Abstract
Improving maternal health is a Millennium Development Goal adopted at the 2000 Millennium Summit of the United Nations. As part of the improving maternal health in Tanzania, it has been recommended that skilled birth attendants be present at all births to help reduce the high maternal mortality ratio. However, utilization of these attendants varies across socio-economic groups. The government of Tanzania has repeatedly attempted to carry out health sector reforms (HSRs) to alleviate disparities in health service utilization. In particular, around 1999, HSRs were incorporated into two approaches, including Decentralization by Devolution and Sector Wide Approach. This study aims to clarify the unresolved questions with little published evidence on the effect of HSRs on reducing disparities in utilization of skilled birth attendants across socio-economic groups over time. We used four cross-sectional datasets from the Tanzania Demographic and Health Survey: 1992, 1996, 1999, and 2004/05. Subjects included 14,752 women of reproductive age (15-49 years) and data on the most recent birth in the 5 years before each survey. Logistic regression analysis was performed with the dependent variable of whether respondents utilized skilled birth attendants or not, and with the main independent variables of time and socio-economic group. Results showed that the disparity in utilization of skilled birth attendants was significantly decreased from 1999 to 2004/05. These findings suggest that the two strategies, Decentralization by Devolution and Sector Wide Approach, in the process of HSRs are effective in reducing the disparities in utilization of skilled birth attendants among socio-economic groups.
Introduction
Improving maternal health is one of eight Millennium Development Goals (MDGs) adopted at the 2000 Millennium Summit of the United Nations; this goal was designed to accelerate a global reduction in maternal mortality and improve universal access to reproductive health by 2015 [World Health Organization (WHO) 2004]. In 2010, an estimated 287,000 maternal deaths occurred globally; 245,000 of these deaths (85%) occurred in Sub-Saharan Africa and South Asia. In 2010, 10 countries, including Tanzania, were reported to account for 60% of all maternal deaths worldwide (WHO; UNICEF; UNFPA and World Bank 2012).
According to the Tanzania Demographic and Health Survey (TDHS), the maternal mortality ratio in 2010 was estimated at 454/100,000 live births, which was lower than the maternal mortality ratio of 578/100,000 live births in 2004/05 (National Bureau of Statistics Tanzania and ICF Macro 2011). This most recent estimate, however, is still unacceptably higher than the ratio of 300/100,000 live births listed by the WHO (WHO; UNICEF; UNFPA and World Bank 2012).
Based on available knowledge, most of these maternal deaths could be avoided (Mpembeni et al. 2007). WHO recommends a number of essential interventions that can improve maternal health during the antenatal, childbirth, and postnatal periods (WHO 2009). Appropriate case management and referral, and effective emergency obstetric care in the first hours and days after childbirth could prevent most maternal deaths, caused by pregnancy-related complications. Therefore, it has been recommended that skilled birth attendants attend all births (WHO 2010).
Disparity in maternal healthcare coverage is a probable cause of the low utilization of maternal healthcare services in some areas. However, by reviewing 54 countries, Barros et al. (2012) demonstrated that skilled birth attendants were the least equitably utilized service in maternal healthcare plans and thus require special attention. Therefore, addressing the poor-rich disparity in healthcare is critical to attaining this MDG (Houweling et al. 2007). In addition, health sector reforms (HSRs) may help a deteriorating health system increase utilization of health services and improve health outcomes for the underprivileged population (Pariyo et al. 2009).
Health sector reforms in Tanzania
In 1994, the government of Tanzania proposed the most recent wave of HSRs to help both restore the deteriorated healthcare system and secure financial resources for healthcare. In the past, the government of Tanzania adopted the socialism policy in the 1960s and had provided free medical care for all under the principle of universal coverage through a centralized healthcare system. Private for-profit healthcare organizations were banned, and numerous public health facilities were established (Ministry of Health 1996). In the early 1980s, the policies were changed from centralization to decentralization as the former policies failed in service delivery (Munga et al. 2009). In addition, because Tanzania had a huge financial deficit and heavy debts, economic liberalization measures were pushed for and adopted starting in the late 1980s. In other words, free market mechanisms were introduced (Tax 2000). However, the decentralized healthcare system did not function well due to a sharp reduction in the number of civil servants in local governments that resulted from the economic liberalization measures. Concurrently, private for-profit medical and dental practices were re-instituted in 1991, and user fees were introduced in government health facilities starting in 1993 (Ministry of Health 1996).
In addition to aiming to empower local councils to develop health sector plans and further diversify the sources of healthcare financing by decentralization, the proposal for HSR aimed to improve universal access to healthcare, especially for vulnerable groups and the poor (Ministry of Health 1994). This proposal was implemented in the HSR Plan of Action 1996-1999 and the HSR Programme of Work 1999-2002 (Burki 2001). The former plan focused on developing new financial sources such as a Community Health Fund (CHF) and health insurance (Ministry of Health 1996). A CHF was implemented at one pilot district in 1996, and this program spread to 10 districts by 1999. Those who paid the CHF fees for their household members were entitled to a basic healthcare package as defined by each district. In principle, those who could not afford to pay were exempt from paying the CHF fees (Mtei and Mulligan 2007). In addition, private insurance services emerged in the mid to late 1990s and covered enrollees from private firms, and non-governmental and not-for-profit organizations established micro-insurance schemes for community members in the latter half of the 1990s (Haazen 2012).
In 1999, the latter program, the HSR Plan of Action 1996-1999, was begun. In the same year, the approach of Poverty Reduction Strategy Paper (PRSP) was initiated by the World Bank, which had continued to provide development aid to developing countries and attempt to reduce poverty around the world. The past relatively short-term approaches to reduce poverty were shifted into medium and long-term approaches to attaining MDGs. Naturally, the PRSPs aimed to reduce the maternal mortality ratio and increase deliveries utilizing skilled birth attendants to attain the maternal health MDG. Moreover, the Sector Wide Approach (SWAP) was incorporated into the framework of the PRSP (The United Republic of Tanzania 2003; African Development Bank and African Development Fund 2004).
