other robots are programmed to improve or restore the skills or activities of the users.8) The Balance Assist Exercise Robot (BEAR) is the robot that was developed for balance practice, and operated by users’ weight shifting in the standing position.9)
The BEAR system has been developed to improve users’ balance performance. Users of the BEAR include patients with stroke, neuromuscular disease, frailty, or other balance disorders.9,10) These participants can perform the balance exercise by shifting his or her weight to control the BEAR so as to move the avatar on the monitor appropriately. Forward, backward, and rotation movements are performed with participants standing on the BEAR to shift their weight in the relevant direction. Therefore, participants are required to precisely control their body on the BEAR. Three types of exercises have been programmed into the BEAR system, and these exercises are presented as game activities (namely, tennis, skiing, and rodeo) on the computer monitor. The difficulty of each activity is determined by the speed and accuracy of the body displacements required of the participants. Each activity has 40 difficulty levels. Although the BEAR includes three types of activities, each with 40 difficulty levels, which of the activities makes the greatest demands on the participants remains unclear. Because the BEAR is a training robot for improving balance function, it is assumed that excessive load on cardiopulmonary function will not occur; however, this has not been sufficiently confirmed. Therefore, the way in which the load level of the BEAR interacts with the disease and level of frailty of the participants should be clarified.
The BEAR was originally intended for patients with diseases that affect balance. However, such patients may not be able to reach the highest level of difficulty in all three types of activities. In this study, we employed the BEAR in combination with expiratory gas analysis in healthy adult males to reliably measure the load level up to the highest difficulty level of each activity.
Expiratory gas analysis can measure the oxygen consumption during activities such as running and cycling, among others.11) Oxygen consumption during activity indicates the load intensity of that activity.12,13) By means of expiratory gas analysis, the load intensities of a wide range of activities have been elucidated.14) The current study was carried out to clarify the intensity of balance exercises when using the BEAR.
Our hypothesis was that the BEAR possesses specialized characteristics for balance training without generating excessive cardiopulmonary stress. This study aimed to clarify the load intensities of BEAR activities using expiratory gas analysis.
This study adhered to the guidelines of the Declaration of Helsinki and was conducted after obtaining approval from Hyogo College of Medicine Institutional Ethics Committee of Human Research (approval number: 1888; approval date: February 3, 2015). Informed consent was obtained from each participant prior to enrollment in the study. The examiner explained the study in writing, and the consenting participants filled out and signed the consent form.
The participants were healthy volunteers without orthopedic disease, central or peripheral nervous system disease, neuromuscular disease, cardiopulmonary disease, pain, or disabilities. Moreover, only male subjects were included as participants to minimize the variability associated with gender. All participants were instructed not to exercise excessively, eat, or drink large amounts of water for 30 min before the measurements were carried out.
The expiratory gas analyzer was calibrated prior to the measurements. The equipment was switched on at least 1 h before the calibration. Flow calibration was performed with a 2000-ml calibrator, and gas concentration calibration was performed with calibration gas.
Participants were fitted with the expiratory gas analysis system and electrocardiogram prior to a 10-min period of supine rest. After supine rest, participants then rested for 3 min in the sitting position. This sitting rest phase was used to establish the VO2 data at rest. While the participants remained in the sitting position, they were given an orientation on how to use and to manipulate the BEAR (Toyota Motor Corporation, Aichi, Japan) by watching a 2-min video in the sitting position after measurement of the resting blood pressure. Then, the participant stepped onto the BEAR to learn how to operate it. The participant operates the BEAR with assistance for support in the forward, backward, left, and right directions according to the instruction of the image on the monitor; participants also practice holding their position while balance disturbance is introduced. There was no programmed time limit for stepping onto the BEAR and learning how to maneuver; however, all participants completed this phase within 5 min. Next, to practice operation while looking at the actual training screen, the participant operates the BEAR while following the avatar on the monitor screen. Practice maneuvers while watching the training screen continued for up to 5 min. The expiratory gas analyzer had been worn continuously since the first 10 min of bed rest, and expiratory gas monitoring was performed continuously. After a break, one of the BEAR activities was started from level 1. The three activity types (tennis, skiing, and rodeo) were ordered randomly for each participant. Participants underwent the BEAR activities at levels 1, 5, 10, 15, 20, 25, 30, 35, and 40 in sequence while wearing the exhaled gas analyzer. Participant rested in a chair after every three to five activity levels. The participant moved to the next activity when level 40 was reached in the previous activity. The duration of each game level was 90 s. The maximum number of game trials played by a participant in 1 day was 12.
