Original Article
Investigation of the Continuity and Usefulness of the “Infinite Recipe” Salt Reduction System Developed by Shimane University
2024 年 41 巻 3 号 p. 53-61
詳細
2024 年 41 巻 3 号 p. 53-61
Salt reduction is essential for the prevention and treatment of hypertension. Thus, novel strategies for salt reduction measures are necessary. We have developed a “low-sodium system” that is “infinitely rearrangeable” using a menu application, frozen ingredients, and low-sodium retort sauce by utilizing Shimane University’s patented technology. In 10 hypertensive subjects (systolic blood pressure (SBP) greater than 130 mmHg and less than 180 mmHg) that were not administered with antihypertensive treatment continued to consume a reduced-salt diet for 28 days. Throughout the study period, the feeding rate for all subjects was 90.0% (504/560). The completion rate (28 days) of the 10 subjects in the study was 100%. Before and after the intervention, the average SBP for all subjects showed a downtrend (morning SBP; 139.0, 125.3 mmHg: night; 128.8, 121.7 mmHg, respectively) with reductions in the 24-hour urinary sodium excretion and salt checklist score. The continuity and usefulness of the “infinite recipe” salt reduction system was inferred.
Salt restriction is important in the treatment of hypertension, and the Japanese Society of Hypertension recommends less than 6 g of salt per day [1]. However, this is not considered a long-term treatment because of the pain associated with “bad taste” and “poor flavor.” Moreover, salt control at home is difficult, and home-delivered low-sodium frozen foods have limited menus and are ineffective when incorporated in one’s diet. Thus, novel strategies for salt reduction measures are necessary.
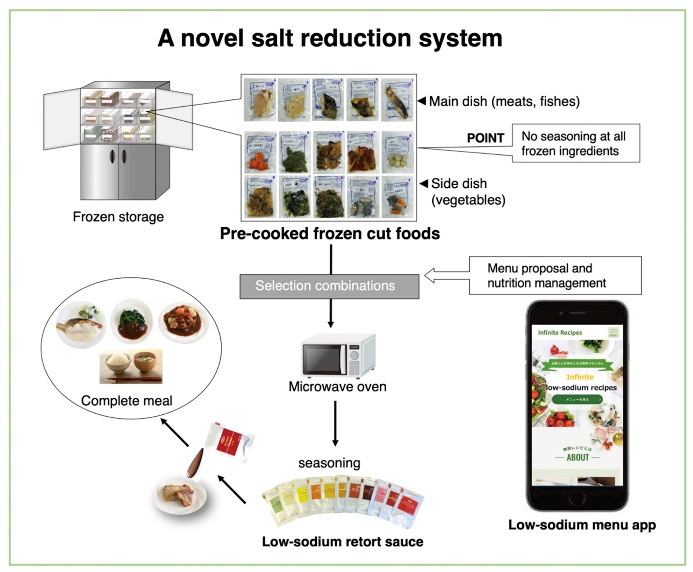
Although the antihypertensive effect of salt reduction has been verified in many countries worldwide, intervention studies have been conducted by simply providing nutritional guidance (salt intake of 6 grams or less per day) or imposing uniform dietary restrictions with research institutes outsourcing low-sodium diets [2, 3]. This makes it difficult to implement correct salt restrictions or to maintain a semi-compulsory diet for long periods of time at home. Therefore, we have developed a “low-sodium system” that is “delicious,” “easy to cook,” and “infinitely rearrangeable” using a menu application, frozen ingredients, and low-sodium retort sauce based on Shimane University’s patented technology (Patent No.6714238) [4] in collaboration with industry and academia. In this pilot study, we investigated the continuity and usefulness of the novel salt reduction system. Therefore, the subjects were tested to see if this system would allow them to continue on a low-sodium diet for an extended period of time (28 days).
The “infinite recipe” salt reduction system
This study was conducted with the approval of by the Medical Research Ethics Committee, Shimane University Faculty of Medicine, (20160519-1: UMIN000049601).
