Abstract
Gastrointestinal stromal tumors (GISTs) are the most common among gastrointestinal mesenchymal tumors, but its prognosis has not been accurately predicted by the current risk stratification guidelines, National Institutes of Health classification. In this study, we evaluated the predictive factors for GIST prognosis in a retrospective analysis of 332 patients. The data collected included tumor sites, including the esophagus, stomach, duodenum, small intestine, and extragastrointestinal sites; tumor size; microscopic indicators for malignant tumor behavior, such as the number of dividing cells, cell necrosis, atypical morphology, and invasion into the muscular or mucous layer; and previously established immunohistochemical indicators, CD117, CD34, and discovered on GIST-1 (DOG-1). No single occurrence of any microscopic indicators correlated with the prognosis of GIST; however, the total number of microscopic indicators was a significant prognostic factor of GIST (P < 0.001). Regarding the tumor sites, the order of prognostic risk (from the lowest to the highest) was as follows: the esophagus, stomach, duodenum, small intestine, extragastrointestinal sites, and colorectum. The association between tumor sites and prognosis was significant (P < 0.001). On the other hand, the expression of CD117 or CD34 was not associated with the risk of GIST. Importantly, 91% of the patients (302/332) showed the expression of DOG-1, and the lack of DOG-1 expression was associated with poor prognosis (P < 0.05). In conclusion, both tumor sites and total number of microscopic indicators are independent risk factors associated with the prognosis of GIST. The lack of DOG-1 expression may be predictive of malignant outcome.
Introduction
The category of gastrointestinal stromal tumors (GISTs), the definition of which was first proposed by Mazur and Clark (1983), originates from gastrointestinal mesenchymal stem cells. GIST accounts for approximately 0.1%-3% of all gastrointestinal tract tumors (Comandone and Boglione 2005), and GIST is the most common type of abdominal mesenchymal tumors. Although surgical resection of the tumor may be curative for the disease, the probability of tumor recurrence or metastasis remains high postoperatively. The prognostic risk of GIST postoperatively is estimated based on the risk classification guideline of the United States National Institutes of Health (NIH) (Joensuu 2008). This guideline uses tumor size and the number of dividing cells as parameters for determination of the risk of GIST. This guideline also classifies tumors originating from the stomach or non-stomach regions into different risk categories. Non-stomach GIST can be found in the small intestine and colorectal or extragastrointestinal sites; however, the association between these tumor sites and prognostic risk remains unclear (He et al. 2012).
The expert panel that established the NIH classification consensus believed that the evaluation of microscopic morphological indicators is subject to inter-examiner variability, with the exception of tumor size and mitotic counts, and that reproducibility from different pathologists is poor. Nevertheless, selected microscopic indicators, including tumor necrosis, arrangement of surrounding blood vessels, atypia, invasion into the muscularis propria, and invasion into the mucous layer, have been shown to be correlated with the prognostic risk of GIST (He et al. 2012).
Several immunohistochemical markers have been proposed for GIST. CD117 is the protein product of the c-kit proto-oncogene, which is a transmembrane tyrosine kinase receptor. For GIST, the expression rate of CD117 was estimated to be 85%-95% (Laurini and Carter 2010). Approximately 50%-85% of patients with GIST showed the expression of CD34, which is a hematopoietic precursor cell marker (Tan et al. 2012). Discovered on GIST-1 (DOG-1) was identified as a gene that was highly expressed in patients with GIST. The protein product of DOG-1 is a membrane protein comprising eight transmembrane regions that functions as a calcium-regulated chloride channel protein (Liegl et al. 2009). DOG-1 has been considered as a novel diagnostic marker for GIST, with the sensitivity that is superior to that of CD117, particularly for CD117− GIST with suspicious morphology (Miettinen et al. 2009). In such GIST, DOG-1 can be used selectively in combination with the platelet-derived growth factor subunit-A for auxiliary diagnosis. The application of an anti-DOG-1 monoclonal antibody further showed high sensitivity and specificity for GIST (Espinosa et al. 2008). However, evidence of a relationship between the expression of DOG-1 and the prognosis of GIST is limited.