The primary endpoints using the expiratory gas analyzer and electrocardiogram were oxygen consumption (grossVO2, netVO2) and heart rate (HR). Secondary endpoints were metabolic equivalents (METs), respiratory rate (RR), tidal volume (TV), and oxygen pulse (O2pulse) which was calculated using the ratio of VO2 to HR. HR was expressed as the average value of the last 30 s of each 90-s game. Oxygen uptake, TV, RR, and O2pulse were measured breath-by-breath, and the rolling averages of these data were calculated. NetVO2 was calculated by subtracting the resting grossVO2 from the exercising grossVO2 to eliminate the effects of body weight and resting VO2. RR and TV were assessed to determine whether differences in ventilation pattern occurred in the three exercise types. O2pulse was assessed to see how much of an increase in stroke volume was associated with each level of each activity.
Blood pressure was measured during the rest time between every three to five games in batches. Blood pressure was also measured in the sitting position at the start and at the end of each activity type (i.e., at level 1 and level 40) for all subjects.
Data on grossVO2, HR, RR, and TV were averaged over the last 30 s of the first 3 min of sitting rest and for the last 30 s of each 90-s activity level. METs were obtained by dividing the average value of oxygen uptake during exercise by the body weight and by the average value of oxygen uptake in the sitting position.
The required participant sample size was calculated using JMP Pro 15. Power analysis was conducted with the following settings: between-group variance 1.0, within-group variance 2.0, significance level 0.05, power 0.8. Comparative tests between level 1 activities and other activity levels and between activities for METs, HR, RR, and TV were performed using repeated measures two-way ANOVA with SPSS 12.0 J and Tukey’s post-test. The level of significance was set at P <0.05. Blood pressure values at sitting rest before the start of the first activity and at the end of the 12 activity levels were compared using the t-test.
A total of 14 healthy participants were recruited. All participants were male, and their characteristics are presented in Table 1. Differences in grossVO2, net VO2, METs, HR, O2pulse, RR, and TV between different activity levels of the same activity and between activity types at the same level are shown in Table 2. Changes in netVO2, METs, and HR by activity level are also shown in Fig. 1. The main effects, effect sizes, and factor interactions by two-way analysis of variance with repeated measures are listed in Table 3. Blood pressures at rest and after performing each type of activity at level 40 are shown in Table 4.
| Characteristic | Value | |||
| Age | (years) | 25.7 | ± | 1.9 |
| Weight | (kg) | 64.4 | ± | 12.0 |
| Height | (cm) | 168.9 | ± | 5.3 |
| BMI | (kg/m2) | 22.6 | ± | 4.2 |
| Measurement days | (days) | 2.6 | ± | 0.9 |
| Resting data | ||||
| GrossVO2 | (ml/min) | 246.4 | ± | 49.2 |
| Heart rate | (beat/min) | 73.4 | ± | 8.7 |
| O2pulse | (ml/beat) | 3.4 | ± | 1.0 |
| Respiratory rate | (/min) | 17.5 | ± | 5.3 |
| Tidal volume | (ml) | 571.7 | ± | 104.7 |
| SBP | (mmHg) | 116.1 | ± | 9.6 |
| DBP | (mmHg) | 68.8 | ± | 8.5 |
BMI, body mass index; VO2, amount of oxygen uptake; O2pulse, oxygen uptake divided by heart rate; SBP, systolic blood pressure; DBP, diastolic blood pressure.
