Abstract
Lung function is one of the strongest determinants of cardiopulmonary health and longevity. Long-term exposure to air pollution has been associated with decreased lung function. We undertook a retrospective study to compare the long-term consequences of air pollution in two areas of Japan: Mizushima, Okayama Prefecture and Kitakyushu, Fukuoka Prefecture. Industrialization began in Mizushima in the 1940s, whereas it began in Kitakyushu in the early 1900s. In Kitakyushu, levels of nitrogen dioxide have been higher compared to the Mizushima area. The subjects comprised 623 officially acknowledged victims of pollution-related illness (489 from Mizushima and 134 from Kitakyushu). All subjects were lifetime non-smokers and aged 65 years or older at the time of their last medical examination in 2009. Demographic data including diagnosed lung diseases and lung function at the time of certification assessment performed between 1973 and 1988 were obtained. The subjects from Kitakyushu were significantly younger (47.1 vs. 51.0 years, p < 0.001) and a higher percentage had asthma (91.2 vs. 36.8%, p < 0.001) compared to those from Mizushima. Furthermore, all measures of lung function were significantly lower in Kitakyushu group at the time of the certification assessment (p < 0.001) and at the follow-up (p < 0.001). However, no significant differences were observed in the annual mean decline in lung function between the two groups, despite the overall decrease in air pollution. In conclusion, the normal lung function is not restored even after improvement of air pollution. It is essential for every city to prevent air pollution.
Introduction
In recent years, the World Health Organization has warned about the danger of air pollution (http://www.who.int/mediacentre/factsheets/fs313/en/index.html). However, despite such warnings, the problem of air pollution has increased in developing countries. Long-term exposure to air pollutants, especially particulate air pollutants, has been reported to be associated with increased mortality (Dockery et al. 1993; Abbey et al. 1999; Hoek et al. 2002; Pope et al. 2002; Nafstad et al. 2004) and decreased lung function (Tashkin et al. 1994; Ackermann-Liebrich et al. 1997; Abbey et al. 1998; Sekine et al. 2004). Lung function is known to be one of the strongest determinants of cardiopulmonary health and longevity (Tockman et al. 1995; Hole et al. 1996; Mannino et al. 2003; Sin et al. 2005); however, the causal pathway underlying this relationship is poorly understood (Donaldson et al. 2001). Though the benefits to lung function of smoking cessation are well established (Fletcher and Peto 1977; Scanlon et al. 2000), few studies have investigated the effect of a reduction in air pollution on lung function (Abbey et al. 1998; Avol et al. 2001; Downs et al. 2007).
The Japanese economy underwent significant development and achieved high economic growth in the 1950s and 1960s. However, despite the economic growth, expenditure on social welfare remained low. As a result, a deterioration in the environment occurred, and there was an increase in the incidence of pollution-related illnesses. In conjunction with industrial development, air pollution became a problem, though the severity of the problem demonstrated great regional diversity.
In response to the increase in pollution-related illnesses, the Pollution-Related Health Damage Compensation Law was passed in 1973; this law provided that compensation be awarded to victims of air pollution. Although people whose health was seriously damaged as a result of air pollutants became officially designated as pollution victims, a few studies have examined the lung function of individuals with pollution-related illnesses (Mizushima-Kyodo General Hospital Group 2005; Guo et al. 2008). Though 40 years have passed since the above legislation, it has not been clearly demonstrated whether anti-pollution measures have had an effect on lung function. Furthermore, although it is acknowledged that the level of air pollution has an impact on lung function, no studies have investigated this issue.
The purpose of the present study was to analyze and compare the lung function of officially acknowledged victims of pollution-related illnesses in two areas in Japan with different histories of pollution. We aimed to determine the relationship between air-polluted environments and lung function.