In the low-sodium system, the frozen ingredients were not seasoned in any way, and after being microwaved, they were seasoned with a low-sodium sauce. The frozen ingredients and low-sodium sauces were freely combined (about 8,000 combinations) at home using a menu application (Fig.1). Soy sauce and dressing were also used to add flavor to the side dishes. All recipes are less than 2 g and the average total calories per meal was approximately 580 kcal (Table 1). The 28-day (56 meals) menu was delivered to the subjects’ homes thrice, twice for 10 days, and once for 8 days. This delivery method was used because it is an opportunity for the subjects to demonstrate their willingness to continue in the study.
| Menu |
Energy (kcal) |
Protein (g) |
Lipid (g) |
Carbohydrate (g) |
Salt content (g) |
|
|---|---|---|---|---|---|---|
| 1 | White rice | 280 | 4.5 | 0.5 | 66.8 | 0 |
|
Sauteed pork with Nanban sauce Side dish: asparagus and bell peppers |
236 | 17.7 | 14.3 | 10.1 | 0.9 | |
| Taro with mayonnaise | 76 | 1.3 | 4.6 | 8.2 | 0.2 | |
| total | 592 | 23.5 | 19.4 | 85 | 1.1 | |
| 2 | White rice | 280 | 4.5 | 0.5 | 66.8 | 0 |
| Curry soup with beef (asparagus) | 305 | 13 | 23.8 | 11 | 1.6 | |
| Cabbage and tuna salad | 33 | 6 | 0.2 | 2.4 | 0.3 | |
| total | 618 | 23.5 | 24.6 | 80.2 | 1.9 | |
| 3 | White rice | 280 | 4.5 | 0.5 | 66.8 | 0 |
| Chicken and broccoli with Shrimp sauce | 166 | 18.2 | 8.9 | 4.8 | 0.6 | |
| Cabbage with sesame paste | 22 | 0.9 | 1.2 | 2.7 | 0.1 | |
| Pumpkin with mayonnaise | 87 | 1.5 | 4.7 | 11.2 | 0.2 | |
| total | 555 | 25.1 | 15.3 | 85.5 | 0.9 | |
| 4 | White rice | 280 | 4.5 | 0.5 | 66.8 | 0 |
|
Salmon/Miso sauce Assorted dishes: INGEN (Japanese beans) |
134 | 14.9 | 4.4 | 9.8 | 0.9 | |
| Omelet | 70 | 4.3 | 2.9 | 6.6 | 0.5 | |
| Taro with mayonnaise | 76 | 1.3 | 4.6 | 8.2 | 0.2 | |
| total | 560 | 25 | 12.4 | 91.3 | 1.5 | |
| 5 | White rice mixed with a raw egg | 352 | 10.7 | 5.6 | 67.1 | 0.3 |
| Miso soup with low-salt miso | 45 | 3.4 | 1.7 | 5.1 | 0.7 | |
|
Sawara (spanish mackerel) with Cream Sauce Assorted dishes: eggplant |
157 | 12.6 | 10.9 | 3.7 | 0.3 | |
| Spinach with sesame dressing | 15 | 1.6 | 0.4 | 2.6 | 0.5 | |
| total | 568 | 28.2 | 18.5 | 78.6 | 1.8 | |
| 6 | White rice | 280 | 4.5 | 0.5 | 66.8 | 0 |
|
Mackerel with Lemon sauce Assorted dishes: broccoli, cauliflower |
218 | 11.3 | 17.6 | 4.2 | 1.1 | |
| Komatsuna with French dressing | 19 | 0.8 | 0.2 | 2.1 | 0.3 | |
| Boiled egg | 65 | 5.8 | 4.3 | 0.7 | 0.6 | |
| total | 582 | 22.4 | 22.6 | 73.7 | 2 | |
| 7 | White rice | 280 | 4.5 | 0.5 | 66.8 | 0 |
| Fried prawns | 135 | 5.6 | 7.6 | 11.2 | 0.5 | |
| Cabbage and tuna salad | 33 | 6 | 0.2 | 2.4 | 0.3 | |
| Pumpkin and mushrooms with Nanban sauce | 85 | 2.6 | 0.9 | 19.5 | 0.8 | |
| total | 533 | 18.7 | 9.3 | 99.9 | 1.6 | |
| Average of 7 meals | 572 | 23.8 | 17.5 | 84.9 | 1.5 |
Menu and nutrition for seven meals selected by subject No.1.