| grossVO2 (ml/min) | Level | Tennis | Skiing | Rodeo | |||||||||
| 1 | 331.2 | ± | 53.2 | 338.0 | ± | 69.9 | 332.9 | ± | 90.1 | ||||
| 5 | 338.7 | ± | 67.2 | 351.6 | ± | 63.9 | 378.2 | ± | 78.3 | ||||
| 10 | 346.7 | ± | 73.1 | 371.9 | ± | 71.1 | 388.5 | ± | 87.5 | ||||
| 15 | 340.4 | ± | 66.7 | 383.2 | ± | 82.9 | 417.5 | ± | 114.3 | ||||
| 20 | 362.9 | ± | 84.7 | 409.5 | ± | 89.8 | 454.5 | ± | 114.9 | b, ** | |||
| 25 | 356.2 | ± | 69.6 | 403.5 | ± | 84.2 | 468.6 | ± | 128.2 | b, ** | |||
| 30 | 381.7 | ± | 94.6 | 451.9 | ± | 88.7 | b | 528.1 | ± | 153.5 | b, **, § | ||
| 35 | 447.7 | ± | 93.3 | b | 475.2 | ± | 115.9 | b | 583.0 | ± | 149.4 | b, **, §§ | |
| 40 | 505.1 | ± | 126.9 | b | 539.7 | ± | 134.9 | b | 656.9 | ± | 191.7 | b, **, §§ | |
| netVO2 (ml/min) | Level | Tennis | Skiing | Rodeo | |||||||||
| 1 | 82.2 | ± | 38.0 | 89.0 | ± | 46.1 | 83.9 | ± | 59.4 | ||||
| 5 | 89.8 | ± | 44.7 | 102.6 | ± | 41.7 | 129.2 | ± | 60.1 | * | |||
| 10 | 97.8 | ± | 45.5 | 122.9 | ± | 56.0 | 139.5 | ± | 59.0 | * | |||
| 15 | 91.5 | ± | 46.1 | 134.3 | ± | 61.6 | a | 168.6 | ± | 86.4 | a, * | ||
| 20 | 114.0 | ± | 59.7 | 160.6 | ± | 71.1 | b, † | 205.6 | ± | 82.9 | b, **, § | ||
| 25 | 107.3 | ± | 47.5 | 154.6 | ± | 54.8 | b, † | 219.7 | ± | 93.4 | b, **, §§ | ||
| 30 | 132.8 | ± | 68.2 | a | 203.0 | ± | 56.8 | b, † | 279.1 | ± | 129.3 | b, **, § | |
| 35 | 198.7 | ± | 71.1 | b | 226.3 | ± | 86.3 | b | 334.1 | ± | 132.8 | b, **, §§ | |
| 40 | 256.2 | ± | 105.7 | b | 290.8 | ± | 109.5 | b | 408.0 | ± | 175.8 | b, **, §§ | |
| METs | Level | Tennis | Skiing | Rodeo | |||||||||
| 1 | 1.36 | ± | 0.24 | 1.39 | ± | 0.28 | 1.39 | ± | 0.23 | ||||
| 5 | 1.38 | ± | 0.19 | 1.45 | ± | 0.26 | 1.60 | ± | 0.29 | ||||
| 10 | 1.41 | ± | 0.23 | 1.56 | ± | 0.28 | 1.63 | ± | 0.23 | ||||
| 15 | 1.39 | ± | 0.19 | 1.60 | ± | 0.25 | 1.75 | ± | 0.34 | ||||