In summary, the NIH risk classification is not sufficient to predict precisely the prognostic risk of GIST postoperatively in clinical settings (Wada et al. 2014); however, a replacement guideline has not been widely established yet. Here, we analyzed retrospectively clinical and pathological features of 332 patients with GIST, with the aim of an evaluation of predictive factors for the prognosis of GIST and potentially providing supplementary tools to the NIH risk guideline.
Materials and Methods
Clinical Data
The medical records of 332 patients with GIST who were admitted to the First Affiliated Hospital of Anhui Medical University between January 2002 and December 2011 for surgical treatment were collected. To confirm the diagnosis, pathology sections were reviewed by two senior gastrointestinal pathologists. Data regarding sex, age, tumor site (esophagus, stomach, duodenum, small intestine, colorectum, and extragastrointestinal sites), maximal tumor diameter, and lymph node status of patients were obtained from clinical history and the general pathological records. For this study, we obtained approval of the Ethics Committee of Anhui Medical University. All protocols for analysis of patient records were approved by the Institutional Review Board.
Immunohistochemical Examination
Histological sections (4 μm) of 10% formalin-fixed paraffin-embedded samples from all 332 patients were used for immunohistochemical examination. Primary antibodies used were as follows: anti-CD34 (polyclonal, QBEnd/10), anti-CD117/C-kit (polyclonal, YR145), and anti-DOG-1 antibodies (polyclonal, SP31) (Maixin-Bio, Inc., Fuzhou, China). Antigen retrieval was performed in ethylene-diaminetetraacetic acid (pH 8.0) using a pressure cooker for 10 min at 98°C. All slides were treated with 3% hydrogen peroxide to block endogenous peroxidase, followed by incubation with primary antibodies against CD34, CD117, or DOG-1 at 4°C overnight. Immunohistochemical staining was performed using the EliVisionTM plus IHC Kit (Maixin-Bio, Inc., Fuzhou, China) and was visualized using diaminobenzidine (DAB Kit; Maixin-Bio, Inc., Fuzhou, China). Negative controls were prepared by replacing primary antibodies with phosphate-buffered saline (PBS). Known immunostaining-positive sections were used as positive controls.
Histological Examination
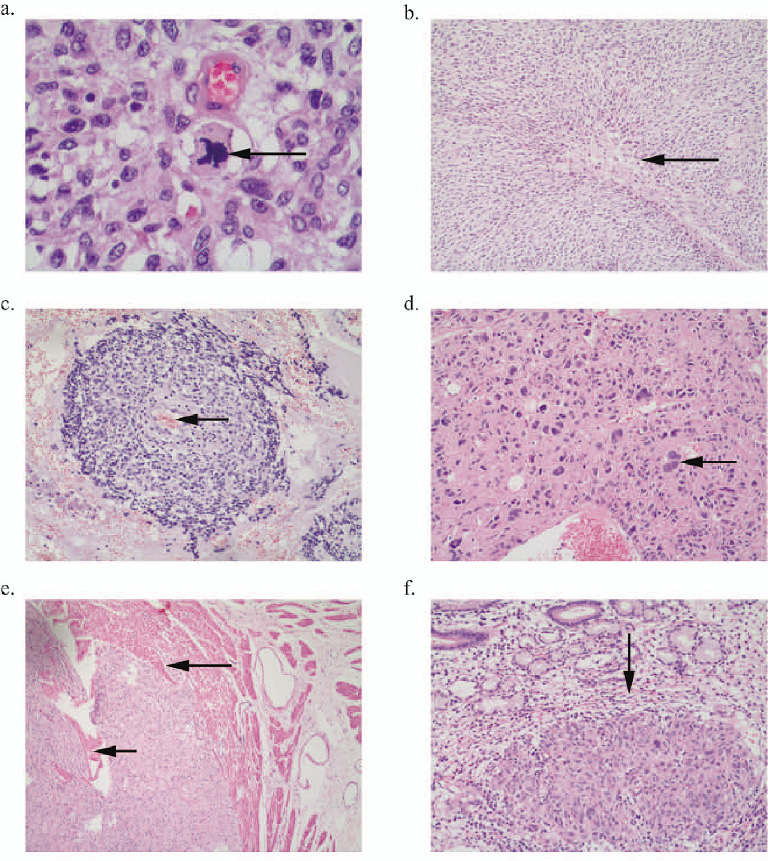
For each case, a total of 4-28 hematoxylin and eosin (HE)-stained slides (median, six slides) were reviewed. The following morphological indicators were recorded: (1) mitotic counts, mitotic cell counts were recorded/high power field (HPF) using a microscope [the count/50 HPFs was reported; the mitosis level was categorized into three groups, < 5/50 HPFs, 5-10/50 HPFs, and ≥ 10/50 HPFs (Fig. 1a)]; (2) necrosis, referring to tumor necrosis, defined by a residual shadow of tumor cells in the necrotic area (Yan et al. 2003) (Fig. 1b); (3) arrangement of surrounding vessels: referring to tumor cells surrounded by thin walled-blood vessels, with degeneration or necrosis of adjacent cells and the formation of coin-shaped structures (Miettinen et al. 2006) (Fig. 1c); (4) atypia, referring to cells with an atypical morphology (Yan et al. 2003) (Fig. 1d); (5) invasion into the muscularis propria: referring to tumor cells forming destructive structures that separate smooth muscle fibers (Tworek et al. 1999) (Fig. 1e); and (6) invasion into the mucous layer: referring to tumor cells that invade the mucoderm (Tworek et al. 1999) (Fig. 1f). For each case, the total number of these positive histological indicators was recorded as the total number of microscopic indicators.
