Abstract
The victims of the Great East Japan Earthquake and Tsunami have been forced to live in temporary housing, mainly by two different methods of resettlement: group allocation that preserved pre-existing local social ties and lottery allocation. We examined the effects of various factors, including the resettlement methods and social support, on mental health. From February to March 2012, we completed a cross-sectional survey of 281 refugees aged 40 years or older, who had lost their homes in the tsunami and were living in temporary housing in Iwanuma city. Psychological distress of the victims was assessed using the Kessler Psychological Distress Scale (K6) that consists of six self-reported items. Participants were also asked whether they had provided or received social support during this time. Participants were categorized as “providing social support” if they listened to someone else’s concerns and complaints, or “receiving social support” if they have someone who listened to their concerns and complaints. After adjusting for age and sex, multiple log-binomial regression analysis showed that participants without social support had a higher risk of psychological distress. Group allocation victims were more likely to receive social support than those who underwent lottery allocation. However, the resettlement approach did not significantly correlate with distress. Other factors associated with a higher risk of psychological distress were a younger age (55 or younger), living with either 3 people or 6 or more people, and having a lower income. The present results suggest that social support promotes the mental health of disaster victims.
Introduction
Disasters are an increasing public health concern (Noji 2005; Limpakarnjanarat and Ofrin 2009); in 2010 alone, there were 373 disasters around the globe, causing around 296,800 deaths (Centre for Research on the Epidemiology of Disasters: http://www.emdat.be/). The National Police Agency of Japan (https://www.npa.go.jp/archive/keibi/biki/higaijokyo_e.pdf) reported on March 11, 2011 that the Great East Japan Earthquake and Tsunami killed more than 15,000 people (with an additional 2,600 reported missing). The tsunami caused the destruction of more than 390,000 homes, forcing survivors to resettle into temporary housing. The disaster also caused physical and mental health problems (Moriyama and Kaga 2013; Ochi et al. 2013; Tuerk et al. 2013; Yamashita and Shigemura 2013) and disaster-related stressors (Shultz et al. 2013).
Residents of temporary housing face enormous psychological strain in coping with the loss of family, friends, and relatives; physical injury; changing living environments; loss of property and jobs; and the disruption of social networks. Because the coastal areas of Japan are at a higher risk of future tsunamis, local governments have restricted many victims from rebuilding their houses, and have instead created various plans to rebuild towns for the victims; these include developing new towns on mountainsides or building higher bases for new towns along the coasts. However, because these recovery plans will take several years to complete, victims are forced to live in temporary houses for an extended period. Being forced into temporary housing following a disaster has been documented as an important factor that determines how survivors recover (Yzermans et al. 2005; Neria et al. 2008; Uscher-Pines 2009; Tomiyasu et al. 2013; Tanimura et al. 2014).
Recent studies have highlighted the importance of social ties in disaster recovery (Nakagawa and Shaw 2004; Aldrich 2011; Tomiyasu et al. 2013; Xin et al. 2013; Tanimura et al. 2014). Aldrich (2011, 2012) showed that communities rich in social capital recovered more quickly after disasters. In addition, interpersonal connectedness is considered a key factor for mental health recovery in the short and middle terms after disasters (Hobfoll et al. 2007). In contrast, the disruption of social relationships among victims due to the disaster can exacerbate secondary traumas (Long and Wong 2012).
Following the earthquake and tsunami, Japanese municipal governments quickly began to build temporary housing structures. Two main methods were adopted to resettle victims into temporary housing. In the first approach, the victims were randomly allocated to temporary housing as housing became available, using a lottery system (lottery allocation). In the alternative approach, the local authorities attempted to preserve local social ties by moving members of a community together into the same flat of housing (group allocation). The former method is more straightforward for local governments from an operational perspective, but has the drawback of disrupting social ties within communities. In contrast, the latter approach preserves community ties (Tomiyasu et al. 2013), but involves longer delays to ensure that housing can be provided for everyone; furthermore, group allocation requires a considerably greater effort on the part of local governments. To our knowledge, no study has examined the effect of these two resettlement methods on the social support and mental health of survivors. Accordingly, our study sought to determine the impact of these resettlement approaches on social support and mental health, accounting for sociodemographic factors, among the relocated victims living in temporary housing in Miyagi, one year after the earthquake and tsunami.
