Abstract
Students of the Tohoku University School of Medicine experienced the Great East Japan Earthquake on March 11, 2011. We conducted a series of surveys to examine the relationships among their experiences and activities on the day of the earthquake, their physical, mental, and economic problems following the disaster, and how their problems changed over time. The initial survey was performed in April 2011, with three follow-up surveys in July 2011, February 2012, and April 2013. The initial survey focused on students’ experiences and living conditions during the disaster, which contained questions on their locations and circumstances, family circumstances, lives after the earthquake, voluntary works, physical or mental health problems, and desire for counseling. The follow-up surveys included new items regarding their circumstances, changes in their health problems, and their desire for economic assistance. Students who answered the first survey to the 4th one, with response rates in the following bracket, were as follows: 472 (28.0%), 640 (29.9%), 681 (36.0%), and 678 (39.0%), respectively. Six months after the earthquake, about 20% having experienced physical and/or mental problems. Although there was a trend toward a reduction in suffering and health problems over time, some students’ conditions remained unchanged or worsened. It is notable that students who had participated in voluntary activities, despite their own suffering of harm and distress, were identified as the group that required the closest attention. Our present results can be applied to appropriate supports for students in future large-scale disasters.
Introduction
The “2011 off the Pacific Coast of Tohoku Earthquake,” also known as the Great East Japan Earthquake, occurred at 14:46 on March 11, 2011, with the epicenter off the Sanriku coast, approximately 70 km east of Sendai in Miyagi Prefecture, where Tohoku University is located. Seismic intensities of the magnitude 9.0 earthquake were recorded at 7 in Kurihara City in the same prefecture and slightly under 6 at Tohoku University (Japan Meteorological Agency 2013).
The disaster inflicted substantial damage across a broad area from Tohoku to the Kanto region, as the earthquake also caused a large tsunami, liquefaction, and land subsidence. In addition, the earthquake and tsunamis caused the Fukushima Daiichi nuclear disaster in the neighboring prefecture of Fukushima. Two years after the disaster (at the time of the writing of this article on September 9, 2013), 18,703, 2,674, and 6,220 people were recorded as deceased, missing, and injured, respectively, as a result of the Great East Japan Earthquake (Shibahara 2011). In addition, many victims were forced to live in evacuation shelters, with the total number of evacuees (as of January 9, 2015) from Miyagi and the neighboring prefectures of Iwate and Fukushima recorded at 61,355 (Fire and Disaster Management Agency 2013; National Police Agency 2015).
When the earthquake struck, Tohoku University School of Medicine students of all departments, with the exception of third-year medical students, were absent due to the spring break; therefore, when they returned to begin the new term, it was critical to understand how they had been affected by the disaster, and whether they had experienced physical or psychological difficulties. For students in the graduate school, understanding these issues was important in the context of whether they would be able to continue their studies. Students from the Tohoku region comprise a large proportion of the university’s student body, and considering the possibility that family finances were devastated, data were required to understand the impact of the disaster on each student. Moreover, given the reports in the literature regarding various experiences that can result in trauma for victims of this type of large-scale disaster, we believed that a considerable number of students would have been exposed to traumatic situations (Kin and Onuma 2012; National Center of Neurology and Psychology 2012).
It is therefore essential to survey the students’ experiences of the disaster quickly and act without delay to improve their situations via interventions such as mental health care and economic assistance. Furthermore, given the inevitability that resolution of the many problems arising from a disaster of this scale would occur over a long period, we implemented a series of surveys over time.
The purpose of this research was to investigate the aftermath and devastating effects of the Great East Japan Earthquake, as follows: 1) the physical, mental, and economic problems that arose for students; 2) physical and mental problems associated with students’ experiences and activities at the time of the disaster; and 3) the long-term impact of the disaster on the students and how this changed over time. Furthermore, we examined the survey results to determine the types of response that should be considered by educational and other institutions when large-scale disasters occur in the future.
In addition, when students requested assistance during the implementation of the surveys, the survey sponsors provided either direct assistance or resources, such as counseling services, scholarships, or economic assistance, to enable students to address their problems independently.
Methods
Survey participants
In Japan, undergraduate systems for students who will participate in medical care in the future are as follows. (1) Medical doctors’ license can be obtained after the state examination, and only those who are authorized such as graduation of the 6-year course of education in medical schools can take this state examination. “The Department of Medicine” in this study corresponds to such medical school. (2) “The Department of Health Sciences” in our university has a 4-year program, and students who wish to be nurses, radiation technologists, or clinical laboratory technologists are studying to take a state examination.