Bold for low-sodium sources.
Study design and subjects
This study enrolled 10 Izumo City Hall (Shimane, Japan) employees who agreed to participate in the research. The eligibility criteria were as follows: hypertensives (SBP greater than 130 mmHg and less than 180 mmHg) who were not administered with antihypertensive treatment. On the other hand, patients on hemodialysis or peritoneal dialysis with potassium restriction were excluded from the study. The 10 subjects were not concentrated in a particular department (e.g., Health and Welfare Department), but were assigned to different departments.
In accordance with the study design, these 10 subjects learned the correct blood pressure measurement method via video, took blood pressure readings at home every morning and evening for three weeks using the same sphygmomanometer, and entered those blood pressure levels into the application. The subjects measured their blood pressure twice, entered the measurements into the application, and the average value was automatically recorded. After three weeks (observation period prior to intervention study), we observed that there was less variation in each of the measurements in all of the subjects. From this information, the principal investigator confirmed that all of them met the eligibility criteria (130–180 mmHg). The planned number of cases for this study was 10, so the study was performed. Height and weight were measured at the beginning of the study.
Primary endpoint
According to the meta-analysis literature [3], of the 136 references cited, 57% had an intervention duration of 14 days or less, 21% 15–30days, and 4% more than 60 days. As a result, antihypertensive effects were observed with intervention periods of 2 weeks or longer, and there was no significant change in these effects when the intervention was continued for 30 days or longer. Therefore, the 28-day intervention period was judged to be reasonable. Twenty four-hour urine storage was done at home on the day before the study began and on the last day of the study and submitted to the Izumo City Hall health office the next day.
Evaluation criteria and judgment
In this study, instead of having fully cooked low-sodium meals (all meals) delivered to the home during the intervention period, the participants create and order their own menus using an application, range up the ingredients they receive, and then season them with sauces. In addition, each intake must be recorded. Considering this time-consuming process and the fact that the intervention trial lasted 28 days, including weekends and holidays, we judged the salt reduction system to be sustainable if subjects met the following criteria by the end of the intervention period designed for this study. In this research plan, a minimum of one meal per day and at least three days per week (approximately 40%) or at least 40% (22 meals) of the study period (28 days) was considered the standard for utilization compliance. The study was designed to examine continuity, and in light of the aforementioned conditions, the criteria were not met if the subject did not eat a reduced-sodium diet for more than one week. Therefore, we asked the subjects to consume the low-sodium diet provided to them, if possible, two meals a day (not mandatory, and explained that it was acceptable for them to eat one meal). The subjects were aware that they could withdraw from the study at any time by submitting a withdrawal of consent form. The subjects received the selected food items by home delivery service on three separate occasions and were allowed to stop receiving them.
Secondary endpoint
The secondary endpoint was “observation of the average change in systolic blood pressure (SBP) for all participants”. The criterion was set as “completion” if the proportion of the subjects who continued until the end of the study was 40% or more. During the observation period of 3 weeks, all subjects learned from the application the precautions for home blood pressure measurement as described in the Hypertension Guidelines 2019, and we confirmed that all subjects measured their home blood pressure correctly in the same way. Moreover, subjects entered and recorded their daily food intake and morning and evening blood pressure readings in the application accordingly. The subjects used an arm band blood pressure monitor and entered the measured blood pressure values twice into the application, which automatically indicated the average of the two measurements. The subjects’ daily salt intake was measured before and after the intervention via a 24-hour urine collection using U-Mate P (SB-Kawasumi Lab. Inc., Kanagawa). The measurement of the urine sodium levels was outsourced to the Japan Institute of Medical Laboratory Medicine, Inc. (Kyoto, Japan). Before and after the intervention, the subjects were administered with the salt checklist [5] and entered their responses into the application (Fig. 2). All information was obtained by transmission using ID numbers.