Methods
Study setting
The present cross-sectional study was conducted in Iwanuma city as part of the Japan Gerontological Evaluation Study (JAGES) Project (Kondo 2010; Takeuchi et al. 2013). The JAGES project is an ongoing prospective cohort study investigating the social and behavioral factors associated with the loss of health. Iwanuma was a field site of the JAGES project. It is a coastal municipality in the Miyagi prefecture, about 50 km south of Sendai and 80 km west of the epicenter of the 3.11 earthquake (Ishigaki et al. 2013). Iwanuma suffered tremendous damage from the Great East Japan Earthquake and Tsunami, with 180 people killed by the tsunami (Ishigaki et al. 2013) and 48% (29 km2) of land inundated by seawater (Geospatial Information Authority of Japan: http://www.gsi.go.jp/common/000060371.pdf). Iwanuma city government exerted large efforts for group allocation for the disaster victims. The survey was conducted between February 27 and March 3, 2012. The study subjects were local residents aged 40 years or older who had lost their homes in the tsunami and were still living in temporary housing. Out of the original JAGES baseline sample, 504 subjects met the inclusion criteria and 376 (72.8%) participated in our questionnaire survey. Although missing responses on the Kessler Psychological Distress Scale (K6) (Kessler et al. 2002, 2003), mental health outcome composed by 6 questions, were imputed using the average score on the remaining K6 items, data from a further 95 subjects were excluded because of no responses to the K6 scale. Thus, the total number of subjects in these analyses was 281.
The study protocol was approved by the Research Ethics Committee of Tohoku University, Graduate School of Dentistry. All participants provided informed consent.
Outcome variable
The outcome variable, psychological distress, was assessed using the K6 scale. It consists of six self-reported items that assess the symptoms of serious psychological distress. The K6 has been used to screen for anxiety and other mood disorders. Specifically, the scale asks respondents how frequently they have experienced symptoms of psychological distress (e.g., “feeling so sad that nothing can cheer you up”) during the past 30 days. Responses to each item are recorded using a five-point Likert scale (0 = “all of the time,” 1 = “most of the time,” 2 = “some of the time,” 3 = “a little of the time,” and 4 = “none of the time”); the scores for each item are then summed to produce an overall score ranging from 0 (“no distress”) to 24 (“maximum distress”). A score of 13 points or higher on the K6 is considered equivalent to a score of less than 60 on the Global Assessment of Functioning (GAF) scale, according to previous research (Kessler et al. 2003). Therefore, we used this cutoff score of 13 as the definition of serious psychological distress. We used the Japanese version of the K6, which was developed through a standard back-translation procedure and has been validated (Furukawa et al. 2008). The internal consistency reliability (Cronbach’s alpha) for the K6 total score in our sample was 0.92.
Predictor variables
Two main resettlement approaches were used by municipal authorities: (1) victims were resettled en masse according to co-residence in the same communities before the earthquake and tsunami (group allocation) and (2) victims were randomly allocated to temporary housing (lottery allocation). We asked subjects to report the method of allocation (group or lottery allocation) in the questionnaire. Social support was measured using two items: “Do you have someone who listens to your concerns and complaints?” (categorized as ‘receiving social support’) and “Do you listen to someone else’s concerns and complaints?” (providing social support).
In addition, we inquired about sociodemographic factors, comorbid health conditions, and other risk factors for serious psychological distress. Demographic factors included sex, age, marital status, and number of people living together. Age was grouped into quartiles: 55 years or younger, 56-62 years, 63-71 years, and 72 years or older. Marital status was classified into five groups: married, widowed, divorced, never married, and other. The number of people living in the same temporary housing was categorized into six groups: living alone (answered 0 or 1) and 2, 3, 4, 5, or 6 people or more. For socioeconomic factors, participants were also asked about their annual household income and job status. Income was categorized as < ¥1000000, ¥1,000,000-1,999,999, ¥2,000,000-2,999,999, ¥3,000,000-3,999,999, and ≥ ¥4,000,000. Job status was categorized into six groups, as follows: 1 employment was not affected by the earthquake; 2 unemployed by the earthquake and still unemployed; 3 unemployed by the earthquake, but re-employed in the same occupation; 4 unemployed by the earthquake, but re-employed in another occupation; 5 unemployed before and after the earthquake (e.g., retired, homemaker); and 6 unemployed before the earthquake, but now employed. Current medical treatment and activities of daily living (ADL) were included as health status indicators. Current medical treatment was assessed using the question: “Are you receiving hospital-based treatment for any condition?” Subjects could answer “yes” or “no.” ADL was assessed with a single item: “Can you walk, take a bath, and use the toilet without assistance?” The answer was dichotomized into “no disability” and “some disability.”
