Abstract
Polycystic ovary syndrome (PCOS) is one of major causes of irregular menstruation. It is defined as a condition involving the combination of hyperandrogenism and chronic oligomenorrhea or anovulation, and is thought to have a variety of etiologies. Insulin resistance (impaired insulin sensitivity) has been suggested to be one of the etiologies of PCOS. PCOS patients often need to take medication to treat anovulation and infertility. Therefore, it would be beneficial to patients if simple non-pharmacological treatments can be developed. Recently the efficacy of vinegar to improve insulin resistance has been reported. To study the effect of vinegar on metabolic and hormonal indices and ovulatory function in PCOS, seven patients seeking a non-pharmacological treatment for PCOS took a beverage containing 15 g of apple vinegar daily for 90 to 110 days. Ovulation, the menstrual interval, fasting serum glucose level, fasting serum insulin level, luteinizing hormone (LH), follicle stimulating hormone (FSH), and testosterone were compared before and after intake of the vinegar beverage. Intake of the vinegar beverage resulted in a decrease of the homeostasis model assessment insulin resistance index (HOMA-R) in six patients, as well as a decrease of the LH/FSH ratio in five of seven patients. Ovulatory menstruation was observed within 40 day in four of seven patients. These findings suggest the possibility of vinegar to restore ovulatory function through improving insulin sensitivity in PCOS patients, thus, avoiding pharmacological treatment. Intake of vinegar might reduce medical cost and treatment time for insulin resistance, anovulation, and infertility in patients with PCOS.
Introduction
Polycystic ovary syndrome (PCOS) is one of the major causes of irregular menstruation; it affects 4-8% of women of reproductive age (Knochenhauer et al. 1998; Diamanti-Kandarakis et al. 1999; Agrawal et al. 2004; Carmina and Azziz 2006). It is defined as a condition involving the combination of hyperandrogenism and chronic oligomenorrhea or anovulation, and is thought to have a variety of etiologies (Carmina and Azziz 2006; Fauser et al. 2012). Recently, Insulin resistance (impaired insulin sensitivity) has been suggested to be one of the features of PCOS. In addition, some genetic factors have been reported to contribute to both reproductive and metabolic abnormalities in PCOS. (Legro and Strauss 2002; Doi et al. 2005). However, the mechanisms underlying insulin resistance and reproductive anomalies in women with PCOS have not been clearly defined (Falcone et al. 1990; Sharp et al. 1991; Dewailly and Cortet-Rudelli 1992). The heterogeneity of PCOS makes it difficult to elucidate the mechanism. However, insulin resistance has been reported to be associated with a greater risk of anovulation in women with PCOS (Palomba et al. 2009a, 2009b). Therefore, this metabolic abnormality might be a key to ovulatory dysfunction in a portion of women with PCOS. To date, the optimal long-term management of PCOS has not been determined. One of the main aims of treatment for PCOS is to restore ovulation so that these women can conceive. Accordingly, insulin sensitizers have been used to promote ovulation and fertility in women with PCOS (Moghetti et al. 2000; Onalan et al. 2005; Eisenhardt et al. 2006).
The insulin sensitizer employed most often for the treatment of PCOS is metformin (dimethylbiguanide). Metformin is administered orally to lower the blood glucose level in patients with type 2 diabetes (Buse 1999; Bosi 2009), since it enhances the insulin sensitivity of both the liver and the peripheral tissues (Phielix et al. 2011). In addition, metformin was administered to 40 women with PCOS to increase insulin sensitivity and reduce the sequelae of hyperinsulinemia, with ovulation being achieved in 27 patients (Palomba et al. 2009a). Accordingly, metformin is commonly used to achieve ovulation in the patients with PCOS.