The classification standard proposed by the United States NIH in 2008 was used; this classification is recommended for risk classification by the expert panel of GIST in China (Joensuu 2008; Chinese Diagnosis and Treatment Experts Group for Gastrointestinal Stromal Tumors 2009).
Patient Follow-up
Patients were followed-up through revisits to the clinic, phone calls, or mail. The follow-up cut-off date was 6/30/2012. Survival time was defined as the time elapsed from the date of surgical treatment to death or the date of the last follow-up (for those who could not be followed-up half-way through). Deaths caused by other diseases or accidents were excluded from this study.
Statistical Analysis
Data entry was reviewed and confirmed by two authors independently. Statistical analysis was performed using the SPSS software, version 16.0. A comparison of the counting data was performed using the chi-squared test (with Yates’ correction, when applicable). Ridit analysis was performed to test association between ranked data, and linear by linear association test was used for doubly ordered R × C table. P < 0.05 was considered statistically significant. The survival data were analyzed using univariate regression analysis. Significant factors derived from univariate analysis were tested using Kaplan-Meier survival analysis. Cox regression was applied to evaluate the influence of variables on survival.
Results
Clinical Data
The 332 patients with GIST included 200 men and 132 women aged 13-88 years (median age, 58 years). Tumor sites were the esophagus in nine patients, the stomach in 112, the duodenum in 66, the small intestine in 75, the colorectal region in 43, and extragastrointestinal sites in 27, including the gastrocolic omentum in 15, the mesocolon in 10, and the mesentery of the small intestine in 2. Thus, the most frequently observed site was the stomach, followed by the small intestine. The majority of tumors metastasizing from GIST occurred by metastasis through blood vessels; metastasis to regional lymph nodes was found in one among 332 patients with GIST (Table 1). The NIH risk classification was estimated for these patients. A total of 56 (14.0%) patients with very low risk, 92 (22.9%) patients with low risk, 83 (20.7%) patients with intermediate risk, and 101 (25.2%) patients with high risk were observed.
Immunohistochemistry
Immunohistochemical features of CD117, CD34, and DOG-1 are shown in Fig. 2. The expression of CD117 or DOG-1 was defined as the presence of a diffuse membranous and/or cytoplasmic staining in tumor cells, and the expression of CD34 was defined as the presence of cytoplasmic staining in tumor cells. The positive expression rates of CD117 and CD34 were 90.7% (301/332) and 88.3% (293/332), respectively. Moreover, the expression of these two markers was not associated with the NIH risk classification (P > 0.05). The positive expression rate of DOG-1, being 91.0% (302/332), was associated with the NIH risk classification (P < 0.05) (Table 2). The positive expression rate of DOG-1 was 87.1% (27/31) in CD117− cases, while the positive expression rate of DOG-1 was 94.9% of CD34− cases (37/39).