Statistical analysis
To determine the associations between the resettlement approach and social support variables, cross-tabulation and chi-square analyses were performed. Multiple log-binomial regression analysis was then used to examine the associations between each variable and serious psychological distress (Barros and Hirakata 2003). In the initial models, sex and age were adjusted to examine how the resettlement approach and social support variables were associated with serious psychological distress (subjects with a K6 score of ≥ 13). In the multivariate adjusted model, we included all variables simultaneously. Missing answers for predictor variables were added into the models as dummy variables.
The significance level was set at 5% (two-tailed). We used STATA SE version 12.1 (Stata Corp., College Station, TX, USA) for all analyses.
Results
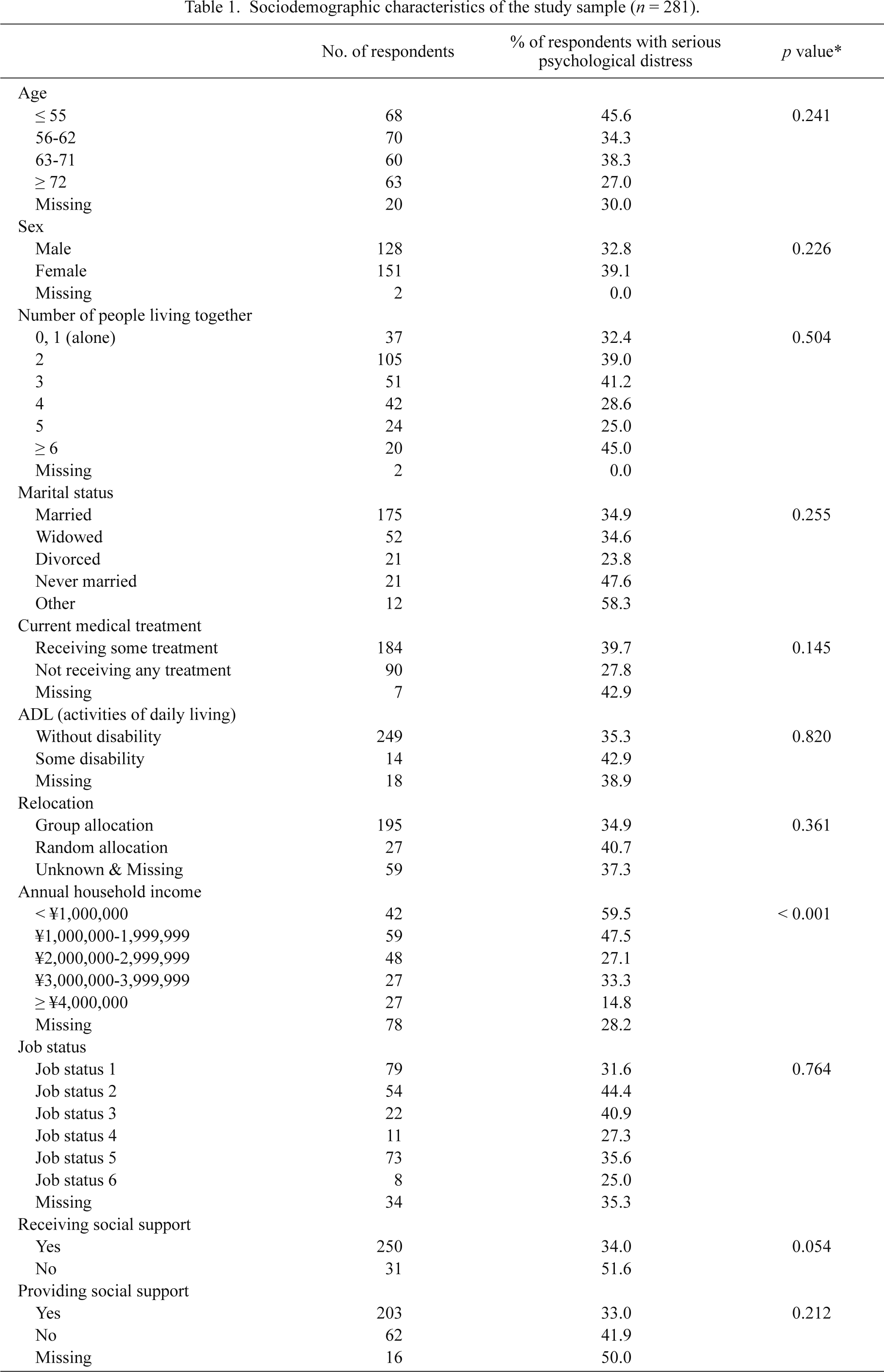
A total of 281 subjects were included in the present analyses. Even one year after the disaster, 101 subjects (35.9% of all respondents) were experiencing serious psychological distress, defined as scoring 13 points or higher on the K6. Table 1 shows the descriptive statistics. The prevalence of serious psychological distress among respondents who underwent group versus lottery allocation was 34.9% and 40.7%, respectively (p = 0.361). Respondents who reported higher psychological distress tended to be without social support, be younger, be receiving some form of medical treatment, and have a lower annual household income.
Fig. 1 shows the association between the resettlement approach and the presence of social support. Respondents who experienced group allocation to temporary housing were more likely to both provide social support to others and to receive social support, compared with the respondents who underwent lottery allocation (receiving social support: p = 0.003, providing social support: p = 0.050).