SWAP is an approach where two parties – donors and the government – develop and fund one program. While individual projects were often financed in pieces and driven by each donor before SWAP, SWAP focuses on various sectors, including the health sector, and its operation is sector-wide in scope, comprehensively covering all relevant programs and projects within each sector countrywide. It enables the potential elimination of duplication of activities and a more effective and efficient use of limited resources (Brown 2000). Internal and external resources from donors are pooled and directed to the priority intervention areas agreed upon by the parties concerned. Broad stakeholders in the country are empowered and involved in project and program formulation (Harrold and Associates 1995).
At the same time, in response to the failure of past decentralization efforts, the government of Tanzania strengthened and remodeled the policy into Decentralization by Devolution (D-by-D) in 2000. D-by-D aimed to devolve personnel, planning, and financial decisions to district governments. The implementation of D-by-D was particularly accelerated in the health sector from 1997 on. The Ministry of Health of Tanzania selected the highest priority health services as part of an essential health package in 2000 and empowered district councils to develop Comprehensive Council Health Plans “to provide Tanzanians with equity of access to cost-effective quality health care as close to the family as possible” (Ministry of Health 2000). D-by-D, which was in essence a domestic decentralization policy, and the relevant processes were funded by the health basket fund of SWAP, which was drawn from the global community.
During this drift of internal and external policies, the HSR Programme of Work 1999-2002 focused on further development of the CHF and the national health insurance scheme. The CHF spread to 68 districts by 2005 (Tidemand et al. 2008), with on average 10% of the population living in participating districts. The National Health Insurance Fund was established in 2001 for civil servants (Haazen 2012) and covered approximately 3% of the Tanzanian population as of 2005 (Mensah and Oppong 2009).
Objective
HSRs are expected to have alleviated the disparity in access and utilization of healthcare services across socio-economic groups in the framework of D-by-D and SWAP under PRSP (Gwatkin 2001). In contrast, economic liberalization measures like privatization, introduction of user fees, and failure of decentralization may have increased this disparity. There is, however, little published rigorous evidence of the effect of HSRs on maternal health service utilization in Tanzania. Therefore, determining whether D-by-D and SWAP under PRSP increased the utilization of skilled birth attendants by the poor is crucial to attaining the maternal health MDG. The objective of this study was to determine how the utilization of skilled birth attendants and any disparities in utilization across socio-economic groups have changed over the chain of HSRs in Tanzania.
Materials and Methods
Data
We used datasets from TDHS, provided by the Measure-DHS (Monitoring and Evaluation to Assess and Use Results Demographic and Health Surveys) project, funded by the United States Agency for International Development and implemented by the Inner City Fund Macro International. The project conducted Demographic and Health Surveys in over 90 countries to advance global understanding of health and population trends in developing countries. With the approval of Measure-DHS, we used a series of standard TDHS datasets from 1992, 1996, 1999, and 2004/05 that included 9,238, 8,120, 4,029, and 10,329 women of reproductive age (15-49 years), respectively. The 1992 dataset coincided with the period of progress of economic liberalization reforms such as reviving private practice and introducing user fees in governmental health facilities. Those of 1996 and 1999 coincided with the start of the HSR Plan of Action 1996-1999 and HSR Programme of Work 1999-2002, respectively. The latter program was framed by D-by-D and SWAP. The 2004/05 dataset contained information 5 years after the commencement of the HSR Programme of Work.
TDHS samples were collected using a two-stage cluster sampling method. In the first stage, clusters were selected from the list of census enumeration areas. In the second stage, households were selected systematically from a complete listing of households in each selected cluster. For this study, from all samples, we selected the most recent birth of women in the 5 years preceding each survey and among women whose de jure place of residence was Tanzania mainland, where the reforms took place. The Tanzania mainland is one of the two sovereign states of the United Republic of Tanzania and covers more than 99% of the area and contains approximately 97% of the population of the whole country. After excluding subjects with missing variables, 14,752 subjects (5,078 in 1992, 4,048 in 1996, 1,501 in 1999 and 4,125 in 2004/05) were suitable for the final analysis. According to Measure-DHS guidelines, we used weighted data to be representative of the population (Rutstein and Rojas 2006).
Dependent variables
As an outcome indicator, we used a dichotomous variable of whether or not a respondent utilized a skilled birth attendant. According to the WHO definition, a skilled birth attendant was defined as follows: “A skilled attendant is an accredited health professional – such as a midwife, doctor or nurse – who has been educated and trained to proficiency in the skills needed to manage normal (uncomplicated) pregnancies, childbirth, and the immediate postnatal period, and in the identification, management, and referral of complications in women and newborns.” Traditional birth attendants are not included in this definition in spite of whether they are trained or untrained. We categorized cadres of maternity care providers into “skilled” or not by using the WHO definition (WHO 2004), which is applicable in a Tanzanian context (Adegoke et al. 2012). In this survey, women were asked, “Who assisted with the delivery of (NAME)?” The interviewer ascertained the type of person who assisted with the delivery and recorded it from the choices of different health professionals. Then we coded the following options: medical doctors, assistant medical officers, clinical officers, nurses/midwives, and maternal and child health aides as 1 to represent skilled attendants. We coded traditional birth attendants, in spite of whether they were trained or untrained, village health workers, relatives, neighbors, or any other person who was not a health professional as 0 to represent unskilled attendants.