| 20 | 1.47 | ± | 0.22 | 1.72 | ± | 0.37 | 1.90 | ± | 0.29 | b, ** | |||
| 25 | 1.46 | ± | 0.26 | 1.69 | ± | 0.30 | 1.94 | ± | 0.37 | b, ** | |||
| 30 | 1.55 | ± | 0.26 | 1.93 | ± | 0.43 | b | 2.18 | ± | 0.39 | b, ** | ||
| 35 | 1.85 | ± | 0.27 | b | 2.02 | ± | 0.45 | b | 2.43 | ± | 0.65 | b, ** | |
| 40 | 2.06 | ± | 0.30 | b | 2.32 | ± | 0.46 | b | 2.74 | ± | 0.72 | b, **, § | |
| HR (beats/min) | Level | Tennis | Skiing | Rodeo | |||||||||
| 1 | 80.3 | ± | 9.0 | 83.9 | ± | 12.1 | 83.6 | ± | 8.6 | ||||
| 5 | 81.4 | ± | 8.7 | 86.7 | ± | 10.1 | 83.2 | ± | 5.8 | ||||
| 10 | 83.2 | ± | 9.8 | 86.7 | ± | 13.0 | 84.6 | ± | 6.8 | ||||
| 15 | 83.1 | ± | 9.3 | 86.7 | ± | 12.6 | 86.4 | ± | 7.4 | ||||
| 20 | 83.9 | ± | 9.2 | 88.3 | ± | 11.6 | 88.8 | ± | 8.0 | ||||
| 25 | 81.8 | ± | 9.9 | 89.3 | ± | 13.4 | 89.1 | ± | 8.5 | ||||
| 30 | 83.3 | ± | 8.6 | 90.7 | ± | 11.7 | 93.5 | ± | 11.1 | * | |||
| 35 | 85.6 | ± | 10.2 | 95.5 | ± | 12.9 | a, † | 98.1 | ± | 13.6 | b, ** | ||
| 40 | 90.8 | ± | 10.6 | b | 101.3 | ± | 12.7 | b, † | 107.4 | ± | 17.2 | b, ** | |
| O2pulse (ml/beat) | Level | Tennis | Skiing | Rodeo | |||||||||
| 1 | 4.19 | ± | 0.89 | 4.13 | ± | 1.13 | 4.04 | ± | 1.19 | ||||
| 5 | 4.22 | ± | 1.02 | 4.16 | ± | 1.11 | 4.56 | ± | 0.96 | ||||
| 10 | 4.23 | ± | 1.02 | 4.42 | ± | 1.21 | 4.61 | ± | 1.04 | ||||
| 15 | 4.14 | ± | 0.85 | 4.54 | ± | 1.29 | 4.85 | ± | 1.29 | ||||
| 20 | 4.34 | ± | 1.01 | 4.78 | ± | 1.49 | 5.16 | ± | 1.27 | b, ** | |||
| 25 | 4.42 | ± | 0.95 | 4.68 | ± | 1.46 | 5.29 | ± | 1.35 | b, * | |||
| 30 | 4.60 | ± | 1.08 | 5.12 | ± | 1.37 | a | 5.71 | ± | 1.55 | b, ** | ||
| 35 | 5.25 | ± | 1.06 | b | 5.12 | ± | 1.53 | b | 6.04 | ± | 1.58 | b, § | |
| 40 | 5.57 | ± | 1.16 | b | 5.48 | ± | 1.58 | b | 6.21 | ± | 1.65 | b | |