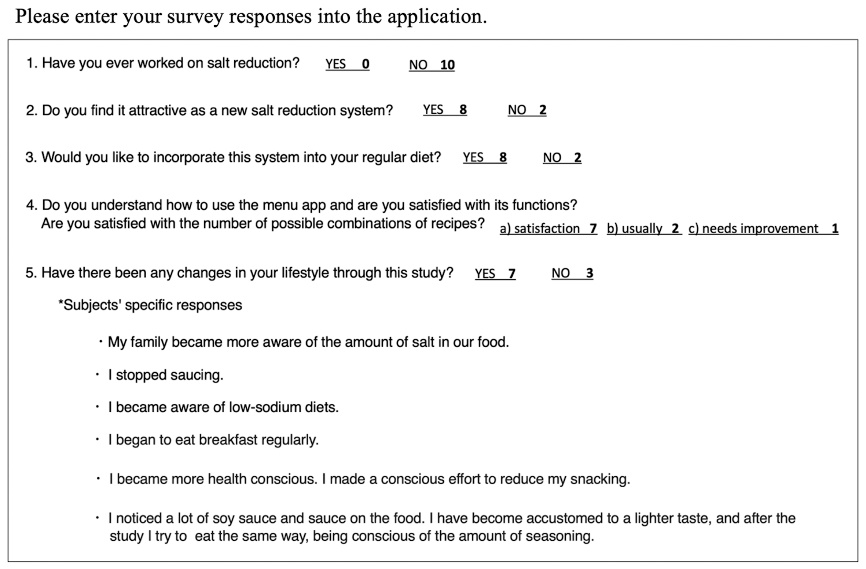
According to the pre-determined menu for the day, all subjects ate two low-sodium meals a day for four weeks in principle and recorded the meals they ate for breakfast, lunch, and dinner into the application on a daily basis. Interestingly, all 10 subjects who were always able to discontinue the study never submitted a withdrawal of consent form and wished to continue food delivery. Therefore, the completion rate (28 days) of the 10 subjects in the study was 100%, indicating that the developed salt reduction system is expected to have continuity (Table 2). The subjects were asked to eat two meals per day, and the average consumption rate for all subjects was 90.0% (506/560 meals: 95%CI 82.40–98.24). Some subjects ate three meals a day instead of only one meal a day. The salt reduction system based on the patented technology is not limited to the use of low-sodium sauces; any seasoning can be used. The low-sodium menu application taught the correct use of seasonings using measuring spoons and misting bottles, and the subjects indicated in the questionnaire that they understood and were able to practice what was described (Fig. 2). Although two meals per day were required, the subjects could eat breakfast, lunch, and dinner at any time of the day. The percentage of breakfast, lunch, and dinner meals eaten were 47.0 (95%CI 40.8–52.2), 20.8 (95%CI 5.5–34.5), and 32.2% (95%CI 19.6–44.2), respectively. The subjects selected a breakfast menu that actively incorporated potassium-rich vegetables and was expected to reduce salt intake (type of breakfast recommended in the application).
For the secondary endpoint, the pre- and post-intervention antihypertensive effect, we observed a downtrend in the mean morning and evening SBP in all subjects (Fig. 3A and Table 2). Next, the subjects were divided into two groups according to the magnitude of blood pressure drop. Five subjects showed a downtrend in SBP that is associated with a reduction in the 24-hour urinary sodium excretion before and after the intervention (Fig. 3B). This group had a greater blood pressure response to salt reduction and might be possibly salt-sensitive.
The post-intervention questionnaire strongly suggested that all subjects were likely to accept the salt reduction system and continue their salt reduction lifestyle in an enjoyable manner. Behavioral changes in eating habits were also observed, such as the participants becoming more “salt conscious” on a daily basis. Eight out of 10 participants indicated that they would like to incorporate this system into their daily diet in the future (Fig. 2). It is noteworthy that the average salt checklist score two months after the end of the intervention study did not differ from the low value observed immediately after the end of the study (data not shown).