At our graduate school, a wide variety of students are studying including medical doctors (MDs) and others, but most of the graduate students are MDs.
We implemented a series of surveys involving undergraduate and graduate students from the Tohoku University School of Medicine between 2011 and 2013. Second- to fourth-year health sciences students were not included in Survey 1, as we were unable to obtain the agreement of the board of the Department of Health Sciences. After 2012, data from new students were excluded because they completed a different questionnaire from that completed by the other students. In addition, data from those who graduated from our medical school in each year were also excluded in this study.
Survey methodology and content
We implemented four surveys in April 2011, July 2011, February 2012, and April 2013 to examine the students’ experiences of the disaster. The survey questionnaire items included: 1) consent to participate in the survey; 2) year of study, school ID, and name; 3) location at the time of the disaster; 4) experiences during the disaster; 5) experiences of those close to them (e.g., family members); 6) post-disaster changes in experience; 7) post-disaster living situation; 8) participation in voluntary activities (yes/no); 9) voluntary activity location, content, and duration; 10) physical distress (yes/no); 11) mental distress (yes/no); 12) changes in physical/mental health since the disaster; 13) desire for counseling (yes/no); and 14) other (free response). It was hypothesized that, as time passed after the disaster, the students’ experiences would change; therefore, the four survey questionnaires were created using different combinations of these items, as appropriate for the timing of each survey. Respondents were permitted to leave questions unanswered, and we stated clearly that students who did not consent to survey participation would remain entitled to counseling assistance for any problems experienced.
The questionnaires were distributed at orientation events for new academic terms and in other situations in which students were assembled, including classes. If graduate students were absent from the campus and could not receive the questionnaire directly, we requested that the office of the department to which the student belonged forward it to the student via mail. An envelope was provided for confidentiality, and a collection box was permanently located in the medical department office to ensure that the envelopes containing the questionnaires could be returned at any time.
Survey sponsors
The Tohoku University School of Medicine Office of Medical Education drew the draft, and the Medical Department’s Student Welfare Committee brushed up to finalize the questionnaires. The tabulation and analysis of the results were performed by the authors.
Analysis methodology for the survey results
The data were analyzed using contingency table tests for independence (chi-square tests), and residual analyses were performed to determine the differences between cells in contingency tables of 3 or more data categories. The p values for the residual analyses (Haberman, 1973) were: p < 0.01 for r > 2.58 and p < 0.05 for r > 1.96. IBM SPSS® Statistics 21.0 was used to perform the chi-square tests and residual analyses. In addition, the relationships between the responses to the question “How did people close to you fare in the disaster?” (“Someone was harmed,” “Home and property were damaged,” and “Domestic finances became difficult”) and the survey items “I have physical distress,” “I have mental distress,” and “I participated in voluntary activities” (yes/no responses for all 6 items) were analyzed using covariance structure analysis (Kano and Miura 2002; Toyoda 2007) and data mining (cluster analysis and association analysis) (Agrawal et al. 1993; Yamaguchi et al. 2004).
Covariance structure analysis
We used covariance structure analysis to analyze the relationships between factors underlying the multivariate data measures. We performed an exploratory factor analysis with covariance structure analysis using a model configured with latent variables and the following 6 items: “Someone was harmed,” “Home and property were damaged,” “Domestic finances became difficult,” “I experience physical distress,” “I experience mental distress,” and “I participated in voluntary activities.” Exploratory factor analysis was performed using a Markov chain Monte Carlo (MCMC) method with IBM SPSS® Amos 21.0 software.
Cluster analysis
Cluster analysis is a classification method for grouping data with similar characteristics within a sample consisting of several variables. In this study, it was used to divide the sample into groups (clusters) to understand the results of the other analyses more clearly via examination of group characteristics. There is a disadvantage to cluster analysis, in that the researcher is able to determine the number of clusters at will, which can lead to arbitrary results. However, we adopted a method to prevent this—namely, using the two-step cluster analysis procedure, which automatically determines the most suitable number of clusters. We also used the Akaike (AIC) and Bayesian information criteria (BIC) in the algorithm. IBM SPSS® Statistics 21.0 was used to perform the two-step cluster analysis.
Association analysis
Association analysis is a type of data mining that enables the effective generation of rules relevant to the occurrence of B (Consequent) given the occurrence of A (Antecedents) in a database, by finding database “itemsets” (item combinations) of value from an infinite number of itemsets. The strength of the rules is evaluated according to measured support, confidence, and lift. We used IBM SPSS® Modeler14.2 to perform this analysis.