Methods
Study areas and subjects
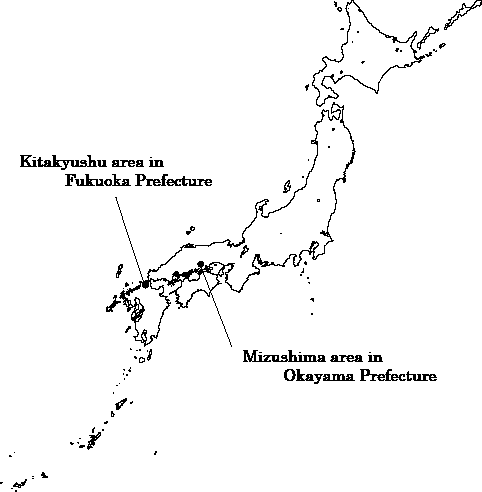
This was a retrospective, longitudinal, observational study. The subjects were officially acknowledged victims of pollution-related illnesses from two areas in Japan that have a research partnership with Nagasaki University. The areas were Mizushima in the city of Kurashiki, Okayama Prefecture, and the city of Kitakyushu in Fukuoka Prefecture, both of which undertook regular health surveys. The location of the two areas appears in Fig. 1. In all, 5,946 victims were considered for inclusion in this study. The victims had undergone regular health surveys since the pollution legislation was passed in 1973. Individuals aged 65 years or older at the time of their last medical examination in 2009 were enrolled in the study. To exclude the influence of cigarette smoking, we targeted only non-smokers and excluded all former or current smokers. This study was conducted using the records from medical examinations performed on the victims in Kurashiki and Kitakyushu for government certification for pollution-related illness from 1973 to 1988.
This study was approved by the Ethics Committee of Nagasaki University (approved number: 08072424-2).
Officially acknowledged victims of pollution-related illness
All registered victims met the following conditions, as determined by the Public Relief System of Kurashiki and Kitakyushu in accordance with the Pollution-Related Health Damage Special Measures Law (1969) and the Pollution-Related Health Damage Compensation Law (1973): (1) they resided or had spent time carrying out activities in an area specified as having significant air pollution (Table 1), and (2) they had been diagnosed with chronic bronchitis, asthma, or pulmonary emphysema by a respiratory physician. In accordance with the Public Nuisance Countermeasures Law (1967), the registered victims were entitled to various forms of compensation, including monthly consultation with a respiratory physician, prescriptions for expectorants and bronchodilators, and annual assessment of respiratory symptoms by means of a detailed questionnaire and lung function testing.
Air monitoring
Air pollution in Mizushima and Kitakyushu was measured according to the levels of four important pollutants: sulfur dioxide (SO2), nitrogen dioxide (NO2), carbon monoxide (CO), and suspended particulate matter (SPM). SPM is particulate matter with a diameter of 10 micrometers or less that is suspended in the atmosphere, and has been subject to environmental standards in Japan since 1972. The data were obtained from the air pollution office (comprising of a general environmental air measurement office and a motor exhaust measurement office), which is part of the public supervision system, in each district. The values of air pollution were measured at 21 sites in Mizushima (http://www.pref.okayama.jp/page/detail-4625.html) and at 19 sites in Kitakyushu (http://www.pref.fukuoka.lg.jp/c05/kankyohakusyo.html). These measurements reflect the average annual value for air pollution in each area.
Statistical analysis
Age, anthropometric data, diagnosed lung diseases, and lung function at the time of the certification assessment and at the last medical examination for each victim were used in the analysis. With regard to the annual mean change in lung function from 2000 to 2009, we determined a regression line for lung function that was continuously measured, and we computed the annual mean change in lung function as the coefficient of that regression line. The annual mean change was calculated only for those victims who underwent follow-ups for at least 7 times of examination.
We compared the above data for the two groups of victims from Mizushima and Kitakyushu. For statistical analysis, the two-sample t test, chi-square test, and Mann-Whitney U test were used after determining normality with the Kolmogorov-Smirnov test. All analyses were performed using the PASW software package version 18.0 (SPSS, Japan Inc., Tokyo, Japan), and differences were considered statistically significant when the two-tailed p value was < 0.05.
Results
The average annual values of the air pollutants in the two areas are shown in Fig. 2. No significant differences were observed between the two areas in terms of SO2 or CO levels. Since the 1980s, Kitakyushu showed higher annual average NO2 values than those observed in Mizushima. SPM levels in Mizushima have not been measured since the 1980s, so it was not possible to make a comparison of such data.