| RR (breath/min) | Level | Tennis | Skiing | Rodeo | |||||||||
| 1 | 23.0 | ± | 4.0 | 22.3 | ± | 3.9 | 22.9 | ± | 3.7 | ||||
| 5 | 23.2 | ± | 4.1 | 22.8 | ± | 4.0 | 24.1 | ± | 4.0 | ||||
| 10 | 23.5 | ± | 3.6 | b | 22.7 | ± | 3.6 | b | 23.8 | ± | 5.5 | b | |
| 15 | 23.4 | ± | 3.4 | 23.3 | ± | 4.4 | 24.7 | ± | 4.2 | ||||
| 20 | 24.1 | ± | 4.2 | b | 24.1 | ± | 4.0 | b | 26.1 | ± | 4.9 | b | |
| 25 | 24.2 | ± | 3.7 | b | 24.1 | ± | 5.5 | b | 25.4 | ± | 4.2 | b | |
| 30 | 25.7 | ± | 4.0 | b | 24.9 | ± | 5.6 | a | 26.4 | ± | 4.3 | b | |
| 35 | 26.2 | ± | 5.4 | 25.9 | ± | 5.6 | 27.5 | ± | 4.1 | ||||
| 40 | 29.0 | ± | 4.6 | 27.0 | ± | 6.3 | 28.4 | ± | 6.2 | ||||
| TV (ml/breath) | Level | Tennis | Skiing | Rodeo | |||||||||
| 1 | 562.9 | ± | 101.7 | 587.7 | ± | 113.8 | 572.2 | ± | 86.7 | ||||
| 5 | 563.9 | ± | 91.1 | 596.0 | ± | 103.0 | 594.0 | ± | 111.5 | ||||
| 10 | 564.8 | ± | 90.8 | 603.8 | ± | 118.7 | 618.3 | ± | 134.6 | ||||
| 15 | 569.2 | ± | 75.2 | 606.8 | ± | 115.1 | 638.0 | ± | 143.2 | ||||
| 20 | 588.1 | ± | 145.6 | 607.4 | ± | 115.3 | 643.6 | ± | 159.1 | b | |||
| 25 | 562.5 | ± | 85.3 | a | 613.3 | ± | 122.0 | b | 662.7 | ± | 127.8 | b | |
| 30 | 572.7 | ± | 93.8 | 643.8 | ± | 113.1 | 685.6 | ± | 170.1 | b, * | |||
| 35 | 631.2 | ± | 107.0 | 643.7 | ± | 119.8 | 723.6 | ± | 197.1 | ** | |||
| 40 | 662.0 | ± | 159.4 | 686.9 | ± | 119.4 | 733.1 | ± | 184.6 | ||||
Data are mean ± SD.
a, P <0.05 vs. level 1; b, P <0.01 vs. level 1; *, P <0.05 tennis vs. rodeo; **, P <0.01 tennis vs. rodeo; †, P <0.05 tennis vs. skiing; §, P <0.05 skiing vs. rodeo; §§, P <0.01 skiing vs. rodeo.
VO2, amount of oxygen uptake; HR, heart rate; VO2pulse, oxygen pulse; RR, respiratory rate, TV, tidal volume.
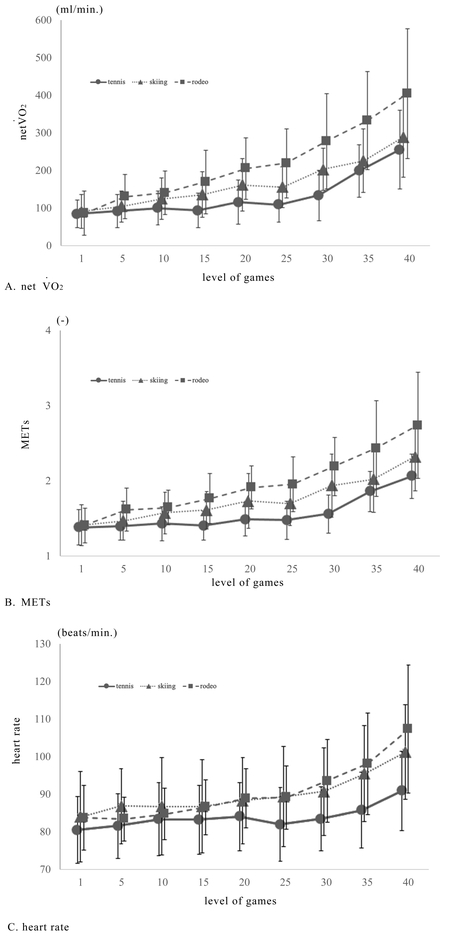
Cardiopulmonary parameters for increasing game levels. (A) netVO2, (B) METs, and (C) heart rate.