Independent variables
In this study, a key issue was the inequitable utilization of skilled birth attendants across socio-economic groups, of which the usual indicator is household income (O’Donnell et al. 2007). However, it is not necessarily suitable for areas such as sub-Saharan countries, where monetary economics are not fully developed. Thus, the wealth index has been used as a proxy in developing countries (Rutstein and Johnson 2004). The wealth index is an indicator of the living standard of households that is comparable to expenditures and income measures (O’Donnell et al. 2007). According to the methodology of Demographic and Health Surveys, we assigned each household an asset score generated through principal component analysis by each similar dichotomous indicator of durable assets and utility services. These were, namely, availability of electricity, television, radio, refrigerator, motorcycle, bicycle, and toilet facility; source of water; and the quality of the house reflected by the type of floor. Then, we summed these scores by household and divided households into quintiles of wealth index groups (Rutstein and Johnson 2004), from Quintile 1 (poorest) to Quintile 5 (richest).
In addition, we prepared the following categorical variables of mothers’ attributes from the TDHS datasets to put into the statistical model as independent variables: educational level; literacy; exposure to mass media; religion; marital status; employment status; area of residence; and region of residence. We did not use region dummies to interpret regional characteristics as associated with the utilization of skilled birth attendants, but rather to remove the unmeasured and potentially confounding effects particular to every region. We also included the following continuous variables: maternal age; parity; number of household members; number of health facilities per population of 100,000, and regional gross domestic product per capita. The first three variables were derived from the TDHS datasets; the last two regional attributes were obtained from the Ministry of Health of Tanzania’s Annual Health Statistical Abstracts and the National Accounts of Tanzania mainland, respectively.
Statistical analysis
To assess the utilization of skilled birth attendants by socio-economic group, we formulated a binary logistic regression model as shown in the equation below:
where Pij is the probability of utilization in the year of i (i = 1, 2, 3) by quintile j (j = 1, 2, 3, 4). The term on the left side is the log-odds of utilization rate and α is a constant of this formula. Ti is a time dummy of the specific year i. In this study, Ti is unique to the model; T1 is ‘1996 or later dummy’ and equals 1 if the year was 1996, 1999, or 2004/05, 0 if the year was 1992; T2 is ‘1999 or later dummy’ and equals 1 if the year was 1999 or 2004/05 and 0 if the year was 1992 or 1996; T3 is ‘2004/05 dummy’ and equals 1 if the year was 2004/05 and 0 if the year was 1992, 1996, or 1999. With such unique time dummies, βTi, which is the coefficient of Ti, shows the difference of the log-odds of the utilization rate in the year of i from that in the preceding year of i−1, but only βT1 shows the difference from the reference year of 1992 (see Appendix). Gj is a group dummy of the specific quintile j categorized by relative wealth index scores; G1, G2, G3 and G4 are Quintile 1, Quintile 2, Quintile 3, and Quintile 4 dummies in order. G1 equals 1 if a subject is categorized into Quintile 1 and 0 if she is categorized in any other quintile; the other group dummies are defined in the same manner. The Quintile 5 dummy was not used as that group was the reference category. βGj is a coefficient of Gj and shows the difference of the log-odds of utilization rate in the group of j from that in the reference group of Quintile 5.
Then, TiGj is a cross term of Ti and Gj and its coefficient, βTGij, shows the difference of two differences. One of the two is the difference, which we call Dij, of the log-odds of the utilization rate in the year of i in the group of j from that in the preceding year of i−1 in the same group of j. The second is the difference, which we call Di-ref, of the log-odds in the year of i in the reference group from that in the preceding year of i−1 in the reference group. In other words, βTGij means the difference (Dij−Di-ref) of the change (Dij) of the log-odds of the utilization rate in the group j during the period of i−1 to i, from the change (Di-ref) of that in the reference group during the same period. In this context, if βTi is significantly negative (positive), it indicates that the mean utilization rate in the reference group of Quintile 5 decreased (increased) during the period of i−1 to i. If βGj is significantly negative (positive), it indicates that there was a disparity in the utilization of skilled birth attendants in the reference year of 1992 between quintile j and the reference group of Quintile 5 and women in quintile j utilized skilled birth attendants less (more) than those in Quintile 5. If βTGij is significantly negative (positive) after there was a disparity and the mean utilization rate in quintile j was lower than in Quintile 5 in the year of i−1, it indicates that the disparity increased (decreased or changed into the reversal order of the utilization rate between the two quintiles) during the period of i−1 to i. X is a matrix of all other independent variables and γ is a coefficient vector of X. All data were analyzed using SPSS version 17.0 (SPSS Inc., Chicago, IL, USA), and a p value of ≤ 0.05 represented statistical significance.
Ethical considerations
In Demographic and Health Surveys, informed consent was obtained from participants beforehand, and confidentiality was adhered to during data collection. The survey procedure and instruments were approved by the Ethics Committee of the Opinion Research Corporation Macro International Incorporated (Calverton, MD, USA). Our study was made with anonymous datasets offered by Measure-DHS after approval of the Tokyo Medical and Dental University ethics committee (No. 634).
Results
Descriptive statistics
Table 1 shows descriptive statistics for the dependent variable. The overall percentages of utilization rates of skilled birth attendants show a decreasing trend from 1992 to 1999; thereafter, it increased in 2004/05. Across quintiles of wealth index, the percentage of women utilizing skilled birth attendants in Quintile 1 and 2 decreased from 1992 to 1999 while those of Quintile 3, 4, and 5 increased. Interestingly, a reverse trend was observed from 1999 to 2004; the percentage of women utilizing skilled birth attendants in Quintile 1 and 2 increased while those of Quintile 3, 4, and 5 decreased.
Table 2 depicts descriptive statistics for the independent variables. The mean age of mothers in all of the years was 28.5 years, with approximately 7 to 8 family members and four children born on average. The majority completed primary school; could easily read; were Christians who belonged to the Catholic or Protestant denominations; were married; worked; and lived in rural areas. In terms of exposure to mass media, most could not listen to a radio at least once a week from 1992 to 1999; however, more women listened in 2004/05.