Histology
Histomorphological indicators, including necrosis, arrangement of surrounding vessels, atypia, invasion into the muscularis propria, and mucosal infiltration, were examined using a microscope. None of the single microscopic histomorphological indicators correlated with the NIH risk classification. Therefore, we summarized the number of positive microscopic findings as the total number of microscopic indicators. The total number of microscopic indicators was highly associated with the NIH risk classification (P < 0.01) (Table 3).
Follow-up and Survival Analysis
For 293 patients with a follow-up duration of 5 years, the accumulative 1-, 3-, and 5-year survival rates were 93.0%, 87.0%, and 66.0%, respectively. Table 4 shows the results of univariate Cox regression analysis of the factors contributing to the survival of 332 patients with GIST. Immunohistochemical indicators CD117 and CD34 were not associated with the prognosis of GIST, whereas a greater total number of microscopic indicators, higher NIH risk classification, and negativity for expression of DOG-1 were significantly associated with worse prognoses (P < 0.05). Tumor site was also significantly associated with the prognosis of GIST, with a trend toward increasing risk (P < 0.05) for tumors located in the esophagus, stomach, duodenum, small intestine, extragastrointestinal sites, and colorectum, in this order.
Subsequent Kaplan-Meier survival analysis revealed the presence of a significant difference in the survival rates between the groups with the positive and negative expression of DOG-1 (Fig. 3a). Significant difference was also observed in the survival rates among the NIH risk classification groups with very low, low, intermediate, and high risk (Fig. 3b). The survival rate decreased with an increase in the total number of microscopic histomorphological indicators (Fig. 3c). Tumors at various sites also had significantly different survival rates. The ranking of survival rate (from the lowest to the highest) was as follows: esophagus, stomach, duodenum, small intestine, extragastrointestinal sites, and colorectum (Fig. 3d).
Discussion
Pathological diagnosis of GIST is the overall judgment based on general pathology, histopathology, immunohistochemistry, and results of genetic testing. Here, we evaluated the appropriateness of the NIH standards in conjunction with histological and immunohistochemical markers for diagnosis of GIST. In the current study, the positive expression rates of CD117 and CD34 were 90.7% and 88.3%, respectively. Univariate analysis demonstrated that the expression of CD117 and CD34 was not associated with patients’ prognosis; further, this suggested that these parameters were immunohistochemical indicators that were sensitive for diagnosis of GIST, rather than prognosis indicators. The positive expression rate of DOG-1 was 91.0%; this was higher than that of CD117. Moreover, the positive expression rate of DOG-1 reached 87.1% (27/31) in CD117− cases; this suggests that DOG-1 can also be used as a sensitive immunohistochemical indicator for diagnosis of GIST, and that the combined detection of CD117 and DOG-1 can improve the accuracy of diagnosis of GIST. It has been identified that not all GISTs are positive for the expression of CD117 and DOG-1. Some of these tumors are now described as wild-type GIST, some of which are deficient in succinate dehydrogenase (Doyle et al. 2012). Moreover, our univariate analysis demonstrated that the negative expression of DOG-1 was associated with patients’ prognosis. We speculate that the negative expression of DOG-1 may be predictive of poor prognosis. This is consistent with the findings of Jung et al. (2011). Nevertheless, the negative expression rate of DOG-1 was low in patients included in the current study, and the number of patients with negative expression was low. Thus, further investigation regarding whether the negative expression of DOG-1 can be used as a marker to determine the malignant biological behavior of GIST is required.
The accurate determination of the biological behavior of GIST is extremely important for deciding clinical treatment. However, because currently no tangible criteria exist that can be used to define benign vs. malignant GIST, it is difficult to predict the clinical outcome of these tumors. At present, the classification scheme of the United States NIH is used widely (Joensuu 2008). The NIH classification designated tumor size and mitotic counts as important parameters to determine the GIST risk stratification, and sites of tumors with a stomach vs. non-stomach origin are also included. However, He et al. (2012) believed that the NIH classification does not apply to borderline cases of GIST. Tumor size and mitotic counts are insufficient to predict precisely the prognosis of GIST; thus, the NIH classification has potential issues of underestimation or overestimation. Our study found that GIST originated from different sites had significantly different NIH risk classification and prognosis. Further analysis showed that when tumors were ranked according to the order of tumor origin of the esophagus, stomach, duodenum, small intestine, and colorectum, the NIH risk classification sequentially started from low to high, and prognosis worsened. The NIH classification and the prognosis of GIST with the colorectal origin were inferior to GIST that originated from other sites. Therefore, we believe that the strategy of the NIH classification, which only differentiates tumor malignancy based on gastric vs. non-gastric origin, warrants improvement; the role of tumor origin in the evaluation of the biological behavior of GIST should be further strengthened. Whether to redefine the risk stratification standard to address different tumor origin is pending further discussion. The Armed Forces Institute of Pathology classification of GISTs, which classifies GIST according to different tumor sites, has the potential to replace or supplement the NIH classification for use in patients from China (Joensuu et al. 2012).