Vinegar is a common cooking ingredient. The most important component of vinegar is acetic acid together with small amounts of vitamins, mineral salts, and amino acids. Although vinegar is mainly used for cooking, it is considered to have several effects such as antibacterial (Entani et al. 1998; Sengun and Karapinar 2004), cardiovascular protection (Kondo et al. 2001; Honsho et al. 2005), and antitumor properties (Mimura et al. 2004; Nanda et al. 2004). Recent studies have shown that intake of vinegar with or after a meal can reduce the post-prandial glucose level (Johnston et al. 2004; Östman et al. 2005). Östman et al. (2005) reported that ingesting a meal with vinegar reduced the postprandial responses of blood glucose and insulin in 12 non-diabetic healthy volunteers. Although there was no significant effect of vinegar on postprandial glucose levels in type 2 diabetic patients, vinegar was found to improve insulin sensitivity during the initial 30-minute period after meals in subjects with insulin resistance (Johnston et al. 2004). These reports led to the hypothesis that vinegar might improve insulin sensitivity in women with PCOS who have normal insulin sensitivity or insulin resistance. Because patients easily consume vinegar, it might be useful as a non-pharmacological treatment for PCOS. In this study, therefore we assessed the influence of vinegar on hormonal indices and ovulation in women with PCOS. Our results suggest that vinegar intake restored ovulatory menstruation, together with a decrease of the LH/FSH ratio and improvement of insulin resistance, in women with PCOS.
Materials and Methods
The present study was approved by the Institutional Review Board of Shiga University of Medical Science. The purpose and procedures were carefully explained to all of the participants and written informed consent was obtained. Seven women aged 21 through 40 years old were enrolled. PCOS was diagnosed, according to the criteria of the Japanese Society of Obstetrics and Gynecology by the presence of the following three features: 1) oligomenorrhea or anovulation, that is, irregular menstruation; 2) polycystic ovaries, defined as the presence of more than 10 antral follicles in a ovary; and 3) clinical and/or biochemical evidence of hyperandrogenism, or biochemical evidence of both high LH and normal FSH after exclusion of related disorders. Exclusion criteria include congenital adrenal hyperplasia, Cushing’s syndrome, hyperprolactinemia, and thyroid dysfunction. Women with a history of glucose intolerance (including gestational diabetes) or type 2 diabetes were also excluded. Since acetic acid has a strong, distinct odor, the participants can distinguish whether the beverage includes acetic acid. Therefore, we could not design a case-control study using a different beverage that does not contain vinegar. Prior to starting vinegar intake, blood tests including LH, FSH, testosterone, fasting insulin, and fasting glucose were drawn from day 3 through day 5 of the menstrual cycle or at the quiescent phase when the largest follicle was < 10 mm in diameter, if that phase persisted for more than 30 days. The blood test was drawn on the morning after fasting for at least eight hours. The homeostasis model assessment of insulin resistance index (HOMA-R) was calculated by the formula: fasting serum glucose level × fasting serum insulin levels ÷ 405. Subsequently, 100 ml of a beverage containing 15 g of apple vinegar (MAINZ, Mizkan Co., Ltd., Handa, Japan) was ingested immediately after dinner daily for 90 to 110 days. The ingredient composition of the apple vinegar beverage is shown in Table 1. Basal body temperature (BBT) was checked and recorded in a similar notebook by each patient. In addition, each patient recorded the onset of menstruation and whether she consumed the vinegar beverage. All patients visited our hospital at least every 28 days and were examined by trans-vaginal or trans-abdominal ultrasonography at every visit. The BBT records were checked by doctors at every visit, and ovulation was diagnosed by two doctors individually. When the formation of a corpus luteum was confirmed by ultrasonography or the high phase, diagnosed when the BBT was at least 0.4°C higher than in the low phase, persisted for more than 10 days, the patient was defined as having ovulated. The interval between menstruations was calculated by reviewing the BBT record. On day 3 to day 5 of the menstrual cycle, after ingestion of the beverage for 90 to 110 days, blood tests were redrawn. When ovulation was not confirmed after taking the beverage for 90 days, blood tests were drawn and progestins were given to induce withdrawal bleeding. Because the data was not normally distributed, paired Wilcoxon nonparametric test was used to compare the results before versus after taking the apple vinegar beverage for at least 90 days.