| Main effect interaction |
Degree of freedom F value |
Effect size η2 |
F value significance |
|||
| grossVO2 | type | F (2, 208) | = | 21.6 | 1.289 | ** |
| level | F (8, 208) | = | 68.5 | 5.269 | ** | |
| type*level | F (16, 208) | = | 6.6 | 0.713 | ** | |
| netVO2 | type | F (2, 208) | = | 21.6 | 1.289 | ** |
| level | F (8, 208) | = | 68.5 | 5.269 | ** | |
| type*level | F (16, 208) | = | 6.6 | 0.713 | ** | |
| METs | type | F (2, 208) | = | 14.8 | 1.067 | ** |
| level | F (8, 208) | = | 83.4 | 6.416 | ** | |
| type*level | F (16, 208) | = | 3.7 | 0.534 | ** | |
| HR | type | F (2, 208) | = | 8.1 | 0.789 | * |
| level | F (8, 208) | = | 41.8 | 3.215 | ** | |
| type*level | F (16, 208) | = | 4.2 | 0.568 | ** | |
| O2pulse | type | F (2, 208) | = | 7.2 | 0.744 | * |
| level | F (8, 208) | = | 60.7 | 4.669 | ** | |
| type*level | F (16, 208) | = | 4.1 | 0.562 | ** | |
| RR | type | F (2, 208) | = | 3.7 | 0.534 | * |
| level | F (8, 208) | = | 29.0 | 2.231 | ** | |
| type*level | F (16, 208) | = | 0.9 | 0.260 | n.s. | |
| TV | type | F (2, 208) | = | 6.4 | 0.702 | ** |
| level | F (8, 208) | = | 19.9 | 1.531 | ** | |
| type*level | F (16, 208) | = | 3.0 | 0.387 | ** | |
*, P <0.05; **, P <0.01.
| SBP (mmHg) | DBP (mmHg) | Significance | ||||||
| Rest | 115.3 | ± | 10.9 | 68.6 | ± | 8.3 | ||
| Tennis level 40 | 124.3 | ± | 13.9 | 75.4 | ± | 11.2 | * | |
| Skiing level 40 | 124.7 | ± | 14.6 | 79.6 | ± | 7.3 | * | |
| Rodeo level 40 | 124.4 | ± | 15.9 | 75.4 | ± | 10.0 | * | |
*, P <0.05.
SBP: systolic blood pressure, DBP: diastolic blood pressure.
Values of netVO2, METs, and O2pulse during the rodeo activity were significantly higher than those during tennis and skiing at levels 20 and above; however, no significant differences were observed between tennis and skiing. HR during rodeo was higher than for tennis at levels 30 and above, and HR during skiing was higher than for tennis at levels 35 and above. The RR was not significantly different at any level between the types of exercise, and the TV was significantly higher at level 30 and 35 for rodeo than for tennis. Systolic blood pressure increased significantly after performing level 40 of each exercise compared to the resting state. There was no significant difference in systolic blood pressure after exercise between the activity types.
Intra-type Exercise ComparisonAll subjects reached level 40, the highest level in all three events. For tennis, netVO2 was significantly higher at levels 30, 35, and 40 relative to level 1. For skiing and rodeo, netVO2 for levels 15, 20, 25, 30, 35, and 40 was significantly higher than for level 1. The METs were significantly higher for tennis at levels 35 and above compared with level 1. For skiing, the METs were higher at level 30 and above than for level 1, and for rodeo, the METs at level 20 and above were higher than for level 1. A significant difference in HR was observed between levels 1 and 40 for tennis. For skiing and rodeo, HRs were significantly higher at levels 35 and 40 than at level 1. A significant difference in RR was observed between levels 1 and 10–30 in all types of exercises; however, the standard deviation of RR was higher for level 35 and above, and the differences with level 1 were not significant. For TV, significant differences were observed between levels 1 and 25 for tennis and skiing, and between levels 1 and 20/25/30 for rodeo.
In this study, we attempted to quantify the exercise loads of tennis, skiing, and rodeo activities using the BEAR. The results indicated that the BEAR can be used to achieve balance functions without excessive cardiopulmonary stress.
The BEAR is a robot on which the user stands; it is controlled by weight shifting by the user. Although several studies15,16,17) have reported the effect of robots on users’ oxygen consumption, reports for boarding type robots are limited.18) Many types of robots assist users’ motions, such as gait and standing up, by supporting their body from the ceiling or attaching some equipment to their body. The VO2 measurements for users of these robots indicate how efficiently the robot influences users’ gait or other motions.
The BEAR does not assist the user’s motion but is operated by users standing on the device. The BEAR was developed to improve balance function for the injured, the infirm, and elderly people; however, the exercise load that this device requires has not been quantified. To the best of our knowledge, there is no report on the prevalence of adverse events during balance training using the BEAR. If the exercise load of the device is unknown, there is a possibility that unexpected adverse events may be involved if the participant is frail or has respiratory or cardiovascular disease. Therefore, this study aimed to quantify the load for each activity type and level during BEAR use.