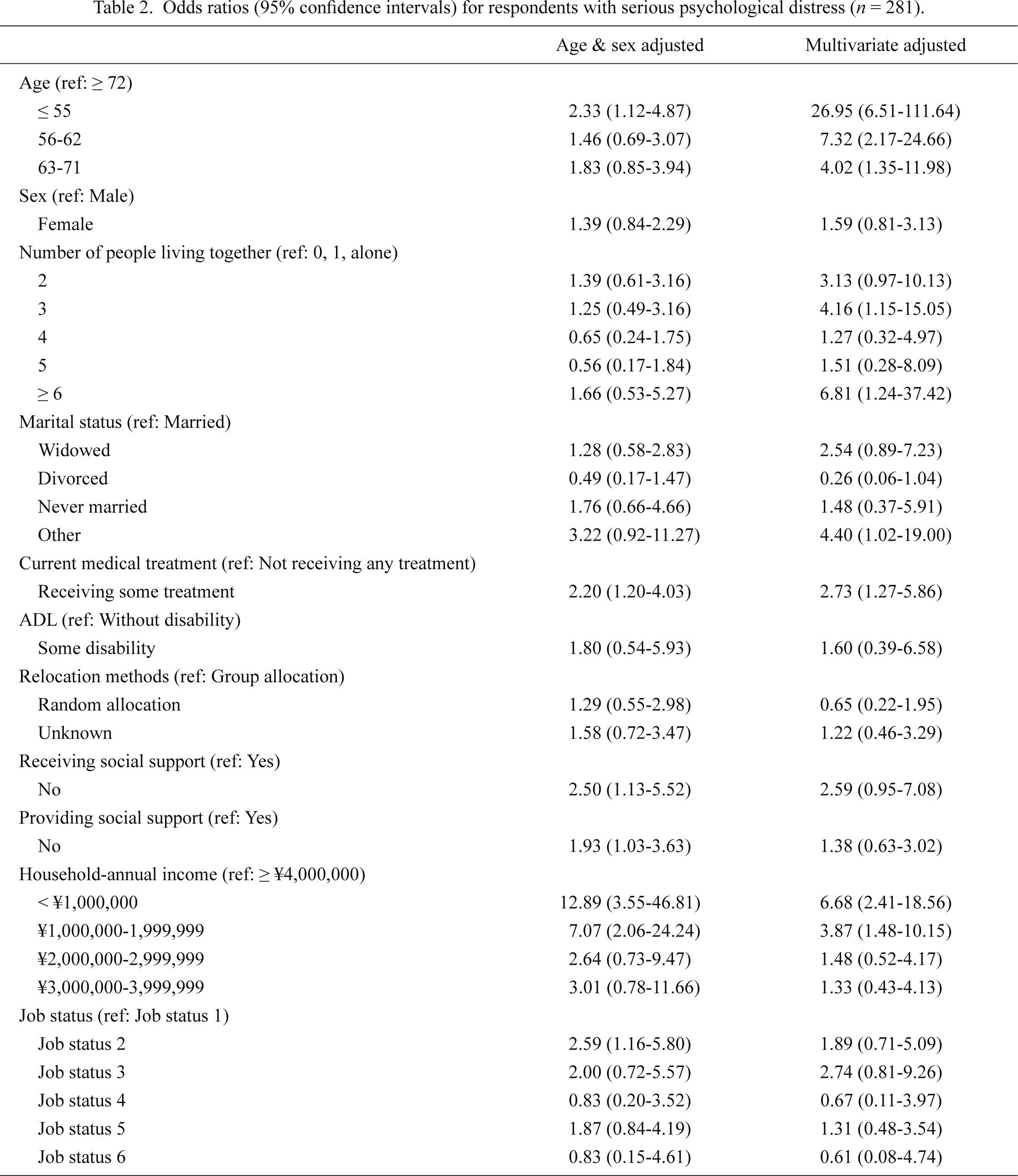
To examine the association between the resettlement approach and social support variables, age- and sex-adjusted log-binomial regression models were used (Table 2, age- and sex-adjusted model). Table 2 excluded missing variable. We found that the resettlement approach was not significantly associated with serious distress. However, respondents who reported that they were not receiving or providing social support were 2.50 and 1.93 times more likely to have serious psychological distress, respectively, compared with those who were receiving or providing social support. Other covariates partially explained the association between social support and mental health in the multivariate model. Factors associated with a higher risk of serious psychological distress were a younger age (55 or younger), living with either 3 people or 6 or more people, having other marital status, receiving medical treatment, and having a lower income.
Discussion
In the present study, we found that even one year after the disaster, 35.9% of refugees living in temporary housing reported serious psychological distress. Survivors who underwent group allocation to temporary housing (and were thus living in proximity to people who were their neighbors before the disaster) were significantly more likely to report receiving social support than those who underwent lottery allocation. Moreover, respondents who were receiving social support showed significantly lower psychological distress, although the resettlement approach was not significantly associated with distress.
Relocation due to disasters has been found to be an important health and social insolation risk factor for survivors, according to previous research (Yzermans et al. 2005; Neria et al. 2008; Uscher-Pines 2009; Tanimura et al. 2014). The present results suggest that the method of resettlement to temporary housing is an important predictor of access to social support. Relocation to temporary housing together with pre-disaster community members was significantly associated with higher social support. Thus, group resettlement appears to preserve the pre-disaster social networks of community members. Previous research has shown that social support is a key variable for reducing psychological distress in the aftermath of disasters (Galea et al. 2006; Neria et al. 2008; Kun et al. 2009; Nandi et al. 2009; Kikuchi et al. 2014; Ootsuka 2014). For future disaster preparedness, government authorities should take note of the findings of the present study.
Resettlement approach did not show a significant association with distress, despite it being associated with social support; however, participants who had experienced group allocation were less likely to report serious psychological distress than those who were randomly allocated (34.9% vs. 40.7%). This contradictory result might be explained by a lack of statistical power because of a smaller sample size. In addition, in temporary housing, volunteers and local government officials were available to offer support to victims, often organizing various events and visiting victims seeking support. It is possible that our questionnaire did not account for such support, which may explain the non-significant association between the resettlement approach and mental health.