Results
The ingredient composition of 100 ml of the beverage contains 15 g of apple vinegar (Table 1). The apple vinegar contains 5% (weight/weight) of acetic acid. Therefore, 100 ml of the beverage contains 750 mg of acetic acid. The profile of the patients, including age, gravidity, parity, body weight, height, body mass index, and menstrual status before intake of the apple vinegar, is shown in Table 2. Based on the body mass index, two of the seven patients were defined as obese and one was overweight. There were two patients with oligomenorrhea, three patients with amenorrhea, and two patients with anovulatory menstrual cycles. After the intake of apple vinegar, ovulatory menstruation was observed within 40 days in four of the seven patients (patients 1 to 4), including both of the obese patients (patient 1 and 2). Ovulatory menstruation took longer than 40 days in two of the patients (patients 5 and 6). No ovulatory menstruation was observed for 90 days in one patient (patient 7), who was treated by progestins. HOMA-R was obtained for only six of the seven patients. When compared to the level before vinegar intake, the HOMA-R decreased after intake of the beverage in all six of the patients; however, the difference was not significant difference (Fig. 1a). The LH/FSH ratio decreased in five of the seven patients, including all four patients who resumed ovulation within forty days (Fig. 1b). There was no change in the serum total testosterone level before and after taking the vinegar beverage (Fig. 1c).
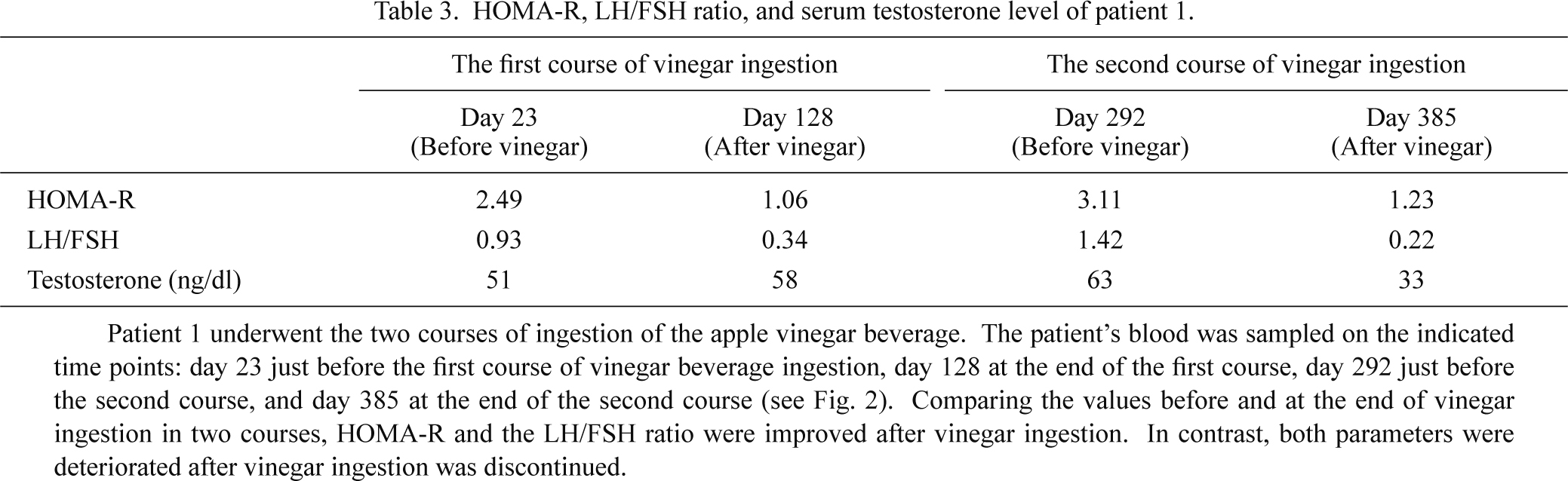
A typical patient with restored ovulation after the intake of the vinegar beverage (patient 1) is shown in Fig. 2 and Table 3. The patient ingested two courses of the apple vinegar beverage. Before starting intake of the beverage, she was oligomenorrheic with a menstrual interval that was usually longer than 50 days. The menstruation interval became shorter during and just after intake of the beverage in both the first and second courses and became longer again after she ceased ingesting the vinegar beverage (Fig. 2). Moreover, the LF/FSH ratio and HOMA-R were improved at the end of both courses. However, if compared the LH/FSH ratio and HOMA-R between the end of the first course on day 128 and before starting the second course on day 292, the metabolic and hormonal status were deteriorated after she ceased ingestion of apple vinegar for four months (Table 3). Furthermore, patient 3 had been infertile for two years. She ingested the vinegar beverage for another two months after regular intake for 90 days and became pregnant without any other treatment. These findings also suggest that vinegar has a role in the restoration of ovulatory function and the promotion of fecundity.