In all, 623 officially acknowledged victims of pollution-related illness were finally included in the study (Mizushima, 489 victims and Kitakyushu, 134 victims). Fig. 3 shows a flow chart of the study subjects. Victims with incomplete data for lung function were excluded from the study.
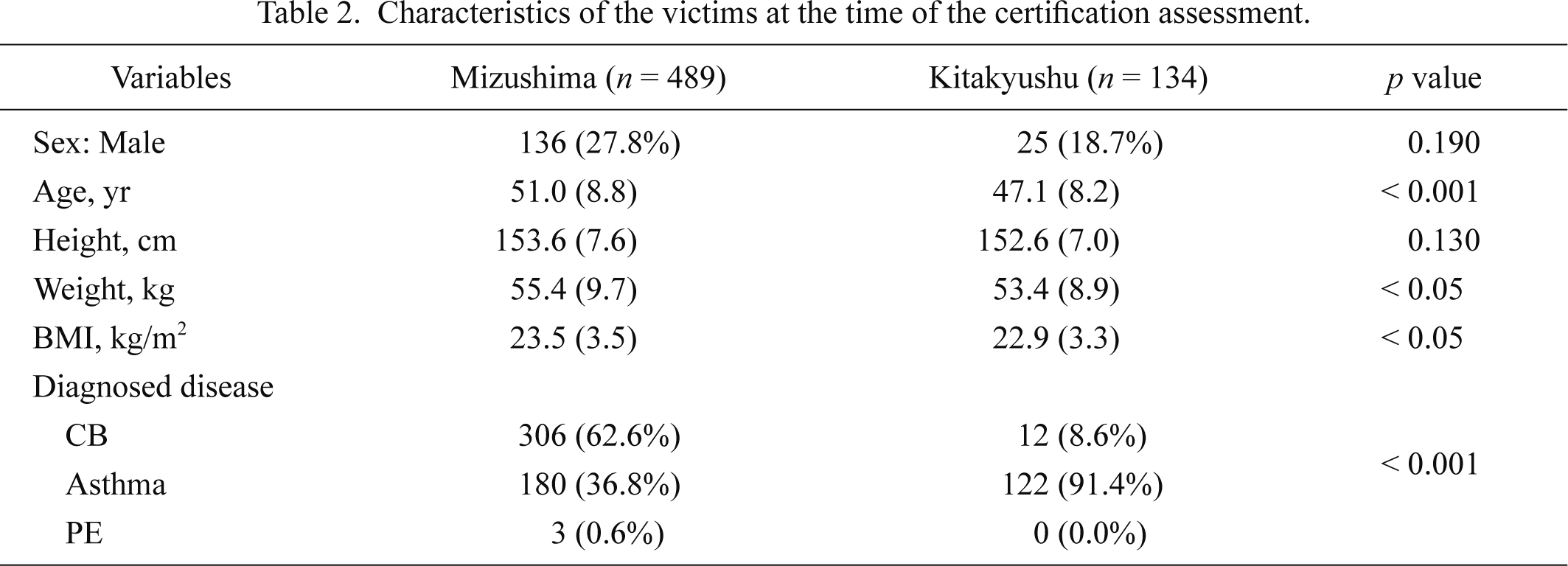
The characteristics of each victim at the time of the certification assessment are shown in Table 2. Significant differences were observed in age, weight, body mass index, and diagnosed diseases between the two groups. The victims in the Kitakyushu group were younger than those in the Mizushima group.