Logistic regression results
Table 3 shows the results of logistic regression analysis. βT1 and βT2 were not significant but βT3 was significantly negative; these results indicate that the mean utilization rate of skilled birth attendants in Quintile 5 did not change from 1992 to 1999, but it significantly decreased in 2004/05 compared with 1999. βG1, βG2, βG3, and βG4 were significantly negative, indicating that the mean utilization rate was lower in 1992 in Quintiles 1, 2, 3, and 4; there were disparities in the utilization of skilled birth attendants between each of these groups and Quintile 5 in 1992. As for the interaction terms of TiG1, βTG11 and βTG21 were significantly negative but βTG31 was significantly positive. These findings mean that the disparity in utilization of skilled birth attendants between Quintile 1 and Quintile 5 significantly increased from 1992 to 1996 and from 1996 to 1999 but significantly decreased from 1999 to 2004/05. Similarly, the disparity between Quintile 2 and Quintile 5 and between Quintile 4 and Quintile 5 significantly increased from 1996 to 1999 and from 1992 to 1996, respectively, but the disparity between Quintile 2 and Quintile 5 significantly decreased from 1999 to 2004/05. Since the utilization of skilled birth attendants in Quintile 5 did not significantly change from 1992 to 1999, utilization in Quintiles 1, 2, and 4 not only relatively decreased in comparison with Quintile 5 but did by absolute measures as well.
In addition, women with primary, secondary, and higher education were significantly more likely to utilize skilled birth attendants than those with no education, and the magnitude of these coefficients showed a tendency to increase utilization in the order listed. The following characteristics had significantly greater associations with utilization rates: mothers who could read easily; those who listened to the radio at least once a week; those who belonged to a religious group; had a higher number of household members; and had access to a higher number of health facilities per population of 100,000. On the other hand, parity and living in rural areas were negatively associated with utilization rates.
Discussion
The effect of HSRs on maternal health service utilization is an unresolved issue with little rigorous evidence. A cross-sectional study and a descriptive study showed a positive association of maternal health outcomes with HSRs, including those under the SWAP in Uganda (Orinda et al. 2005) and decentralization in Sri Lanka (Dmytraczenko et al. 2003), respectively. In contrast, other reports have pointed out the negative effects of HSRs. A qualitative study of the Philippines showed that decentralization in its early phase fragmented the health system and disrupted the referral system; as a result, access to health services was threatened (Lakshminarayanan 2003). A descriptive study of selected African countries (Nanda 2002) and a cross-sectional study of Afghanistan (Mayhew et al. 2008) showed that the introduction of user fees reduced reproductive health service utilization by the poor and consequently widened this disparity. In addition, we found a time-series study on the utilization rate of skilled birth attendants; however, this study did not explicitly argue the association of utilization of skilled birth attendants with HSRs (Kruger et al. 2011). The present study conducted a time-series analysis by using four cross-sectional datasets. Thus, we clarified the chronological change of the association with HSRs for the first time. In general, time-series studies can investigate a change of matters before and after an event, like an HSR, whereas a cross-sectional study cannot.
It has been pointed out that rapid liberalization undermined traditional society and traditional safety nets in developing countries, then increased poverty (Stiglitz 2003). Before the HSRs brought economic liberalization, post-independence Tanzanians had enjoyed free-for-service healthcare in public medical facilities under the socialism policy (Ministry of Health 1996). In fact, utilization rates of skilled birth attendants in 1992 were almost equal between Quintiles 1, 2, and 3, and it was considered that the socialism policy had been somewhat pro-poor. However, the introduction of user fees had a negative impact on the social sector, including healthcare (Tax 2000), and the utilization rate decreased in Quintile 1 from 1992 to 1999 and in Quintile 2 from 1996 to 1999. Furthermore, the disparity increased between each of these two poorer groups and the richest group (Quintile 5). In the case of Thailand, Indonesia, and Cambodia, the introduction of user fees was successful with the use of carefully designed waivers and exemptions (Bitrán and Giedion 2003). Conversely, they deterred utilization among the poor in Kenya, Zambia, and Zaire (Palmer et al. 2004), especially if they were introduced without an effective exemption and waiver system (Bonu et al. 2003). One study suggested that the introduction of user fees was unlikely to achieve equity if these fees were introduced alone without any form of risk sharing (Gilson 1997). In Tanzania, waivers and exemptions were not successfully implemented to provide safety nets for the poor and other vulnerable groups (Haazen 2012).
In addition, the situation was exacerbated by the mushroomed private for-profit healthcare facilities. Most of these facilities were built in economically advantageous locations in urban areas where they were needed the least (Benson 2001) and were inaccessible to the poor due to relatively high charges; this increased the disparity in healthcare utilization based on economic standing (Sahn et al. 2003). These findings, along with the current findings, indicate that reforms using free market mechanisms had a detrimental effect on the utilization of skilled birth attendants by the poor.
On the other hand, the disparity shrunk between 1999 and 2004/05. In 1999, the HSR Programme of Work was developed with the implementation of health SWAP, with the preceding introduction of D-by-D in health sector from 1997, and with the commencement of the first Tanzania PRSP from 2000. SWAP was central to the strategies of the PRSP, whose aim was closely related to attaining MDGs. SWAP and D-by-D essentially enhanced utilization by providing an essential health package. The package made reproductive and child health a key intervention area. The package included providing women with information, education, and communication materials for health-seeking behavior, training of health personnel, and ensuring availability of equipment, supplies, and medicine for essential emergency obstetric care (Ministry of Health 2000). It was assumed that resources would be channeled to the poor and the vulnerable groups, as more funding was allocated to the services included in the essential health package (Brown 2000; Ensor et al. 2002). It was important to strengthen the healthcare system and bridge the gaps between the community and formal health sector to enhance utilization of skilled birth attendants (Pfeiffer and Mwaipopo 2013). It was also assumed that the health package successfully helped with such strengthening and bridging. Expenditures for reproductive health in Tanzania increased by 80.75% between 2002 and 2005 (Ministry of Health and Social Welfare 2008). An increase in health expenditures in poor countries is associated with an increase in the utilization of skilled birth attendants (Kruk et al. 2007).