Discussion
For more than 2000 years, vinegar has been used to season and preserve foods, heal wounds, treat infections (Entani et al. 1998; Sengun and Karapinar 2004), prevent cardiovascular disease (Kondo et al. 2001; Honsho et al. 2005), and suppress tumor formation (Mimura et al. 2004; Nanda et al. 2004). It has been suggested that vinegar reduces the glucose response to a carbohydrate load in subjects with insulin resistance and healthy adults (Carol et al. 2004). Johnston and colleagues (2004) reported that subjects with insulin resistance or type 2 diabetes took a vinegar beverage (20 g of vinegar, 40 g of water, and 1 tsp of saccharine) or placebo before meals (87 g of total carbohydrate). In the insulin resistant subjects, ingestion of vinegar significantly reduced postprandial glycemia compared with placebo and improved postprandial insulin sensitivity by 34%. In the subjects with type 2 diabetes, vinegar ingestion was less effective for reducing glycemia; however, the difference was not statistically significant. Despite that finding, vinegar ingestion reduced postprandial glucose level by 19%; therefore, this negative outcome may have been due to the study size or variations of the effect on the glucose concentration. In addition, Östman et al. (2005) demonstrated that acetic acid reduced postprandial serum glucose levels and insulin levels in healthy subjects. These subjects took meals (50 g carbohydrate) alone or with 3 portions of a vinegar beverage containing 1.1, 1.4, or 1.7 g of acetic acid. All vinegar concentrations reduced postprandial glycemia compared with placebo. These findings suggest that vinegar improves insulin sensitivity and regulates blood glucose in healthy adults.
Although it still remains unclear how vinegar alters the glycemic response to a meal, several mechanisms have been proposed. Some investigators have examined whether delayed gastric emptying is related to the antiglycemic effect of vinegar. Liljeberg and Björck (1998) reported that vinegar significantly reduced the postprandial glucose and insulin responses to a starchy meal in healthy subjects and suggested that the mechanism was related to delayed gastric emptying as judged from lower paracetamol levels after the test meal with vinegar. Conversely, in rats fed experimental diets containing the indigestible marker polyethyleneglycol and various concentrations of acetic acid, dietary acetic acid did not alter gastric emptying, food intake, or glucose absorption (Fushimi et al. 2001). Thus, the effect of vinegar on gastric emptying is still controversial.
Another approach for investigating the effect of vinegar is to analyze the enzymes involved in glucose digestion or glucose metabolism. Ogawa et al. (2000) examined the effects of acetic acid and other organic acids on disaccharidase activity in CACO-2 human colon cancer cells. Disaccharidases are glycoside hydrolases, which are enzymes that break down disaccharides into monosaccharides, including sucrose, lactase, and maltase. They found that acetic acid suppressed sucrose, lactase, and maltase activity in a concentration- and time-dependent manner, while the other organic acids did not alter these enzyme activities; they found that acetic acid did not alter de novo synthesis of the sucrose-isomaltase complex at either the transcriptional or translational level. The investigators concluded that acetic acid’s suppressive effect probably occurs during posttranslational processing of the enzyme complex.
Vinegar has also been reported to increase the glucose-6-phosphate (G6P) concentration in skeletal muscle, just as metformin suppresses glucose-6-phospatase expression to increase the intracellular level of G6P and decrease serum glucose (Fushimi et al. 2001). G6P is utilized for glycolysis and the pentose phosphate pathway or is converted glycogen.