GrossVO2 shows the actual value of oxygen consumption; however, it is affected by body weight and the resting value. However, the use of METs excludes these effects. 1 MET is defined as VO2 divided by the body weight and then divided by VO2 in the resting position.15) In this study, this value was set to 1 MET. A comparison of METs showed that the highest value was found for level 40 during rodeo; the exercise intensity for rodeo was higher than those for the other disciplines at all levels. The exercise load for level 40 in rodeo was 2.74 METs; that for cleaning and preparing food in the kitchen, washing dishes, playing with children, and caregiver-assisted activities with light exertion is in the range 2.3–3.0 METs.14) The highest rodeo exercise intensity using the BEAR is suggested, therefore, to correspond to the intensity of these activities. Significant differences in netVO2, METs, and O2pulse between different levels were found in tennis, skiing, and rodeo between levels 1 and 35, 30, and 20, respectively.
Tennis and skiing were characterized by more frequent maneuvers and larger displacements as the activity level increased. To achieve these frequent maneuvers and large displacements for each maneuver, the subjects needed to exert themselves physically. Therefore, it was considered that the oxygen consumption increased as the activity level increased. The reason for the highest VO2 being for rodeo is thought to be the unique kinetic characteristics of this discipline. In tennis and skiing, the subject controls the robot to move it, but in rodeo, the subject has to control the robot so that it does not move. The spontaneous movements of the robot are in the forward-backward and rotational directions, and the subject must exert isometric muscle forces in the flexion-extension-rotation directions of the trunk and upper extremities to inhibit these movements. As a result of mobilizing the activities of these many muscles, it can be inferred that VO2 values during the rodeo were higher. The fact that tennis requires manipulation only in the forward-backward direction and skiing only in the rotational direction, whereas rodeo requires manipulation in both directions, may have contributed to the increase in VO2.
For these reasons, rodeo was considered to have the highest oxygen consumption. However, the maximum oxygen consumption for rodeo was only 2.74 METs, which is very unlikely to induce excessive cardiopulmonary stress.
The subjects of this study were all men. It is possible that variation in the measured results was minimized by limiting the range of subjects. According to previous studies,19) men have a larger skeletal muscle volume than women, and therefore have a higher basal metabolic rate and a higher energy metabolism during exercise. Therefore, it is possible that the VO2 values obtained in this study would be smaller in women.
All participants were healthy subjects in their 20s; consequently, the results of the present study cannot accurately represent the cardiopulmonary response in diseased, elderly, or frail participants. Therefore, the results of this study should be cautiously applied to diseased and frail groups. The fourteen subjects in this study showed statistically significant differences between activities and for higher activity levels, but more robust results may be obtained with a larger number of subjects.
During the measurements, the sequence in which the activities were presented was randomly selected; however, the levels increased in order from levels 1 to 40 for all participants and for all three activities. Therefore, learning effects and exercise loadings could have accumulated, and these effects may have occurred on the cardiopulmonary response at high levels. Therefore, the randomization of levels should be considered in the future to ensure that the subjects start from the complete resting position at each level.
The duration of each game was 90 s, and the VO2 values were averaged over the final 30 s. The maximum VO2 obtained in this study was about 650 ml/min at level 40. Previous studies20) have shown that a steady state can be reached in about 2 min if VO2 is below 1500 ml/min. However, considering the kinetics of gas exchange during exercise, it was possible that gas exchange did not reach the steady state.
In this study, we investigated the effect of balance training with the BEAR on cardiopulmonary function using expiratory gas analysis and heart rate monitoring. The results showed that the intensity of exercise increased as the level increased for all three types of exercise, with rodeo being the most intense. Although the effects on cardiorespiratory function were observed at level 20 and above, the exercise intensity induced by the BEAR was less than 3 METs, suggesting that the use of the BEAR by frail subjects and patients with respiratory or cardiovascular diseases would be reasonable.
The authors have declared that no conflict of interest exists.