Moreover, the number of districts operating the CHF increased from 10 in 1999 to 68 in 2005 under the framework of D-by-D and SWAP. The CHF mainly covered those who were living in rural areas and the poor (Mtei and Mulligan 2007). This program led to sick individuals in member households getting treatment 15% more often than those in non-member households (Msuya et al. 2007). Furthermore, CHF members were 1.6 times more likely to access outpatient care than non-members (Chanfreau et al. 2005). The majority of poor households viewed enrollment in CHF as important compared to relatively wealthier groups (Kamuzora and Gilson 2007). Utilization patterns in primary public health facilities and district hospitals seemed to have changed from pro-rich to pro-poor (Makawia et al. 2010). These findings suggest that the CHF played a part in increasing the utilization of skilled birth attendants among poor women.
As mentioned above, the HSR Plan of Action was in operation from 1996 to 1999 before the HSR Programme of Work with health SWAP and full-scale D-by-D. During this period, the disparity was still widening as in the preceding period. The reason could be that this period was the preliminary stage for the forthcoming full-scale reforms aimed at poverty reduction. In 1999, the CHF had only been executed in 10 of 114 districts. Private insurance services and micro-insurance schemes were estimated to cover less than 0.3% and 1% of the total population, respectively (Bultman et al. 2012; Haazen 2012).
In our analysis, mothers’ educational level and religious group membership increased the utilization of skilled birth attendants. Education helped women comprehend health information from various sources, such as health facility staff during antenatal care, brochures, or the radio, and make healthier choices. In fact, the ability to read easily and listen to the radio at least once a week significantly increased the utilization of skilled birth attendants. In addition, the use of maternal health services was strongly influenced by the practices of other women (Gage 2007); thus, belonging to a religious group might offer opportunities to interact with other women and share information. A higher number of household members and access to more health facilities per population of 100,000 were also associated with increased utilization of skilled birth attendants. Family members affected the final decision on location of birth (Kabakyenga et al. 2012) and easy access to the nearest health facility could improve the utilization rate (Gage 2007; Mpembeni et al. 2007). On the other hand, increased parity reduced the utilization of skilled birth attendants (Kabakyenga et al. 2012). Women with less experience with pregnancy were more likely to be concerned and seek expert care. Living in rural areas also reduced utilization, as has been shown in previous studies (Wang et al. 2011; Kabakyenga et al. 2012).
Again, from 1999 to 2004/05, utilization of skilled birth attendants in Quintiles 1 and 2 increased in comparison with changes in Quintile 5. However, the utilization rate in the two groups in 2004/05 barely matched the 1992 rate, because the numbers had decreased in the two preceding periods. In addition, we should pay attention to the fact that the utilization of skilled birth attendants by Quintile 5 was significantly reduced from 1999 to 2004/05, although the National Health Insurance was founded in 2001 and covered public servants, who were relatively wealthier. Unfortunately, we cannot examine the effect of the implementation of National Health Insurance on utilization rates, as there is no information on civil servants in the datasets. Moreover, the utilization rate was lowest in Quintile 3 in 2004/05. Regression results also showed no change in the disparity in utilization of skilled birth attendants among Quintiles 3, 4, and 5 from 1999 to 2004/05. HSR measures may not have been as effective among these three relatively wealthier groups. Futhermore, many health professionals did not uniformly possess or demonstrate many of the abilities that would qualify them as skilled birth attendants, due to inconsistencies in pre-service training and regulations (Spangler 2012). We should pay attention to such wide differences in ability.
Nevertheless, the HSR Programme of Work with D-by-D and SWAP under PRSP seemed to correct the downward trend and increase the utilization of skilled birth attendants, especially by poor women. Recently, it was pointed out that government intervention was indispensable to successful development of the least developed countries. Government interventions should not rely only on free market mechanisms in the sense of economics, but also establish and use non-market institutions (Stiglitz 1989), which are infrastructures such as property rights, peace, formal rules, laws, and regulations along with the informal rules of society; the economic environment; and education, healthcare, and the natural environment required for economic activity (World Bank 1997). D-by-D facilitated making Comprehensive Council Health Plans that prioritized reproductive health among overall healthcare and that conformed to the needs of the districts concerned. SWAP founded the financial basis for D-by-D and enhanced participation of the local government and broad stakeholders, including poor people, in program formulation. It is assumed that D-by-D, SWAP, and relevant institutions together helped enhance the utilization of skilled birth attendants and reduced disparity in groups due to economic differences.
There are a few limitations to this study. First, HSR measures were implemented intermittently, month by month, district by district, as decentralization gradually progressed. The datasets, however, include only information on regions, which are larger areas than districts, in the four time periods studied. Therefore, we cannot discriminate which particular HSR measures were effective in improving utilization of skilled birth attendants. We can only make assumptions within the general framework of the HSRs. Second, TDHS adopted a two-stage cluster sampling method, but the statistical model of this study could not reflect the variance of the utilization rate between clusters. If the intra-cluster correlation is not so small as to be negligible, too low p values may be reported in the regression analysis. Third, we used information that was reported by respondents about past medical/pregnancy experiences; this information may be prone to recall bias. However, we minimized this bias by using information obtained from the most recent birth of the respondents in each survey.