In addition, metformin has been reported to activate 5′-AMP-activated protein kinase (AMPK), an enzyme that plays an important role in insulin signaling, whole body energy balance, and the metabolism of glucose and fats (Towler and Hardie 2007). Sakakibara et al. (2006) revealed the efficacy of acetic acid on reducing fasting plasma glucose level and hemoglobin A1c by giving mice 0.3% acetic acid for 8 weeks. Acetic acid reduced the expression of genes involved in gluconeogenesis and lipogenesis, which is partially regulated by AMPK. They also reported that sodium acetate, in the form of neutralized AcOH, directly activated AMPK and lowered the expression of genes such as for glucose-6-phosphatase (Sakakibara et al. 2006). These results indicate that the hypoglycemic effect of AcOH might be due to activation of AMPK as well as the efficacy of metformin.
There have been no reports about a direct effect of vinegar or acetic acid on folliculogenesis and ovarian function; therefore, we could not determine how ovulatory function was restored in our PCOS patients by vinegar ingestion. However, we theorize that vinegar reduces insulin resistance by activating AMPK and suppressing glucose-6-phosphatase in the skeletal muscles and peripheral tissues of our PCOS patients. That is, vinegar improved ovarian function by regulating insulin resistance in the same way as metformin acts on PCOS.
Our study suggests that vinegar may be effective for obese PCOS patients and/or patients with PCOS and insulin resistance. In both obese patients (patients 1 and 2), ovulation was restored or the menstrual cycle was shortened. In patients 1 through 3, who responded well to the vinegar beverage, HOMA-R was decreased by more than 50%. These findings also suggest that vinegar acted through the improvement of insulin resistance.
Velazquez et al. (1994) first reported the efficacy of metformin on restoring menstrual cycles in amenorrheic women with PCOS. Subsequently, uncontrolled studies and randomized, controlled trials have evaluated the efficacy of metformin for improvement of menstruation (Moghetti et al. 2000; Palomba et al. 2009b). The results obtained from several uncontrolled studies have indicated that metformin is effective for restoring the menstrual cycle in approximately 62% of oligomenorrheic women with PCOS (Palomba et al. 2009b). In a randomized, double-blind, placebo-controlled study, the effect on menstrual irregularities after six months of metformin treatment was assessed in 23 PCOS patients (Moghetti et al. 2000). They showed that metformin produced a significant improvement of the menstrual cycle while no efficacy was observed for the placebo control and five women in the metformin group vs. none in the placebo group had their menstrual pattern substantially improved during treatment (Moghetti et al. 2000). More recently, a meta-analysis of insulin-sensitizing drugs showed that metformin could improve the menstrual pattern of PCOS patients (Tang et al. 2009). These findings suggest that metformin can be useful for the improvement of the ovulation rate. In our study, ovulation and a regular menstrual cycle were restored in four of seven patients; these benefits were comparable to that of metformin.
Vitamin C is an antioxidant. One hundred milliliters of the vinegar beverage contains 55 mg of vitamin C, which supplies more than half of the daily requirement, but not more than the total requirement, if considering that the total amount of vitamin C needed for a woman is 100 mg per day. Recently, antioxidant levels including vitamin C and E levels have been reported to be decreased in non-obese PCOS patient (Kurdoglu et al. 2012); however, there has been no report studying the efficacy of vitamin C for the treatment of PCOS. Therefore, the replacement of vitamin C cannot be denied to be a contributor to ovulation restoration in PCOS patients.
There has been one report regarding adverse reactions to vinegar (Carol and Cindy 2006). Aspiration of vinegar has been related to laryngospasm, resulting in subsequent vasovagal syncope. Also, inflammation of the oropharynx and second-degree caustic injury of the esophagus and cardia were observed in a 39-year-old woman who drank 1 tablespoon of rice vinegar. Her symptom resolved spontaneously after several days (Chung 2002). The odor and taste of vinegar are related to adverse effects; however, these symptoms resolve spontaneously. Esophageal injury due to vinegar appears to be rare; however, it merits attention. Although chronic inflammation of the esophagus is a cancer risk, vinegar is reported to be inversely associated with the risk of cancer of the esophagus (Xibib et al. 2003). These reports suggest that vinegar is safe at low concentrations. In our study, 100 ml of the apple vinegar beverage contained 750 mg of acetic acid and the sour taste was reduced at this concentration. None of the patients complained about the taste in this study.