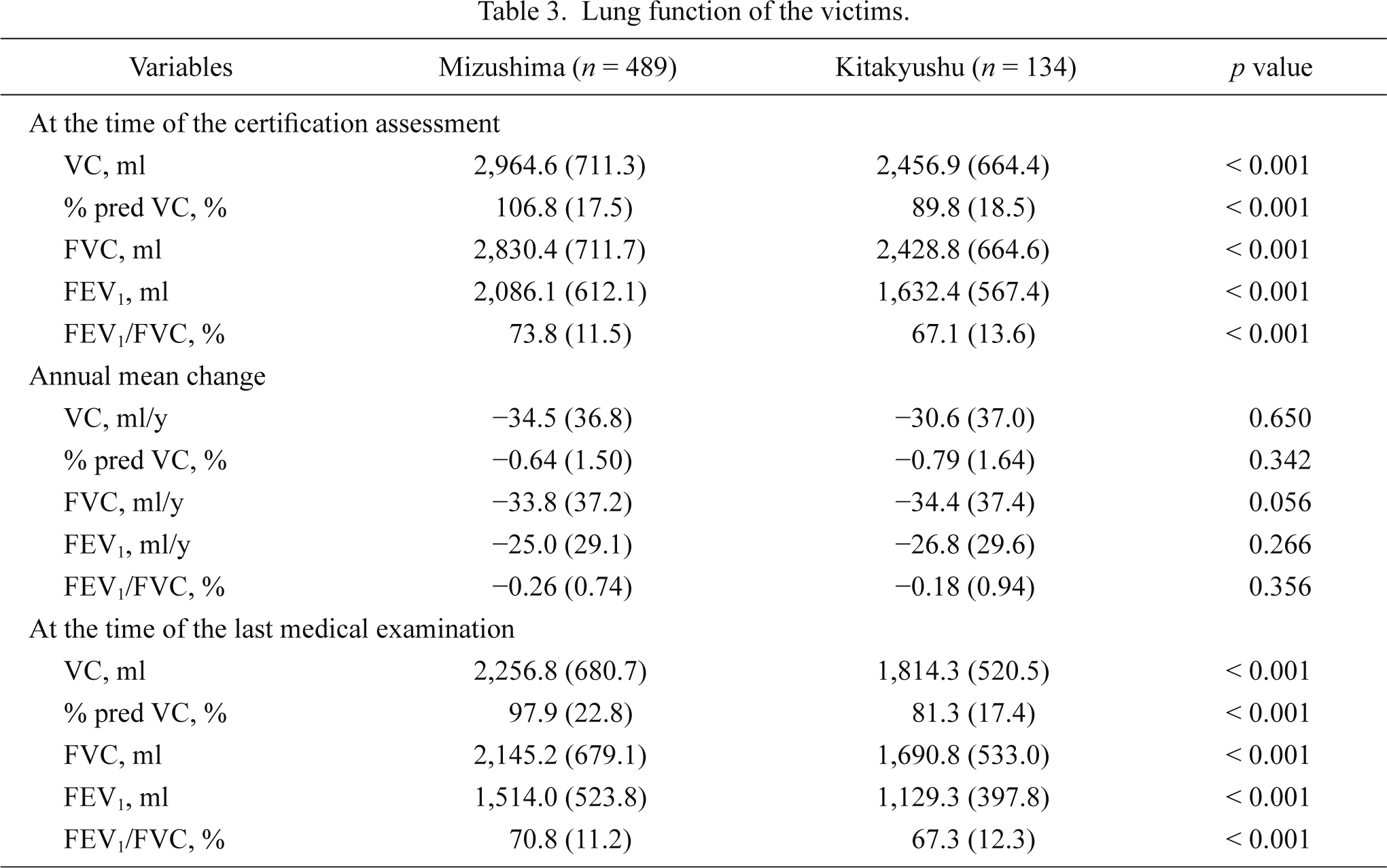
Data regarding lung function are presented in Table 3. Significant differences were observed between the two groups for all measures of lung function at the time of the certification assessment (p < 0.001). The Kitakyushu group showed significantly lower lung function values than the Mizushima group.
No significant differences were recorded in the annual mean change in lung function between the two groups (Table 3). Significant differences were found between the two groups for all measures of lung function at the time of the last medical examination (p < 0.001). The Kitakyushu group showed significantly lower lung function values than the Mizushima group in 2009.
Lung function decreased in both groups from at the time of the certification assessment to at the time of the last medical examination (Mizushima; VC, −34.5 ml/year and FEV1, −25.0 ml/year, and Kitakyushu; VC, −30.6 ml / year and FEV1, −26.8 ml/year).
Discussion
In this study, we analyzed lung function from designated victims of air pollution from two areas in Japan (Mizushima and Kitakyushu). Significant differences were observed in age, diagnosed lung diseases, and lung function between the two groups. Specifically, officially acknowledged victims of pollution-related illness in Kitakyushu were younger and the proportion of individuals with asthma was higher than in Mizushima. Moreover, all the victims showed low values of lung function at the time of certification assessment.