Conclusion
In Tanzania, HSRs were continuously carried out in response to domestic and global circumstances. In the early 1990s, liberalization measures such as privatization and the introduction of user fees were predominant due to poor economic conditions. In the mid-1990s, some attempts were started to enhance universal access by securing a safety net like the CHF and empowering local councils to make district health plans matching local needs. By the end of 1990s, D-by-D and SWAP had been introduced in health sectors and endeavors to reduce poverty started in earnest. Indeed, findings of this study showed that the disparity in the utilization of skilled birth attendants across socio-economic groups decreased from 1999 to 2004/05 in Tanzania, while it had increased from 1992 to 1999. The downward trend of utilization by poor women seemed to reverse around 1999. These findings imply that continuing and enhancing D-by-D and SWAP in the process of HSRs may further reduce the disparity, and may improve the utilization of skilled birth attendants to come closer to attaining the maternal health MDG.
Conflict of Interest
The authors have no conflict of interest to declare.
Appendix
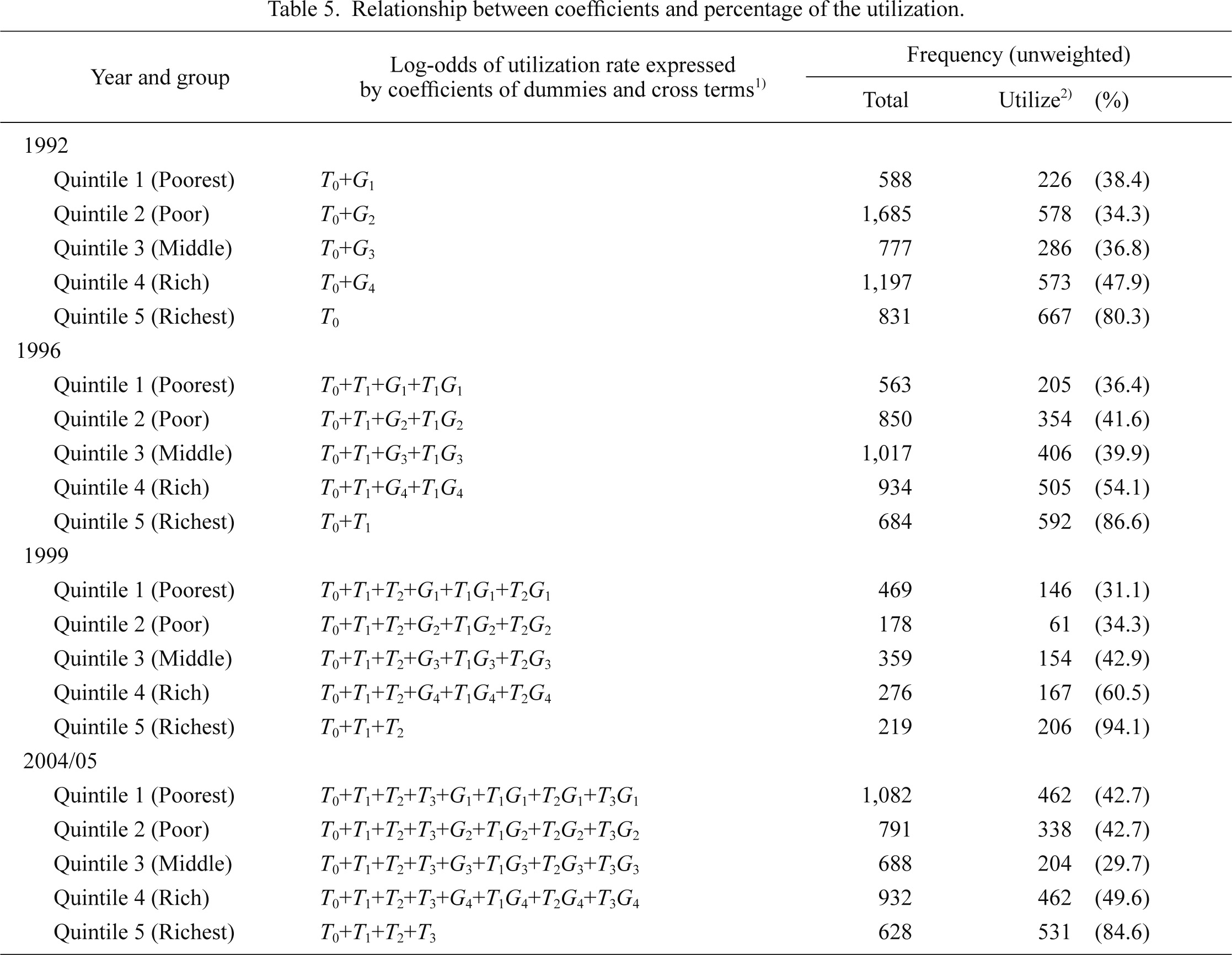
Time dummy Ti of this study is unique to the model to measure the effect in the time i based on the preceding time i−1. In usual statistical models, Ti equals 1 if the time is only the specific time i, and 0 if it is all other times (..., i−2, i−1, i+1, i+2, ...). Ti and its cross term reflect the effects at time i based on the reference time. For example, in the datasets of this study, if the time dummies are used in the usual manner, T1, T2, and T3 reflect the effects in 1996, 1999, and 2004/05, respectively, and the baseline is always 1992 as the reference. However, we defined time dummies in a unique manner in this study to make T1, T2, and T3 reflect the effect in 1996, 1999, and 2004/05 based on the preceding time, that is, 1992, 1996, and 1999, respectively. Concretely speaking, Ti is defined as 1 if the time is i or later (i, i+1, i+2, ...) and 0 if it is before i (..., i−2, i−1). We can empirically make sure of the validity of the unique time dummies and the interpretation using the datasets of unweighted samples of the model with only time dummies Ti and group dummies Gj.
The regression results of the model are shown in Table 4; we call the constant T0 for convenience. In such a simple model without other potential confounding variables, the log-odds of the utilization of skilled birth attendants within each group in every year should be expressed by coefficients of the dummies and cross terms as shown in the second column of Table 5. These unique time dummies should show the difference of two log-odds between the time of i and i−1. While the frequency and percentage of women in the unweighted sample who utilized skilled birth attendants are shown in right column of Table 5, we calculated the probabilities from the log-odds computed from the coefficients. Then, we confirmed that the probability within every group in every year was consistent with the percentage at the level of 8 significant digits. Thus, we believe the validity of our methods is sound.