Although the sample size of this study was small, it is hopefully sufficient to indicate the possibility of the ingestion of vinegar to improve insulin resistance, ovulatory function, and menstrual regularity in patients with PCOS. Intake of vinegar might reduce medical cost and the time needed to treat anovulation, infertility, and insulin resistance in patients with PCOS. To the best of our knowledge, this is the first report on the efficacy of vinegar for PCOS. Further studies are needed to confirm this efficacy.
Acknowledgements
The authors thank the Central Clinical Laboratory of Shiga University of Medical Science for serum analysis.
Conflict of Interest
We have no conflicting interest affecting the present study.
References
-
Agrawal,
R.,
Sharma,
S.,
Bekir,
J.,
Conway,
G.,
Bailey,
J.,
Balen,
A.H. &
Prelevic,
G.
(2004) Prevalence of polycystic ovaries and polycystic ovary syndrome in lesbian women compared with heterosexual women. Fertil. Steril., 82, 1352-1357.
-
Bosi,
E.
(2009) Metformin — the gold standard in type 2 diabetes: what does the evidence tell us? Diabetes Obes. Metab., 11, 3-8.
-
Buse,
J.B.
(1999) Overview of current therapeutic options in type 2 diabetes. Rationale for combining oral agents with insulin therapy. Diabetes Care, 22 Suppl 3, C65-C70.
-
Carol,
J.,
Cindy,
K. &
Amanda,
B.
(2004) Vinegar improves insulin sensitivity to a high-carbohydrate meal in subjects with insulin resistance or type 2 diabetes. Diabetes Care, 27, 281-282.
-
Carol,
J. &
Cindy,
G.
(2006) Vinegar: medicinal uses and antiglycemic effect. MedGenMed., 8, 61.
-
Carmina,
E. &
Azziz,
R.
(2006) Diagnosis, phenotype, and prevalence of polycystic ovary syndrome. Fertil. Steril., 86 Suppl 1, S7-S8.
-
Chung,
C.H.
(2002) Corrosive oesophageal injury following vinegar ingestion. Hong Kong Med J., 8, 365-366.
-
Dewailly,
D. &
Cortet-Rudelli,
C.
(1992) Insulin resistance and polycystic ovarian syndrome. Horm. Res., 38, 41-45.
-
Diamanti-Kandarakis,
E.,
Kouli,
C.R.,
Bergiele,
A.T.,
Filandra,
F.A.,
Tsianateli,
T.C.,
Spina,
G.G.,
Zapanti,
E.D. &
Bartzis,
M.I.
(1999) A survey of the polycystic ovarysyndrome in the Greek island of Lesbos: hormonal and metabolicprofile. J. Clin. Endocrinol. Metab., 84, 4006-4011.
-
Doi,
S.A.,
Al-Zaid,
M.,
Towers,
P.A.,
Scott,
C.J. &
Al-Shoumer,
K.A.
(2005) Ovarian steroids modulate neuroendocrine dysfunction in polycystic ovary syndrome. J. Endocrinol. Invest., 28, 882-892.
-
Eisenhardt,
S.,
Schwarzmann,
N.,
Henschel,
V.,
Germeyer,
A.,
von Wolff,
M.,
Hamann,
A. &
Strowitzki,
T.
(2006) Early effects of metformin in women with polycystic ovary syndrome: a prospective randomized, double-blind, placebo-controlled trial. J. Clin. Endocrinol. Metab., 91, 946-952.
-
Entani,
E.,
Asai,
M.,
Tsujihata,
S.,
Tsukamoto,
Y. &
Ohta,
M.
(1998) Antibacterial action of vinegar against food-borne pathogenic bacteria including Escherichia coli O157:H7. J. Food Prot., 61, 953-959.
-
Falcone,
T.,
Finegood,
D.T.,
Fantus,
I.G. &
Morris,
D.
(1990) Androgen response to endogenous insulin secretion during the frequently sampled intravenous glucose tolerance test in normal and hyperandrogenic women. J. Clin. Endocrinol. Metab., 71, 1653-1657.