| Subjects | Age | Sex | H | W | BMI | Intake of low-sodium foods during 28 days | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| BF | LU | DNR | Total |
Feeding rate (%) |
Continuity (28 days) |
||||||
| No.1 | 49 | F | 160.2 | 84.1 | 32.8 | 26 | 2 | 23 | 51 | 91 | YES |
| No.2 | 50 | F | 161.2 | 79.2 | 30.5 | 17 | 21 | 12 | 50 | 89.2 | YES |
| No.3 | 58 | F | 161.7 | 65 | 24.9 | 11 | 13 | 12 | 36 | 64.2 | YES |
| No.4 | 52 | M | 174.2 | 83.3 | 27.5 | 27 | 0 | 26 | 53 | 94.6 | YES |
| No.5 | 56 | M | 174.2 | 75.7 | 24.9 | 26 | 13 | 17 | 56 | 100 | YES |
| No.6 | 41 | M | 170.9 | 71.6 | 24.5 | 28 | 26 | 1 | 55 | 98.2 | YES |
| No.7 | 63 | M | 166.2 | 67.1 | 24.3 | 26 | 27 | 2 | 55 | 98.2 | YES |
| No.8 | 55 | M | 163.9 | 59.8 | 22.3 | 28 | 1 | 27 | 56 | 100 | YES |
| No.9 | 26 | M | 178.1 | 85.3 | 26.9 | 22 | 1 | 23 | 46 | 82.1 | YES |
| No.10 | 49 | M | 172.2 | 69.2 | 23.3 | 27 | 1 | 20 | 48 | 85.7 | YES |
| Total | - | - | - | - | - | 238 | 105 | 163 | 506 | - | - |
| Avg | 49.9 | - | - | - | 26.2 | - | - | - | - | 90.3 | 100 |
H, height; W, weight, BF, breakfast; LU, lunch; DNR, dinner.
Pre-, pre-intervention start date; post-, post-intervention end date.
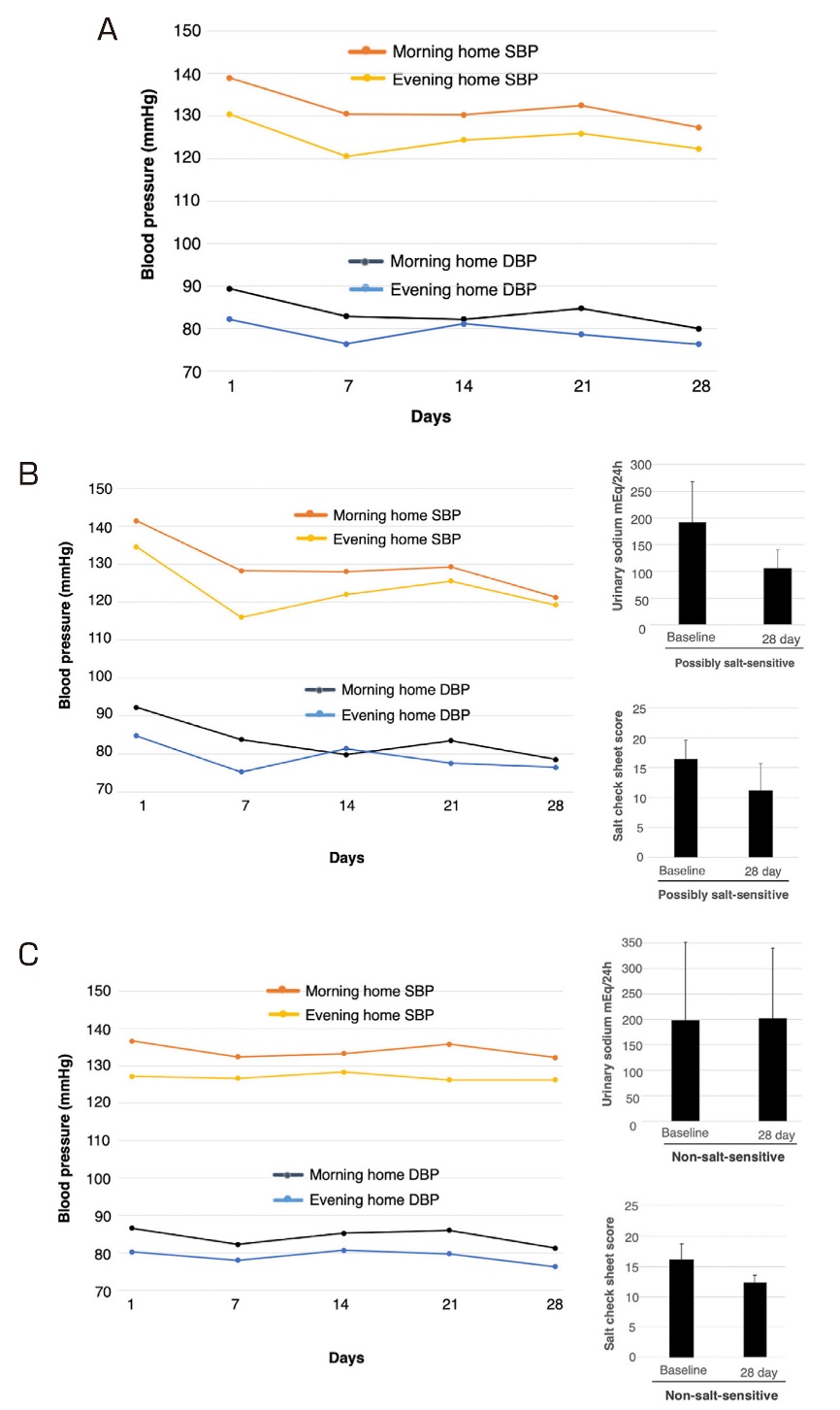
Changes in the average of morning and evening SBP and DBP during the intervention period. The subjects recorded their blood pressure measurements twice, each in the morning and evening, into the application, and the average value was automatically recorded. (A) Changes in all 10 subjects. Blood pressure readings in the evening are averages for nine subjects except No. 7. (B) The left panel shows the blood pressure trends of five subjects (No. 1, 2, 4, 5, and 8) who showed a downtrend in SBP with a reduction in 24-hour urinary sodium excretion before and after the intervention (Table 2 and the top right of this figure). The lower right of the figure shows the salt check score. (C) The left panel shows the blood pressure trends of the remaining five subjects (No. 3, 6, 7, 9, and 10) who showed neither a downtrend in SBP nor a reduction in the 24-hour urinary sodium excretion before and after the intervention (Table 3 and the top right of this figure). The lower right of the figure shows the salt check score. The blood pressure readings in the evening are averages for four subjects except No. 7.