The difference in findings between the two groups of victims may be attributed to differences in air pollution between the two areas. We found that the only air pollutant that differed between the two areas was NO2. NO2 is a harmful air pollutant, and several reports have discussed its adverse effects on the respiratory system (Cooper and Tabershaw 1966; Shy et al. 1970a, b; Goldstein 1971). Some reports suggest an association between level of NO2 in the air and the incidence of asthma (Shima et al. 2002, 2003; Penard-Morand et al. 2005; Jacquemin et al. 2009), which might explain the large number of victims with asthma in Kitakyushu. Other reports have indicated that the level of NO2 in the air is significantly correlated with decreased lung function (Schwartz 1989; Martin et al. 1997; Peters et al. 1999; Gauderman et al. 2004). In our study, a high concentration of NO2 was associated with poorer lung function as measured at the time of the certification assessment in the victims residing in Kitakyushu.
It is also possible that the differences between the two groups may be due to different histories of pollution. Industrialization began in Mizushima in the 1940s, whereas it began in Kitakyushu in the early 1900s, some 40 years earlier. Additionally, at the time of the certification assessment in the 1970s, the victims were on average in their 40s and 50s; exposure to environmental air pollution in their youth and differences in exposure periods may have contributed to the findings. However, although earlier studies have examined levels of exposure to air pollutants (Martin et al. 1997; Peters et al. 1999; Gauderman et al. 2004), no reports have investigated exposure periods. Further study on this issue is thus required.
In the current study, there was no significant difference in the annual rate of decline in lung function between the two groups. Furthermore, the magnitude of the reduction in lung function in FVC and VC in this study was within the previously reported ranges for healthy, non-smoking males and females. (Yokoyama and Mitsulfuji 1972; Nakadate et al. 1994, Nakadate 1997). The levels of all air pollutants have been decreasing since the 1970s, and they returned to the normal range in the 1980s (Fig. 2). After the enactment of the Pollution-Related Health Damage Compensation Law in 1973, the Ministry of the Environment and the Environmental Disputes Coordination Commission undertook measures to reduce environmental pollution. It is believed that those measures reduced the levels of air pollutants in the country. However, the present study focused on the effect of alleviating air pollution on lung function. Only one report has demonstrated an improvement in forced vital capacity in response to a reduction in air pollution (Frye et al. 2003). Thus, the effects of air pollution on lung function may be small in our sample. It is difficult to conclude that improvements in air pollution alone are responsible for preventing a decrease in lung function.
In Japan, compensation for designated pollution victims was authorized by the Pollution-Related Health Damage Compensation Law, which imposed a protocol consisting of periodic hospital consultations for designated pollution victims. Because various measures were taken to reduce air pollution after the compensation law was passed, it is likely that the decrease in lung function of designated pollution victims was due to aging. Additionally, the development of new medications to treat respiratory ailments since the 1970s is another factor that may influence the findings. However, despite the improvement of air pollution, the lung function was not recovered.
This study analyzed the relationship between air pollution and lung function in designated pollution victims in two areas of Japan. Differences in lung function and diagnosed lung diseases between the two areas were observed as a result of different air pollution environments and different pollution histories. As a result of anti-pollution measures, there was an overall decrease in the degree of air pollution. However, the normal lung function is not restored in the two areas. Thus, we should not cause air pollution.
In the future, developing countries, which experienced industrialization after Western countries, will generate large-scale pollution similar to that previously produced in Japan. The measures to reduce pollution in Japan should therefore serve as an appropriate model for other pollution-generating countries.
The limitations of this study include the fact that we were unable to make a comparison with a control group.
Conclusions
We consider that differences in the levels of air pollutants and the duration of pollution between Mizushima and Kitakyushu resulted in differences among the victims with regard to lung function and diagnosed lung diseases. As a result of anti-pollution measures, there was an overall decrease in air pollution. However, the normal lung function is not restored in the two areas.
Acknowledgements
The project was funded by the Environmental Restoration and Conservation Agency of Japan. We thank the study participants, technical staff, the administrative support team, and co-workers for their help. This study was supported by the Foundation for Environmental Rehabilitation and Redevelopment of Mizushima, the City of Kitakyushu and Mizushima-Kyodo Hospital.