-
Fauser,
B.C.,
Tarlatzis,
B.C.,
Rebar,
R.W.,
Legro,
R.S.,
Balen,
A.H.,
Lobo,
R.,
Carmina,
E.,
Chang,
J.,
Yildiz,
B.O.,
Laven,
J.S.,
Boivin,
J.,
Petraglia,
F.,
Wijeyeratne,
C.N.,
Norman,
R.J.,
Dunaif,
A.,
Franks,
S.,
Wild,
R.A.,
Dumesic,
D. &
Barnhart,
K.
(2012) Consensus on women's health aspects of polycystic ovary syndrome (PCOS): the Amsterdam ESHRE/ASRM-Sponsored 3rd PCOS Consensus Workshop Group. Fertil. Steril., 97, 28-38.
-
Fushimi,
T.,
Tayama,
K.,
Fukaya,
M.,
Kitakoshi,
K.,
Nakai,
N.,
Tsukamoto,
Y. &
Sato,
Y.
(2001) Acetic acid feeding enhances glycogen repletion in liver and skeletal muscle of rats. J. Nutr., 131, 1973-1977.
-
Honsho,
S.,
Sugiyama,
A.,
Takahara,
A.,
Satoh,
Y.,
Nakamura,
Y. &
Hashimoto,
K.
(2005) A red wine vinegar beverage can inhibit the renin-angiotensin system: experimental evidence in vivo. Biol. Pharm. Bull., 28, 1208-1210.
-
Johnston,
C.S.,
Kim,
C.M. &
Buller,
A.J.
(2004) Vinegar improved insulin sensitivity to a high-carbohydrate meal in subjects with insulin resistance or type 2 diabetes. Diabetes Care, 27, 281-282.
-
Knochenhauer,
E.S.,
Key,
T.J.,
Kahsar-Miller,
M.,
Waggoner,
W.,
Boots,
LR. &
Azziz,
R.
(1998) Prevalence of the polycystic ovary syndrome in unselected black and white women of the southeastern United States: a prospective study. J. Clin. Endocrinol. Metab., 83, 3078-3082.
-
Kondo,
S.,
Tayama,
K.,
Tsukamoto,
Y.,
Ikeda,
K. &
Yamori,
Y.
(2001) Antihypertensive effects of acetic acid and vinegar on spontaneously hypertensive rats. Biosci. Biotechnol. Biochem., 65, 2690-2694.
-
Kurdoglu,
Z.,
Ozkol,
H.,
Tuluce,
Y. &
Koyuncu,
I.
(2012) Oxidative status and its relation with insulin resistance in young non-obese women with polycystic ovary syndrome. J Endocrinol Invest., 35, 317-321.
-
Legro,
R.S. &
Strauss,
J.F.
(2002) Molecular progress in infertility: polycystic ovary syndrome. Fertil. Steril., 78, 569-576.
-
Liljeberg,
H. &
Björck,
I.
(1998) Delayed gastric emptying rate may explain improved glycaemia in healthy subjects to a starchy meal with added vinegar. Eur. J. Clin. Nutr., 52, 368-371.
-
Mimura,
A.,
Suzuki,
Y.,
Toshima,
Y.,
Yazaki,
S.,
Ohtsuki,
T.,
Ui,
S. &
Hyodoh,
F.
(2004) Induction of apoptosis in human leukemia cells by naturally fermented sugar cane vinegar (kibizu) of Amami Ohshima Island. Biofactors, 22, 93-97.
-
Moghetti,
P.,
Castello,
R.,
Negri,
C.,
Tosi,
F.,
Perrone,
F.,
Caputo,
M.,
Zanolin,
E. &
Muggeo,
M.
(2000) Metformin effects on clinical features, endocrine and metabolic profiles, and insulin sensitivity in polycystic ovary syndrome: a randomized, double-blind, placebo-controlled 6-month trial, followed by open, long-term clinical evaluation. J. Clin. Endocrinol. Metab., 85, 139-146.
-
Nanda,
K.,
Miyoshi,
N.,
Nakamura,
Y.,
Shimoji,
Y.,
Tamura,
Y.,
Nishikawa,
Y.,
Uenakai,
K.,
Kohno,
H. &
Tanaka,
T.