Hou et al. (2010) pointed out that a standard established based merely on two indicators, including tumor size and mitotic counts, is not capable of differentiating malignant from nonmalignant GIST. In addition, those authors screened microscopic biological indicators to predict the biological behavior of GIST. We found no significant association between any single microscopic morphological indicator and NIH classification and the prognosis of GIST. This suggests that no single microscopic morphological indicator can be used to determine the biological behavior of GIST. However, the total number of positive microscopic morphological indicators in each GIST was an independent risk factor associated with the prognosis of GIST. Therefore, microscopic morphological indicators can be used as a helpful complement to determine the biological behavior of GIST.
The biological behavior of GIST remains a perplexing issue, given that even GISTs with smaller lesions (< 2 cm) or inactive cell division can exhibit recurrence and metastasis (Fletcher et al. 2002). The development of adjuvant therapies using postsurgery molecular targeting drugs has turned the direction of GIST treatment from a single surgical resection to more comprehensive treatments. Therefore, further research is substantially critical for the accurate clinical determination of the biological behavior of these tumors and their prognostic evaluation. A need exists to develop individualized standards to determine the biological behavior of GIST, and the introduction of microscopic morphological indicators and the establishment of classification standards for malignant behavior that addresses GIST with different sites of origin have become particularly important.
Conflict of Interest
The authors declare no conflict of interest.
References
-
Chinese Diagnosis and Treatment Experts Group for Gastrointestinal Stromal Tumors
(2009) Chinese consensus in diagnosis and treatment of gastrointestinal stromal tumor. Zhonghua Bing Li Xue Za Zhi, 38, 697-702.
-
Comandone,
A. &
Boglione,
A.
(2005) Biology, diagnosis and therapeutic options in gastrointestinal stromal tumours. Minerva Chir., 60, 197-203.
-
Doyle,
L.A.,
Nelson,
D.,
Heinrich,
M.C.,
Corless,
C.L. &
Hornick,
J.L.
(2012) Loss of succinate dehydrogenase subunit B (SDHB) expression is limited to a distinctive subset of gastric wild-type gastrointestinal stromal tumours: a comprehensive genotype-phenotype correlation study. Histopathology, 61, 801-809.
-
Espinosa,
I.,
Lee,
C.H.,
Kim,
M.K.,
Rouse,
B.T.,
Subramanian,
S.,
Montgomery,
K.,
Varma,
S.,
Corless,
C.L.,
Heinrich,
M.C.,
Smith,
K.S.,
Wang,
Z.,
Rubin,
B.,
Nielsen,
T.O.,
Seitz,
RS.,
Ross,
D.T., et al.
(2008) A novel monoclonal antibody against DOG1 is a sensitive and specific marker for gastrointestinal stromal tumors. Am. J. Surg. Pathol., 32, 210-218.
-
Fletcher,
C.D.,
Berman,
J.J.,
Corless,
C.,
Gorstein,
F.,
Lasota,
J.,
Longley,
B.J.,
Miettinen,
M.,
O’Leary,
T.J.,
Remotti,
H.,
Rubin,
B.P.,
Shmookler,
B.,
Sobin,
L.H. &
Weiss,
S.W.
(2002) Diagnosis of gastrointestinal stromal tumors: A consensus approach. Hum. Pathol., 33, 459-465.
-
He,
D.M.,
Shi,
Y.,
Hou,
Y.Y.,
Hou,
J.,
Lu,
S.H.,
Liu,
Y.L.,
Xu,
C.,
Hu,
Q.,
Tan,
Y.S. &
Zhu,
X.Z.