Conflict of Interest
The authors declare that they have no competing interests.
References
-
Abbey,
D.E.,
Burchette,
R.J.,
Knutsen,
S.F.,
McDonnell,
W.F.,
Lebowitz,
M.D. &
Enright,
P.L.
(1998) Long-term particulate and other air pollutants and lung function in nonsmokers. Am. J. Respir. Crit. Care Med., 158, 289-298.
-
Abbey,
D.E.,
Nishino,
N.,
McDonnell,
W.F.,
Burchette,
R.J.,
Knutsen,
S.F.,
Lawrence Beeson,
W. &
Yang,
J.X.
(1999) Long-term inhalable particles and other air pollutants related to mortality in nonsmokers. Am. J. Respir. Crit. Care Med., 159, 373-382.
-
Ackermann-Liebrich,
U.,
Leuenberger,
P.,
Schwartz,
J.,
Schindler,
C.,
Monn,
C.,
Bolognini,
G.,
Bongard,
J.P.,
Brandli,
O.,
Domenighetti,
G.,
Elsasser,
S.,
Grize,
L.,
Karrer,
W.,
Keller,
R.,
Keller-Wossidlo,
H.,
Kunzli,
N.,
Martin,
B.W.,
Medici,
T.C.,
Perruchoud,
A.P.,
Schoni,
M.H.,
Tschopp,
J.M.,
Villiger,
B.,
Wuthrich,
B.,
Zellweger,
J.P. &
Zemp,
E.
(1997) Lung function and long term exposure to air pollutants in Switzerland. Study on Air Pollution and Lung Diseases in Adults (SAPALDIA) Team. Am. J. Respir. Crit. Care Med., 155, 122-129.
-
Avol,
E.L.,
Gauderman,
W.J.,
Tan,
S.M.,
London,
S.J. &
Peters,
J.M.
(2001) Respiratory effects of relocating to areas of differing air pollution levels. Am. J. Respir. Crit. Care Med., 164, 2067-2072.
-
Cooper,
W.C. &
Tabershaw,
I.R.
(1966) Biologic effects of nitrogen dioxide in relation to air quality standards. Arch. Environ. Health, 12, 522-530.
-
Dockery,
D.W.,
Pope,
C.A. 3rd.,
Xu,
X.,
Spengler,
J.D.,
Ware,
J.H.,
Fay,
M.E.,
Ferris,
B.G. Jr. &
Speizer,
F.E.
(1993) An association between air pollution and mortality in six U.S. cities. N. Engl. J. Med., 329, 1753-1759.
-
Donaldson,
K.,
Stone,
V.,
Seaton,
A. &
MacNee,
W.
(2001) Ambient particle inhalation and the cardiovascular system: potential mechanisms. Environ. Health Perspect., 109 Suppl 4, 523-527.
-
Downs,
S.H.,
Schindler,
C.,
Liu,
L.J.,
Keidel,
D.,
Bayer-Oglesby,
L.,
Brutsche,
M.H.,
Gerbase,
M.W.,
Keller,
R.,
Kunzli,
N.,
Leuenberger,
P.,
Probst-Hensch,
N.M.,
Tschopp,
J.M.,
Zellweger,
J.P.,
Rochat,
T.,
Schwartz,
J. &
Ackermann-Liebrich,
U.
(2007) Reduced exposure to PM10 and attenuated age-related decline in lung function. N. Engl. J. Med., 357, 2338-2347.
-
Fletcher,
C. &
Peto,
R.
(1977) The natural history of chronic airflow obstruction. Br. Med. J., 1, 1645-1648.
-
Frye,
C.,
Hoelscher,
B.,
Cyrys,
J.,
Wjst,
M.,
Wichmann,
H.E. &
Heinrich,
J.
(2003) Association of lung function with declining ambient air pollution. Environ. Health Perspect., 111, 383-387.
-
Fukuoka prefecture. State of enviranment of Fukuoka prefecture.
http://www.pref.fukuoka.lg.jp/c05/kankyohakusyo.html [Accessed: March 29, 2013].