Ethical considerations
Because questions included in this survey could cause participants to re-experience the disaster, which could lead to re-traumatization, care was taken to ensure that students did not feel forced to participate. Before beginning the survey, students were provided with a thorough explanation and asked to participate only if they agreed with the survey’s purpose. A summary of the study was published on the university’s medical department website, and the participants’ right to withdraw from the study, even after receiving the survey, was emphasized.
With respect to participation in voluntary activities, we informed all participants that their participation in voluntary activities would not affect their futures or student evaluations. We also established a procedure to anonymize the data, as the surveys included participants’ names. We also stipulated that, should the results be published, used in academic presentations, or made publicly available, the anonymity of the data would be scrupulously maintained.
This study was approved by the Ethics Committee of Tohoku University Graduate School of Medicine (Registration number 2013-1-151) and the student welfare committee at the university’s medical department.
Results
Survey response rates and composition
Table 1 shows the numbers of surveys distributed and returned for each of the four surveys. The four surveys were distributed to a total of 2,669 undergraduate and graduate students who attended Tohoku University School of Medicine between 2011 and 2013 (excluding data from students who just enrolled in a course in 2012 and 2013), and 1,383 (51.8%) returned at least one survey.
Because the survey questions were designed to facilitate understanding of the students’ experiences during the disaster and subsequent changes in those experiences, such as those involving physical and mental health, combinations of questions were selected for each survey to reflect the passage of time. As a result, the sets of questions in the four questionnaires varied according to the timing of the surveys, as shown in Table 2.
Survey participants’ experiences during the earthquake
Table 3 shows the students’ locations when the earthquake occurred. Overall, “other” was the largest category, followed by “home” and “hometown.” The breakdown of “other” responses showed that, because the earthquake occurred during the spring break, many students were away from the campus, travelling, shopping, or attending club training camps. Looking at data from the academic department, the order of the frequencies for medical students’ locations during the disaster was similar to that of the remainder of the sample (“other,” followed by “home” and “hometown”). However, many of the fourth-year students (third-year students at the time of the disaster) were in one of the lecture halls attending a mock academic conference, which is part of the regular curriculum. For health sciences students, “home” was the most frequent response, followed by “other” and “hometown.” In contrast, many of the graduate students had been in hospitals during the earthquake, and as a result, “other” was followed by “regional hospital” and “university hospital.” The breakdown of “other” for graduate students showed that there were also cases in which the participants had been at a research facility or other workplace when the disaster occurred. As a possible anomaly in the data, it is likely that first-year health science students (who had not yet entered university at the time of the disaster) erred in choosing “university lecture building,” perhaps meaning they had been in a high school or preparatory school lecture hall.
Table 4 shows that 476 students experienced loss, injury, or damage to their surroundings during the disaster, much of which was due to damage to homes and property. The proportion of students who experienced the destruction of buildings, injury to themselves or others was approximately 5%, these were possible sources of trauma. The results of a chi-square test examining department affiliation and each type of disaster-related harm suggested a possible relationship between department and “at least half of a building was destroyed,” “only the household fixtures and furniture were damaged,” “there was hardly any damage,” and “other damage,” as independence was rejected at the 1% level. Adjusted residuals, relative to the expected values, were significantly higher when the residual was positive and lower when it was negative. The residual analysis p values were: for p < 0.01 for r > 2.58 and p < 0.05 for r > 1.96. As 20% or more of all cells displayed an expected frequency of less than 5, “you were harmed or wounded” and “someone else was harmed” fell outside the suitability level for a chi-square test. The frequency for “at least half of a building was destroyed” was significantly high for graduate students but nonsignificant for medical and health sciences students. Of the students who indicated that “only fixtures and furnishings were damaged,” the incidence of the response was highest for graduate students, followed by health science students, while it was very low for medical students. Of the students who indicated that “there was hardly any damage,” the frequency of the response was high for medical students, low for graduate students, and nonsignificant for health science students. The frequency of “other damage” was high for graduate students, low for medical students, and nonsignificant for health science students.

Table 5 shows students’ participation in voluntary activities; 35.4% of the students participated in voluntary activities within 6 months of the disaster. The result of a chi-square test to examine the relationship between academic department and voluntary activity participation was significant. According to the residual analysis, the frequency of participation in voluntary activities was significantly high for medical students, significantly low for health science students, and nonsignificant for graduate students. Voluntary activities consisted mainly of clearing tsunami debris, operating evacuation shelters, and sorting and distributing relief goods. There were also students who provided assistance with medical treatment on behalf of the medical school (Table 6).