References
-
Adegoke,
A.,
Utz,
B.,
Msuya,
S.E. &
van den Broek,
N.
(2012) Skilled birth attendants: who is who? a descriptive study of definitions and roles from nine sub Saharan African countries. PLoS One, 7, e40220.
-
African Development Bank
&
African Development Fund
(2004) Revised Guidelines for Bank Group Operations using Sector-Wide Approaches (SWAps), African Development Bank, Tunis.
-
Barros,
A.J.D.,
Ronsmans,
C.,
Axelson,
H.,
Loaiza,
E.,
Bertoldi,
A.D.,
França,
G.V.A.,
Bryce,
J.,
Boerma,
J.T. &
Victora,
C.G.
(2012) Equity in maternal, newborn, and child health interventions in Countdown to 2015: a retrospective review of survey data from 54 countries. Lancet, 379, 1225-1233.
-
Benson,
J.S.
(2001) The impact of privatization on access in Tanzania. Soc. Sci. Med., 52, 1903-1915.
-
Bitrán,
R. &
Giedion,
U.
(2003) Waivers and Exemptions for Health Services in Developing Countries, World Bank, Washington, D.C.
-
Bonu,
S.,
Rani,
M. &
Bishai,
D.
(2003) Using willingness to pay to investigate regressiveness of user fees in health facilities in Tanzania. Health Policy Plan., 18, 370-382.
-
Brown,
A.
(2000) Current Issues in Sector-wide Approaches for Health Development: Tanzania Case Study, World Health Organization, Geneva.
-
Bultman,
J.,
Kanywanyi,
J.L.,
Maarifa,
H. &
Mtei,
G.
(2012) Tanzania Health Insurance Regulatory Framework Review, Ministry of Health and Social Welfare & Social Security Regulatory Authority, Dar es Salaam.
-
Burki,
O.
(2001) Sector-Wide Approach in Tanzania: The Health Sector Example: Observations from a Bi-lateral, Swiss Agency for Development and Co-operation, Berne.
-
Chanfreau,
C.,
Musau,
S. &
Kidane,
L.
(2005) Costing HIV/AIDS Services for Community Health Fund Members and Non-members in Hanang District, Tanzania, Abt Associates Inc., Bethesda, MD.
-
Dmytraczenko,
T.,
Rao,
V. &
Ashford,
L.
(2003) Health Sector Reform: How it Affects Reproductive Health, Population Reference Bureau, Washington, D.C.
-
Ensor,
T.,
Dave-Sen,
P.,
Ali,
L.,
Hossain,
A.,
Begum,
S.A. &
Moral,
H.
(2002) Do essential service packages benefit the poor? Preliminary evidence from Bangladesh. Health Policy Plan., 17, 247-256.
-
Gage,
A.J.
(2007) Barriers to the utilization of maternal health care in rural Mali. Soc. Sci. Med., 65, 1666-1682.
-
Gilson,
L.
(1997) The lessons of user fee experience in Africa. Health Policy Plan., 12, 273-285.
-
Gwatkin,
D.R.
(2001) The need for equity-oriented health sector reforms. Int. J. Epidemiol., 30, 720-723.
-
Haazen,
D.
(2012) Making Health Financing Work for Poor People in Tanzania, World Bank, Washington, D.C.
-
Harrold,
P.
&
Associates
(1995) The Broad Sector Approach to Investment Lending: Sector Investment Programs, World Bank, Washington D.C.
-
Houweling,
T.A.J.,
Ronsmans,
C.,
Campbell,
O.M.R. &
Kunst,
A.E.
(2007) Huge poor-rich inequalities in maternity care: an international comparative study of maternity and child care in developing countries. Bull. World Health Organ., 85, 745-754.
-
Kabakyenga,
J.K.,
Östergren,
P.O.,
Turyakira,
E. &
Pettersson,
K.O.
(2012) Influence of birth preparedness, decision-making on location of birth and assistance by skilled birth attendants among women in south-western Uganda. PLoS One, 7, e35747.
-
Kamuzora,
P. &
Gilson,
L.
(2007) Factors influencing implementation of the community health fund in Tanzania. Health Policy Plan., 22, 95-102.
-
Kruger,
C.,
Olsen,
O.E.,
Mighay,
E. &
Ali,
M.
(2011) Where do women give birth in rural Tanzania? Rural Remote Health, 11, 1791.
-
Kruk,
M.E.,
Galea,
S.,
Prescott,
M. &
Freedman,
L.P.
(2007) Health care financing and utilization of maternal health services in developing countries. Health Policy Plan., 22, 303-310.
-
Lakshminarayanan,
R.
(2003) Decentralisation and its implications for reproductive health: the Philippines experience. Reprod. Health Matters, 11, 96-107.
-
Makawia,
S.,
Macha,
J.,
Ally,
M. &
Borghi,
J.
(2010) An Assessment of the Distribution of Health Service Benefits in Tanzania, University of Cape Town, Cape Town.
-
Mayhew,
M.,
Hansen,
P.M.,
Peters,
D.H.,
Edward,
A.,
Singh,
L.P.,
Dwivedi,
V.,
Mashkoor,
A. &
Burnham,
G.
(2008) Determinants of skilled birth attendant utilization in Afghanistan: a cross-sectional study. Am. J. Public Health, 98, 1849-1856.
-
Mensah,
J. &
Oppong,
J.R.
(2009) Maternity Protection and Health Insurance in Africa: Comparative Overview of Ghana, Kenya, Rwanda, and Tanzania, International Labour Office, Geneva.