|
Morning home SBP (mmHg) |
Evening home SBP (mmHg) |
24-h urinary salt excretion (mEq) |
Salt check sheet score | |||||
|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | Pre | Post | |
| No.1 | 136 | 107 | 144 | 119 | 174 | 117 | 16 | 7 |
| No.2 | 144 | 107 | 114 | 103 | 131.3 | 82.5 | 18 | 8 |
| No.3 | 145 | 142 | 111 | 119 | 142.2 | 77.7 | 19 | 12 |
| No.4 | 138 | 119 | 134 | 123 | 235.2 | 102 | 19 | 17 |
| No.5 | 138 | 122 | 127 | 117 | 300 | 157.5 | 18 | 15 |
| No.6 | 148 | 127 | 144 | 130 | 86.3 | 126 | 19 | 12 |
| No.7 | 133 | 136 | 130 | -a | 169.4 | 164.8 | 12 | 12 |
| No.8 | 151 | 137 | 133 | 124 | 118.8 | 67.5 | 11 | 9 |
| No.9 | 126 | 128 | 133 | 126 | 468 | 436.5 | 15 | 11 |
| No.10 | 131 | 128 | 118 | 134 | 123.8 | 200.2 | 13 | 14 |
| Avg | 139 | 125.3 | 128.8 | 121.7 | 194.9 | 153.2 | 16 | 11.7 |
aThe subject stopped measuring the evening blood pressure during the intervention study. Morning blood pressure measurements and food consumption were continued until the last day of the study.
Pre-, pre-intervention start date; post-, post-intervention end date.
It is noteworthy that all 10 subjects were able to continue eating two meals a day at home for 28 days. Thus, the continuity and usefulness of the novel salt reduction system was demonstrated. A major factor in their ability to continue eating is deemed to be the low-sodium system that allows them to easily create a diverse menu on their own. The low-sodium sauce, which is highly praised for its “delicious taste without tasting low-sodium” was developed by creatively using dashi, spices, and citrus fruits. For some ingredients, we worked with a local agricultural cooperative to use local seasonal vegetables. Potassium-rich vegetables (like broccoli) that are deformed and unsalable can also be cut, heated, and frozen for use in this salt reduction system, thereby contributing to the SDGs.