Even one year after the disaster, a substantial number of subjects (35.9%) in our study reported mental health problems, defined as scoring 13 points or higher on the K6 scale. Among the general population of Japan, only 2.3% scored 13 or higher on the K6 scale (Sakurai et al. 2011). However, our survey coincided with the anniversary of the disaster, during which television and newspaper reports memorialized the victims of the earthquake and resultant tsunami. Previous studies have reported an increased prevalence of health problems after the broadcasting of past disasters (Yzermans et al. 2005; Beaudoin 2007). Therefore, media attention might have increased the psychological distress of subjects in the current study, meaning that our results may overestimate the prevalence of psychological distress. An expert review concluded that the requirements for mental health recovery in the short and middle terms after disasters included: (1) a sense of safety, (2) calmness, (3) a sense of self- and community efficacy, (4) connectedness, and (5) hope (Hobfoll et al. 2007). All respondents in our study lost their houses in the tsunami, and some of the respondents also lost their jobs. Moreover, because of the future tsunami risk, victims have not yet been allowed to rebuild their homes in the same coastal areas in which they had lived before the disaster. Recovery plans that promote economic security and enhanced hope, especially for younger generations, are now desperately needed.
In the present multivariate analysis, the social support variables did not show any significant associations with distress. Therefore, there may be mediating factors explaining the association between social support and psychological distress. In the model, people who were aged 55 or younger showed a 26.95 times higher risk of mental distress. People in this age group tended to have jobs, incomes, family members, and social support. Although these factors protect mental health, after adjusting for them in the model, younger people showed the highest risk of experiencing psychological distress. This may be because younger people live with their children and have to rebuild their homes. In a previous study, income and anxiety were found to be a major cause of insomnia after a disaster (Misawa 2014). Younger respondents tended to have more anxiety about their future, which caused psychological distress. In fact, we asked participants about their anxiety regarding the future, and 58.8% of younger people reported strong anxiety. In the 56-62, 63-71, and 72 or older age groups, the rates of strong anxiety reported were 48.6%, 48.3%, and 27.0% of participants, respectively.
This study has some limitations that should be noted. First, the number of subjects was relatively small, decreasing the robustness of our estimates and the stability of the model after adding various variables. Second, our survey did not inquire about seriously distressing life events, such as the death of friends or family members during the disaster.
Acknowledgments
The study was supported in part by the Japan Association of National Universities and the Earthquake Disaster Reconstruction and Revitalization of Japan Support Program at the Institute for Disaster Reconstruction and Regeneration Research and Grant-in-Aid for Scientific Research (B) (KAKENHI 24390469) from the Japan Society for the Promotion of Science. The funding bodies had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript. The authors thank Drs. Rika Ootsuka, Noriko Kawashima, Yuki Noguchi, Shin Yoshinaka, Ritsuko Wako, Shintaro Wakaguri, and Kenji Takeuchi for data collection and providing us with helpful comments on the research.
Conflict of Interest
The authors declare no conflict of interest.
References
-
Aldrich,
D.P.
(2011) The power of people: social capital’s role in recovery from the 1995 Kobe earthquake. Nat. Hazards, 56, 595-611.
-
Aldrich,
D.P.
(2012) Social Networks and Japanese Democracy: The Beneficial Impact of Interpersonal Communication in East Asia. Soc. Sci. Jpn. J., 15, 276-278.
-
Barros,
A.J. &
Hirakata,
V.N.
(2003) Alternatives for logistic regression in cross-sectional studies: an empirical comparison of models that directly estimate the prevalence ratio. BMC Med. Res. Methodol., 3, 21.
-
Beaudoin,
C.E.
(2007) News, social capital and health in the context of Katrina. J. Health Care Poor Underserved, 18, 418-430.
-
Centre for Research on the Epidemiology of Disasters
(2011) Disasters in Numbers. http://www.emdat.be/ [Accessed: October 9, 2014].
-
Furukawa,
T.A.,
Kawakami,
N.,
Saitoh,
M.,
Ono,
Y.,
Nakane,
Y.,
Nakamura,
Y.,
Tachimori,
H.,
Iwata,
N.,
Uda,
H.,
Nakane,
H.,
Watanabe,
M.,
Naganuma,
Y.,
Hata,
Y.,
Kobayashi,
M.,
Miyake,
Y., et al.