-
Gauderman,
W.J.,
Avol,
E.,
Gilliland,
F.,
Vora,
H.,
Thomas,
D.,
Berhane,
K.,
McConnell,
R.,
Kuenzli,
N.,
Lurmann,
F.,
Rappaport,
E.,
Margolis,
H.,
Bates,
D. &
Peters,
J.
(2004) The effect of air pollution on lung development from 10 to 18 years of age. N. Engl. J. Med., 351, 1057-1067.
-
Goldstein,
E.
(1971) Evaluation of the role of nitrogen dioxide in the development of respiratory diseases in man. Calif. Med., 115, 21-27.
-
Guo,
P.,
Yokoyama,
K.,
Suenaga,
M. &
Kida,
H.
(2008) Mortality and life expectancy of Yokkaichi Asthma patients, Japan: Late effects of air pollution in 1960-70s. Environ. Health: a global access science source., 7, 8.
-
Hoek,
G.,
Brunekreef,
B.,
Goldbohm,
S.,
Fischer,
P. &
van den Brandt,
P.A.
(2002) Association between mortality and indicators of traffic-related air pollution in the Netherlands: a cohort study. Lancet, 360, 1203-1209.
-
Hole,
D.J.,
Watt,
G.C.,
Davey-Smith,
G.,
Hart,
C.L.,
Gillis,
C.R. &
Hawthorne,
V.M.
(1996) Impaired lung function and mortality risk in men and women: findings from the Renfrew and Paisley prospective population study. BMJ, 313, 711-715; discussion 715-716.
-
Jacquemin,
B.,
Sunyer,
J.,
Forsberg,
B.,
Aguilera,
I.,
Briggs,
D.,
Garcia-Esteban,
R.,
Gotschi,
T.,
Heinrich,
J.,
Jarvholm,
B.,
Jarvis,
D.,
Vienneau,
D. &
Kunzli,
N.
(2009) Home outdoor NO2 and new onset of self-reported asthma in adults. Epidemiology, 20, 119-126.
-
Mannino,
D.M.,
Buist,
A.S.,
Petty,
T.L.,
Enright,
P.L. &
Redd,
S.C.
(2003) Lung function and mortality in the United States: data from the First National Health and Nutrition Examination Survey follow up study. Thorax, 58, 388-393.
-
Martin,
B.W.,
Ackermann-Liebrich,
U.,
Leuenberger,
P.,
Kunzli,
N.,
Stutz,
E.Z.,
Keller,
R.,
Zellweger,
J.P.,
Wuthrich,
B.,
Monn,
C.,
Blaser,
K.,
Bolognini,
G.,
Bongard,
J.P.,
Brandli,
O.,
Braun,
P.,
Defila,
C.
& et al.
(1997) SAPALDIA: methods and participation in the cross-sectional part of the Swiss Study on Air Pollution and Lung Diseases in Adults. Soz. Praventivmed., 42, 67-84.
-
Mizushima-Kyodo General Hospital Group.
(2005) Research on the deceased victims of air pollution., Mizushima Zaidan, Kurashiki.
-
Nafstad,
P.,
Haheim,
L.L.,
Wisloff,
T.,
Gram,
F.,
Oftedal,
B.,
Holme,
I.,
Hjermann,
I. &
Leren,
P.
(2004) Urban air pollution and mortality in a cohort of Norwegian men. Environ. Health Perspect., 112, 610-615.
-
Nakadate,
T.,
Sato,
T. &
Kagawa,
J.
(1994) Longitudinal changes in time domain spirogram indices and their variability. Eur. Respir. J., 7, 1062-1069.
-
Nakadate,
T.
(1997) Age-related decline in forced expiratory volume in one second and forced vital capacity based on a longitudinal observation of Japanese males. Nihon Kyobu Shikkan Gakkai Zasshi, 35, 954-959.
-
Okayama prefecture. State of enviranment of Okayama prefecture.
http://www.pref.okayama.jp/page/detail-4625.html [Accessed: March 29, 2013].
-
Penard-Morand,
C.,
Charpin,
D.,
Raherison,
C.,
Kopferschmitt,
C.,
Caillaud,
D.,
Lavaud,
F. &
Annesi-Maesano,
I.
(2005) Long-term exposure to background air pollution related to respiratory and allergic health in schoolchildren. Clin. Exp. Allergy, 35, 1279-1287.