In this study, the criteria for continuity and usefulness were set at 40%, as described under Materials and Method. According to survey data from the Japan Frozen Food Association, only about 11% of respondents use frozen foods daily, which together with use frozen foods two to three times a week about 40% [6]. Collectively, we believe that a 40% decision criterion is reasonable, along with the time and effort required for daily application input, etc., as noted in the Methods section. For the above reasons, the subjects were asked to eat two out of three meals per day. Prior to the study, the subjects were instructed to avoid high-sodium meals for the remaining one meal as much as possible. Pre- and post-intervention salt checklist scores showed that subjects showed a behavioral change toward salt reduction.
In this study, all meals were provided to the subjects free of charge. Thus, it is undeniable that they may have been aware that they were being observed, or that they felt psychological pressure to eat as much low-sodium food as possible. Concerned about this, prior to the study, the subjects were told that they never had to force themselves to eat a low-sodium diet and that they could contact the health office at Izumo City Hall at any time to inform them of their intention to discontinue the study.
The habit of eating breakfast is involved in a lower risk of hypertension [7]. Furthermore, the relationship between missing breakfast and cardiometabolic risk is well known [8]. However, a typical Japanese breakfast (e.g., salted salmon fillet and miso soup) is high in salt. Therefore, we recommended the subjects to eat a low-sodium breakfast, resulting their feeding rate was as high as 47% (Table 1).
Interestingly, based on the results of the variation in SBP in all subjects, they might be divided into two groups [9, 10]. A downtrend in blood pressure was observed in one group of subjects with possible salt sensitivity (Fig. 3B, Table 2), but not in the other group (Fig. 3C, Table 2).
However, no clear definition or diagnostic criteria for salt-sensitive hypertension have been established. Therefore, it is not possible to know whether a patient is a salt-sensitive hypertensive type based on numerical values or other factors. In this study, it is necessary to consider the possibility that other factors besides salt reduction, such as lifestyle modification and weight loss, may be involved. As a limitation of this study, it should be stated that the study was conducted on a small sample size (n = 10) in a limited number of occupations. Because this is a single-arm pilot study designed to determine “the completion rate of a reduced-salt diet” (PRIMARY ENDPOINT) and not to examine changes in blood pressure before and after low-salt diet intervention, only descriptive statistics were included (approved research plan without statistical analysis). Due to the reasons mentioned above, there are limitations in the interpretation of the results for outcomes, such as blood pressure (secondary endpoint), and no control group was set. Notably, all subjects completed the program (consumption of two low-sodium meals per day, daily blood pressure measurement and application input, 24-hour urine collection at home, salt check sheet input, and questionnaire response), despite the fact that the evaluation criterion was set as “with continuity” when 40% of the participants completed the program. Although this study has a small sample size (n = 10), the results show the usefulness of this salt reduction system as it can be used at home without the intervention of a medical personnel during the study period (28 days). The effects of gender and age are still to be examined due to the limited number of the subjects. Based on the results of this pilot study, a larger-scale validation study (RCT) will be conducted in the near future. Moreover, the use of digital health applications for hypertension is expected [11, 12]. Furthermore, we have recently invented a new technology that combines this salt reduction system with machine learning to provide the optimal dietary pattern (personalized diet) for each disease state (patent pending). This technology will utilize data on the intestinal microflora of each individual [13].
Our results suggest that the “infinite recipe” salt reduction system is effective and useful to maintain a low-sodium diet.
Ethical approval
This study was conducted with the approval of by the Medical Research Ethics Committee, Shimane University Faculty of Medicine, (20160519-1: UMIN000049601).
Author contribution
M.N., E.M: study design, analysis, and interpretation of data.
Conflict of interest
M.N. holds stock of Mirai-Mugen-Recipe Inc. and is the inventor of Japanese Patent No. 6714238. E.M declares no competing interests.