(2008) The performance of the Japanese version of the K6 and K10 in the World Mental Health Survey Japan. Int. J. Methods Psychiatr. Res., 17, 152-158.
-
Galea,
S.,
Hadley,
C. &
Rudenstine,
S.
(2006) Social context and the health consequences of disasters. Am. J. Disaster Med., 1, 37-47.
-
Geospatial Information Authority of Japan
(2011) Area of wetted surface from Tsunami disaster. http://www.gsi.go.jp/common/000060371.pdf [Accessed: October 9, 2014].
-
Hobfoll,
S.E.,
Watson,
P.,
Bell,
C.C.,
Bryant,
R.A.,
Brymer,
M.J.,
Friedman,
M.J.,
Friedman,
M.,
Gersons,
B.P.,
de Jong,
J.T.,
Layne,
C.M.,
Maguen,
S.,
Nearia,
Y.,
Norwood,
A.E.,
Pynoos,
R.S.,
Reissman,
D., et al.
(2007) Five essential elements of immediate and mid-term mass trauma intervention: empirical evidence. Psychiatry, 70, 283-315; discussion 316-369.
-
Ishigaki,
A.,
Higashi,
H.,
Sakamoto,
T. &
Shibahara,
S.
(2013) The Great East-Japan Earthquake and devastating tsunami: an update and lessons from the past Great Earthquakes in Japan since 1923. Tohoku J. Exp. Med., 229, 287-299.
-
Kessler,
R.C.,
Andrews,
G.,
Colpe,
L.J.,
Hiripi,
E.,
Mroczek,
D.K.,
Normand,
S.L.T.,
Walters,
E.E. &
Zaslavsky,
A.M.
(2002) Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol. Med., 32, 959-976.
-
Kessler,
R.C.,
Barker,
P.R.,
Colpe,
L.J.,
Epstein,
J.F.,
Gfroerer,
J.C.,
Hiripi,
E.,
Howes,
M.J.,
Normand,
S.L.,
Manderscheid,
R.W.,
Walters,
E.E. &
Zaslavsky,
A.M.
(2003) Screening for serious mental illness in the general population. Arch. Gen. Psychiatry, 60, 184-189.
-
Kikuchi,
K.,
Misawa,
J.,
Ootsuka,
R. &
Miura,
H.
(2014) Elderly people’s needs in Great East Japan Earthquake—from the investigation for community-based comprehensive support center. Geriatric Medicine, 52, 137-140.
-
Kondo,
K.
(2010) Health Inequalities in Japan: An Empirical Study of the Older People, Trans Pacific Press, Melbourne.
-
Kun,
P.,
Han,
S.C.,
Chen,
X.C. &
Yao,
L.
(2009) Prevalence and risk factors for posttraumatic stress disorder: a cross-sectional study among survivors of the Wenchuan 2008 earthquake in China. Depress. Anxiety, 26, 1134-1140.
-
Limpakarnjanarat,
K. &
Ofrin,
R.H.
(2009) Planning for and responding to public health needs in emergencies and disasters. In Oxford textbook of public health, 5th ed., edited by
Detels,
R.,
Beaglehole,
R.,
Lansang,
M.A. &
Gulliford,
M.
Oxford University Press, Oxford, pp. 1697-1706.
-
Long,
D. &
Wong,
Y.L.R.
(2012) Time bound: the timescape of secondary trauma of the surviving teachers of the Wenchuan Earthquake. Am. J. Orthopsychiatry, 82, 241-250.
-
Misawa,
J.
(2014) A study of relationship between insomnia and socioeconomic anxiety after the Great East Japan Earthquake: analysis of statistical social survey for residents in Sendai-City. The journal of applied sociology, 56, 17-31.
-
Moriyama,
K. &
Kaga,
M.
(2013) Mental healthcare efforts for the public after the Great East Japan Earthquake: “Guide to Good Mental Health for Those Affected by Natural Disasters” published by the Cabinet Office. Brain Dev., 35, 201-208.
-
Nakagawa,
Y. &
Shaw,
R.
(2004) Social capital: a missing link to disaster recovery. Int. J. Mass Emerg. Disasters, 22, 5-34.
-
Nandi,
A.,
Tracy,
M.,
Beard,
J.R.,
Vlahov,
D. &
Galea,
S.