-
Ministry of Health
(1994) Proposals for Health Sector Reform, Ministry of Health, Dar es Salaam.
-
Ministry of Health
(1996) Health Sector Reform: Plan of action 1996-1999, Ministry of Health, Dar es Salaam.
-
Ministry of Health
(2000) National Package of Essential Health Interventions in Tanzania, Ministry of Health, Dar es Salaam.
-
Ministry of Health and Social Welfare
(2008) Tanzania National Health Accounts (NHA) Year 2002/3 and 2005/6, Ministry of Health and Social Welfare, Dar es Salaam.
-
Mpembeni,
R.N.M.,
Killewo,
J.Z.,
Leshabari,
M.T.,
Massawe,
S.N.,
Jahn,
A.,
Mushi,
D. &
Mwakipa,
H.
(2007) Use pattern of maternal health services and determinants of skilled care during delivery in southern Tanzania: implications for achievement of MDG-5 targets. BMC Pregnancy Childbirth, 7, 29.
-
Msuya,
J.M.,
Jütting,
J. P. &
Asfaw,
A.
(2007) Impact of community health funds on the access to health care: empirical evidence from rural Tanzania. Int. J. Public Admin., 30, 813-833.
-
Mtei,
G. &
Mulligan,
J.
(2007) Community Health Funds in Tanzania: A Literature Review, Ifakara Health Institute, Dar es Salaam.
-
Munga,
M.A.,
Songstad,
N.G.,
Blystad,
A. &
Mæstad,
O.
(2009) The decentralisation-centralisation dilemma: recruitment and distribution of health workers in remote districts of Tanzania. BMC Int. Health Hum. Rights, 9, 9.
-
Nanda,
P.
(2002) Gender dimensions of user fees: implications for women’s utilization of health care. Reprod. Health Matters, 10, 127-134.
-
National Bureau of Statistics Tanzania (NBS)
&
ICF Macro
(2011) Tanzania Demographic and Health Survey 2010, NBS, Dar es Salaam & ICF Macro, Calverton, MD.
-
O’Donnell,
O.,
van Doorslaer,
E.,
Wagstaff,
A. &
Lindelow,
M.
(2007) Analyzing Health Equity Using Household Survey Data: A Guide to Techniques and their Implementation, World Bank, Washington D.C.
-
Orinda,
V.,
Kakande,
H.,
Kabarangira,
J.,
Nanda,
G. &
Mbonye,
A.K.
(2005) A sector-wide approach to emergency obstetric care in Uganda. Int. J. Gynaecol. Obstet., 91, 285-291.
-
Palmer,
N.,
Mueller,
D.H.,
Gilson,
L.,
Mills,
A. &
Haines,
A.
(2004) Health financing to promote access in low income settings — how much do we know? Lancet, 364, 1365-1370.
-
Pariyo,
G.W.,
Ekirapa-Kiracho,
E.,
Okui,
O.,
Rahman,
M.H.,
Peterson,
S.,
Bishai,
D.M.,
Lucas,
H. &
Peters,
D.H.
(2009) Changes in utilization of health services among poor and rural residents in Uganda: are reforms benefitting the poor? Int. J. Equity Health, 8, 39.
-
Pfeiffer,
C. &
Mwaipopo,
R.
(2013) Delivering at home or in a health facility? health-seeking behaviour of women and the role of traditional birth attendants in Tanzania. BMC Pregnancy Childbirth, 13, 55.
-
Rutstein,
S.O. &
Johnson,
K.
(2004) The DHS Wealth Index, ORC Macro, Calverton, MD.
-
Rutstein,
S.O. &
Rojas,
G.
(2006) Guide to DHS Statistics, ORC Macro, Calverton, MD.
-
Sahn,
D.E.,
Younger,
S.D. &
Genicot,
G.
(2003) The demand for health care services in rural Tanzania. Oxford B. Econ. Stat., 65, 241-259.
-
Spangler,
S.A.
(2012) Assessing skilled birth attendants and emergency obstetric care in rural Tanzania: the inadequacy of using global standards and indicators to measure local realities. Reprod. Health Matters, 20, 133-141.
-
Stiglitz,
J.E.
(1989) Markets, market failures, and development. Am. Econ. Rev., 79, 197-203.
-
Stiglitz,
J.E.
(2003) Globalization and growth in emerging markets and the new economy. J. Policy Model., 25, 505-524.
-
Tax,
S.L.
(2000) The social consequences of structural adjustment reforms in Tanzania. The Tanzanet-J., 1, 4-18.
-
The United Republic of Tanzania
(2003) Poverty Reduction Strategy: The Second Progress Report 2001/02, International Monetary Fund, Washington D.C.
-
Tidemand,
P.,
Olsen,
H.B. &
Sola,
N.
(2008) Local Level Service Delivery, Decentralisation and Governance: A Comparative Study of Uganda, Kenya and Tanzania Education, Health and Agriculture Sectors: Tanzania Case Report, Japan International Cooperation Agency, Tokyo.
-
Wang,
W.,
Alva,
S.,
Wang,
S. &
Fort,
A.
(2011) Levels and Trends in the Use of Maternal Health Services in Developing Countries, ICF Macro, Calverton, MD.
-
World Bank
(1997) World Development Report 1997: The State in a Changing World, Oxford University Press, New York, NY.
-
World Health Organization (WHO)
(2004) Making Pregnancy Safer: The Critical Role of the Skilled Attendant: A Joint Statement by WHO, ICM and FIGO, WHO, Geneva.
-
World Health Organization
(2009) WHO Recommended Interventions for Improving Maternal and Newborn Health, 2nd ed., WHO, Geneva.
-
World Health Organization
(2010) WHO Technical Consultation on Postpartum and Postnatal Care, WHO, Geneva.
-
WHO; UNICEF; UNFPA
&
World Bank
(2012) Trends in Maternal Mortality: 1990 to 2010, WHO, Geneva.