(2012) Staging and histologic grading of gastrointestinal stromal tumors. Zhonghua Bing Li Xue Za Zhi, 41, 796-802.
-
Hou,
Y.Y.,
Zhu,
X.Z.,
Lu,
S.H.,
Zhou,
Y.,
Hou,
J.,
Tan,
Y.S.,
Shen,
K.T.,
Qin,
J. &
Sun,
Y.H.
(2010) Study on clinicopathologic parameters of malignant behavior in gastrointestinal stromal tumors. Zhonghua Bing Li Xue Za Zhi, 39, 325-331.
-
Joensuu,
H.
(2008) Risk stratification of patients diagnosed with gastrointestinal stromal tumor. Hum. Pathol., 39, 1411-1419.
-
Joensuu,
H.,
Vehtari,
A.,
Riihimaki,
J.,
Nishida,
T.,
Steigen,
S.E.,
Brabec,
P.,
Plank,
L.,
Nilsson,
B.,
Cirilli,
C.,
Braconi,
C.,
Bordoni,
A.,
Magnusson,
M.K.,
Linke,
Z.,
Sufliarsky,
J.,
Federico,
M., et al.
(2012) Risk of recurrence of gastrointestinal stromal tumour after surgery: an analysis of pooled population-based cohorts. Lancet Oncol., 13, 265-274.
-
Jung,
S.H.,
Suh,
K.S.,
Kang,
D.Y.,
Kang,
D.W.,
Kim,
Y.B. &
Kim,
E.S.
(2011) Expression of DOG1, PDGFRA, and p16 in Gastrointestinal Stromal Tumors. Gut Liver, 5, 171-180.
-
Laurini,
J.A. &
Carter,
J.E.
(2010) Gastrointestinal stromal tumors: a review of the literature. Arch. Pathol. Lab. Med., 134, 134-141.
-
Liegl,
B.,
Hornick,
J.L.,
Corless,
C.L. &
Fletcher,
C.D.
(2009) Monoclonal antibody DOG1.1 shows higher sensitivity than KIT in the diagnosis of gastrointestinal stromal tumors, including unusual subtypes. Am. J. Surg. Pathol., 33, 437-446.
-
Mazur,
M.T. &
Clark,
H.B.
(1983) Gastric stromal tumors. Reappraisal of histogenesis. Am. J. Surg. Pathol., 7, 507-519.
-
Miettinen,
M.,
Makhlouf,
H.,
Sobin,
L.H. &
Lasota,
J.
(2006) Gastrointestinal stromal tumors of the jejunum and ileum: a clinicopathologic, immunohistochemical, and molecular genetic study of 906 cases before imatinib with long-term follow-up. Am. J. Surg. Pathol., 30, 477-489.
-
Miettinen,
M.,
Wang,
Z.F. &
Lasota,
J.
(2009) DOG1 antibody in the differential diagnosis of gastrointestinal stromal tumors: a study of 1840 cases. Am. J. Surg. Pathol., 33, 1401-1408.
-
Tan,
C.B.,
Zhi,
W.,
Shahzad,
G. &
Mustacchia,
P.
(2012) Gastrointestinal stromal tumors: a review of case reports, diagnosis, treatment, and future directions. ISRN Gastroenterol., 2012, 595968.
-
Tworek,
J.A.,
Goldblum,
J.R.,
Weiss,
S.W.,
Greenson,
J.K. &
Appelman,
H.D.
(1999) Stromal tumors of the anorectum: a clinicopathologic study of 22 cases. Am. J. Surg. Pathol., 23, 946-954.
-
Wada,
N.,
Kurokawa,
Y.,
Nishida,
T.,
Takahashi,
T.,
Toyokawa,
T.,
Kusanagi,
H.,
Hirota,
S.,
Tsujinaka,
T.,
Mori,
M. &
Doki,
Y.
(2014) Subgroups of patients with very largegastrointestinal stromal tumors with distinct prognoses: a multicenter study. J. Surg. Oncol., 109, 67-70.
-
Yan,
H.,
Marchettini,
P.,
Acherman,
Y.I.,
Gething,
S.A.,
Brun,
E. &
Sugarbaker,
P.H.
(2003) Prognostic assessment of gastrointestinal stromal tumor. Am. J. Clin. Oncol., 26, 221-228.