(2009) Patterns and predictors of trajectories of depression after an urban disaster. Ann. Epidemiol., 19, 761-770.
-
National Police Agency of Japan
(2014) Damage Situation and Police Countermeasures associated with 2011 Tohoku district—off the Pacific Ocean Earthquake. https://www.npa.go.jp/archive/keibi/biki/higaijokyo_e.pdf [Accessed: October 9, 2014].
-
Neria,
Y.,
Nandi,
A. &
Galea,
S.
(2008) Post-traumatic stress disorder following disasters: a systematic review. Psychol. Med., 38, 467-480.
-
Noji,
E.K.
(2005) Public health in the aftermath of disasters. BMJ, 330, 1379-1381.
-
Ochi,
S.,
Murray,
V. &
Hodgson,
S.
(2013) The great East Japan earthquake disaster: a compilation of published literature on health needs and relief activities, march 2011-september 2012. PLoS Curr., 5.
-
Ootsuka,
R.
(2014) Association between care risk and social support for elderly people in temporary housing residence. Geriatric Medicine, 52, 137-140.
-
Sakurai,
K.,
Nishi,
A.,
Kondo,
K.,
Yanagida,
K. &
Kawakami,
N.
(2011) Screening performance of K6/K10 and other screening instruments for mood and anxiety disorders in Japan. Psychiatry Clin. Neurosci., 65, 434-441.
-
Shultz,
J.M.,
Forbes,
D.,
Wald,
D.,
Kelly,
F.,
Solo-Gabriele,
H.M.,
Rosen,
A.,
Espinel,
Z.,
McLean,
A.,
Bernal,
O. &
Neria,
Y.
(2013) Trauma signature analysis of the great East Japan disaster: guidance for psychological consequences. Disaster Med. Public Health Prep., 7, 201-214.
-
Takeuchi,
K.,
Aida,
J.,
Kondo,
K. &
Osaka,
K.
(2013) Social participation and dental health status among older Japanese adults: a population-based cross-sectional study. PLoS One, 8, e61741.
-
Tanimura,
Y.,
Yoshimi,
K. &
Higuchi,
K.
(2014) The influence of maintaining social capital of community and the use of the ICT on the social isolation of residents of temporary shelters in the Great East Japan Earthquake. The Japan Society of Information and Communication.
-
Tomiyasu,
R.,
Imoto,
S.,
Otsuki,
T.,
Nishide,
K.,
Cho,
S.-e.,
Okamoto,
K.,
Koizumi,
H.,
Goto,
J. &
Kano,
T.
(2013) Proposal and practice of ‘COMMUNITY-CARE TEMPORARY-HOUSING’. AIJ J. Technol. Des., 19, 671-676.
-
Tuerk,
P.W.,
Hall,
B.,
Nagae,
N.,
McCauley,
J.L.,
Yoder,
M.,
Rauch,
S.A.,
Acierno,
R. &
Dussich,
J.
(2013) Forty days after the Great East Japan Earthquake: field research investigating community engagement and traumatic stress screening in a post-disaster community mental health training. Int. J. Psychiatry Med., 45, 159-174.
-
Uscher-Pines,
L.
(2009) Health effects of relocation following disaster: a systematic review of the literature. Disasters, 33, 1-22.
-
Xin,
H.,
Aronson,
R.E.,
Lovelace,
K.A.,
Strack,
R.W. &
Villalba,
J.A.
(2013) Resilience of Vietnamese refugees: resources to cope with natural disasters in their resettled country. Disaster Med. Public Health Prep., 7, 387-394.
-
Yamashita,
J. &
Shigemura,
J.
(2013) The Great East Japan Earthquake, tsunami, and Fukushima Daiichi nuclear power plant accident: a triple disaster affecting the mental health of the country. Psychiatr. Clin. North Am., 36, 351-370.
-
Yzermans,
C.J.,
Donker,
G.A.,
Kerssens,
J.J.,
Dirkzwager,
A.J.,
Soeteman,
R.J.H. &
ten Veen,
P.M.
(2005) Health problems of victims before and after disaster: a longitudinal study in general practice. Int. J. Epidemiol., 34, 820-826.