-
Peters,
J.M.,
Avol,
E.,
Navidi,
W.,
London,
S.J.,
Gauderman,
W.J.,
Lurmann,
F.,
Linn,
W.S.,
Margolis,
H.,
Rappaport,
E.,
Gong,
H. &
Thomas,
D.C.
(1999) A study of twelve Southern California communities with differing levels and types of air pollution. I. Prevalence of respiratory morbidity. Am. J. Respir. Crit. Care Med., 159, 760-767.
-
Pope,
C.A. 3rd.,
Burnett,
R.T.,
Thun,
M.J.,
Calle,
E.E.,
Krewski,
D.,
Ito,
K. &
Thurston,
G.D.
(2002) Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. JAMA, 287, 1132-1141.
-
Scanlon,
P.D.,
Connett,
J.E.,
Waller,
L.A.,
Altose,
M.D.,
Bailey,
W.C. &
Buist,
A.S.
(2000) Smoking cessation and lung function in mild-to-moderate chronic obstructive pulmonary disease. The Lung Health Study. Am. J. Respir. Crit. Care Med., 161, 381-390.
-
Schwartz,
J.
(1989) Lung function and chronic exposure to air pollution: a cross-sectional analysis of NHANES II. Environ. Res., 50, 309-321.
-
Sekine,
K.,
Shima,
M.,
Nitta,
Y. &
Adachi,
M.
(2004) Long term effects of exposure to automobile exhaust on the pulmonary function of female adults in Tokyo, Japan. Occup. Environ. Med., 61, 350-357.
-
Shima,
M.,
Nitta,
Y.,
Ando,
M. &
Adachi,
M.
(2002) Effects of air pollution on the prevalence and incidence of asthma in children. Arch. Environ. Health, 57, 529-535.
-
Shima,
M.,
Nitta,
Y. &
Adachi,
M.
(2003) Traffic-related air pollution and respiratory symptoms in children living along trunk roads in Chiba Prefecture, Japan. J. Epidemiol., 13, 108-119.
-
Shy,
C.M.,
Creason,
J.P.,
Pearlman,
M.E.,
McClain,
K.E.,
Benson,
F.B. &
Young,
M.M.
(1970a) The Chattanooga school children study: effects of community exposure to nitrogen dioxide. 1. Methods, description of pollutant exposure, and results of ventilatory function testing. J. Air Pollut. Control Assoc., 20, 539-545.
-
Shy,
C.M.,
Creason,
J.P.,
Pearlman,
M.E.,
McClain,
K.E.,
Benson,
F.B. &
Young,
M.M.
(1970b) The Chattanooga school children study: effects of community exposure to nitrogen dioxide. II. Incidence of acute respiratory illness. J. Air Pollut. Control Assoc., 20, 582-588.
-
Sin,
D.D.,
Wu,
L. &
Man,
S.F.
(2005) The relationship between reduced lung function and cardiovascular mortality: a population-based study and a systematic review of the literature. Chest, 127, 1952-1959.
-
Tashkin,
D.P.,
Detels,
R.,
Simmons,
M.,
Liu,
H.,
Coulson,
A.H.,
Sayre,
J. &
Rokaw,
S.
(1994) The UCLA population studies of chronic obstructive respiratory disease: XI. Impact of air pollution and smoking on annual change in forced expiratory volume in one second. Am. J. Respir. Crit. Care Med., 149, 1209-1217.
-
Tockman,
M.S.,
Pearson,
J.D.,
Fleg,
J.L.,
Metter,
E.J.,
Kao,
S.Y.,
Rampal,
K.G.,
Cruise,
L.J. &
Fozard,
J.L.
(1995) Rapid decline in FEV1. A new risk factor for coronary heart disease mortality. Am. J. Respir. Crit. Care Med., 151, 390-398.
-
World Health Organization. Air quality and health.
[Cited: September, 2011]. http://www.who.int/mediacentre/factsheets/fs313/en/index.html [Accessed: March 29, 2013].
-
Yokoyama,
T. &
Mitsulfuji,
M.
(1972) Statistical representation of the ventilatory capacity of 2,247 healthy Japanese adults. Chest, 61, 655-661.