(2004) Extract of vinegar “Kurosu” from unpolished rice inhibits the proliferation of human cancer cells. J. Exp. Clin. Cancer Res., 23, 69-75.
-
Ogawa,
N.,
Satsu,
H.,
Watanabe,
H.,
Fukaya,
M.,
Tsukamoto,
Y.,
Miyamoto,
Y. &
Shimizu,
M.
(2000) Acetic acid suppresses the increase in disaccharidase activity that occurs during culture of caco-2 cells. J. Nutr., 130, 507-513.
-
Onalan,
G.,
Goktolga,
U.,
Ceyhan,
T.,
Bagis,
T.,
Onalan,
R. &
Pabuçcu,
R.
(2005) Predictive value of glucose-insulin ratio in PCOS and profile of women who will benefit from metformin therapy: obese, lean, hyper or normoinsulinemic? Eur. J. Obstet. Gynecol. Reprod. Biol., 123, 204-211.
-
Östman,
E.,
Granfeldt,
Y.,
Persson,
L. &
Björck,
I.
(2005) Vinegar supplementation lowers glucose and insulin responses and increases satiety after a bread meal in healthy subjects. Eur. J. Clin. Nutr., 59, 983-988.
-
Palomba,
S.,
Falbo,
A.,
Orio,
F. Jr.,
Tolino,
A. &
Zullo,
F.
(2009a) Efficacy predictors for metformin and clomiphene citrate treatment in anovulatory infertile patients with polycystic ovary syndrome. Fertil. Steril., 91, 2557-2567.
-
Palomba,
S.,
Falbo,
A.,
Zullo,
F. &
Orio,
F.
Jr. (2009b) Evidence-based and potential benefits of metformin in the polycystic ovary syndrome: a comprehensive review. Endocr. Rev., 30, 1-50.
-
Phielix,
E.,
Szendroedi,
J. &
Roden,
M.
(2011) The role of metformin and thiazolidinediones in the regulation of hepatic glucose metabolism and its clinical impact. Trends Pharmacol. Sci., 32, 607-616.
-
Sakakibara,
S.,
Yamauchi,
T.,
Oshima,
Y.,
Tsukamoto,
Y. &
Kadowaki,
T.
(2006) Acetic acid activates hepatic AMPK and reduces hyperglycemia in diabetic KK-A(y) mice. Biochem. Biophys. Res. Commun., 344, 597-604.
-
Sengun,
I.Y. &
Karapinar,
M.
(2004) Effectiveness of lemon juice, vinegar and their mixture in the elimination of Salmonella typhimurium on carrots (Daucus carota L.). Int. J. Food Microbiol., 96, 301-305.
-
Sharp,
P.S.,
Kiddy,
D.S.,
Reed,
M.J.,
Anyaoku,
V.,
Johnston,
D.G. &
Franks,
S.
(1991) Correlation of plasma insulin and insulin-like growth factor-I with indices of androgen transport and metabolism in women with polycystic ovary syndrome. Clin. Endocrinol. (Oxf.), 35, 253-257.
-
Tang,
T.,
Lord,
J.M.,
Norman,
R.J.,
Yasmin,
E. &
Balen,
A.H.
(2009) WITHDRAWN: Insulin-sensitising drugs for polycystic ovary syndrome. Cochrane Database Syst. Rev., 8, CD003053.
-
Towler,
M.C. &
Hardie,
D.G.
(2007) AMP-activated protein kinase in metabolic control and insulin signaling. Circ. Res., 100, 328-341.
-
Velazquez,
E.M.,
Mendoza,
S.,
Hamer,
T.,
Sosa,
F. &
Glueck,
C.J.
(1994) Metformin therapy in polycystic ovary syndrome reduces hyperinsulinemia, insulin resistance, hyperandrogenemia, and systolic blood pressure, while facilitating normal menses and pregnancy. Metabolism, 43, 647-654.
-
Xibib,
S.,
Meilan,
H.,
Moller,
H.,
Evans,
H.S.,
Dixin,
D.,
Wenjie,
D. &
Jianbang,
L.
(2003) Risk factors for oesophageal cancer in Linzhou, China: a case-control study. Asian Pac. J. Cancer Prev., 4, 119-124.