Experience of harm to student finances and individuals close to students
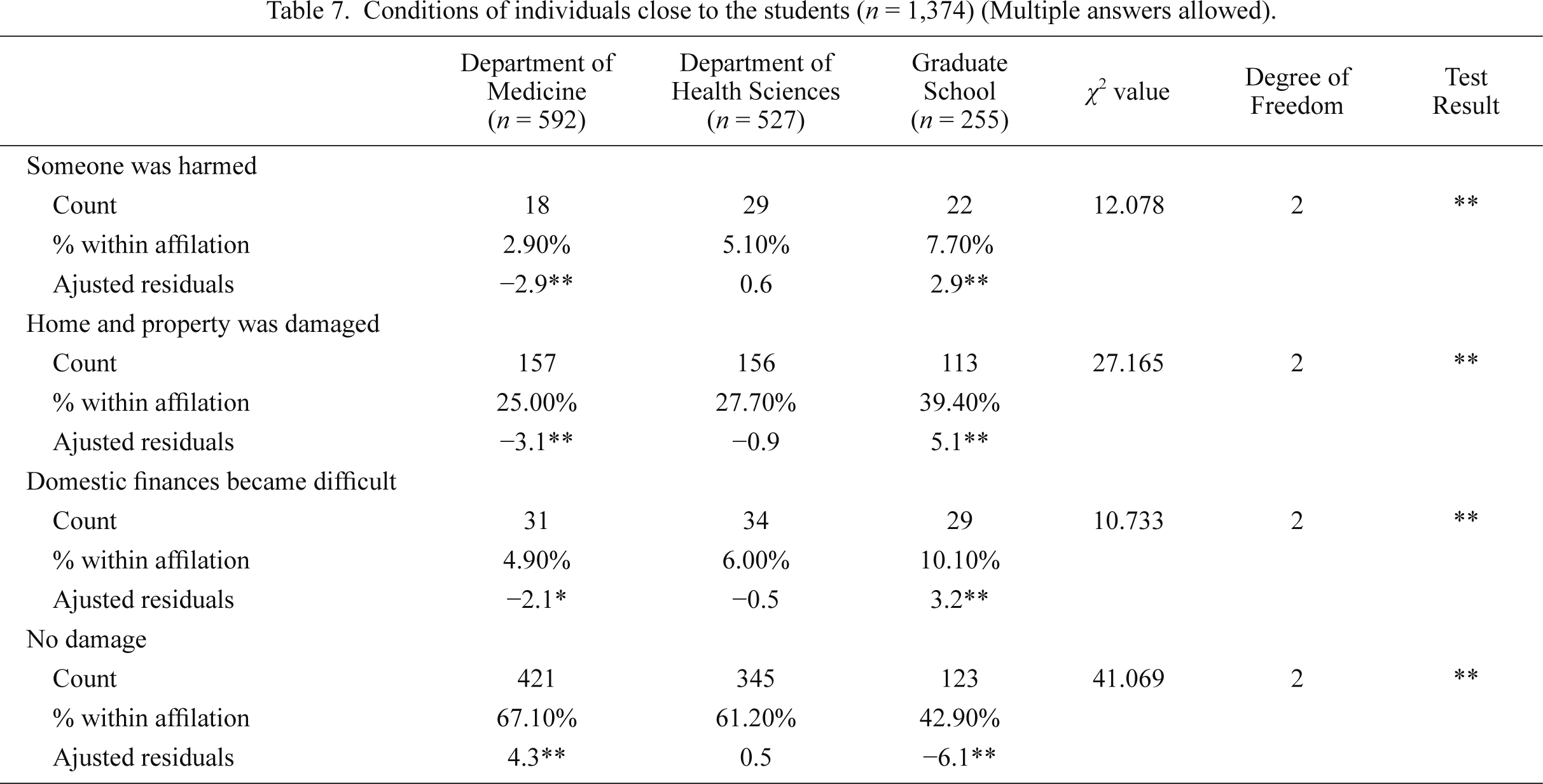
Table 7 shows the students’ experiences of harm to their finances and individuals close to them. About 40% of the students indicated that those close to them were disaster victims, and 6.4% of all respondents indicated that they experienced difficulties with their domestic finances as a result of the disaster. The results of a chi-square test examining department affiliation and each questionnaire item were significant. According to the residual analysis, frequencies for “someone was harmed,” “home and property was damaged,” and “domestic finances became difficult,” were significantly high for graduate students and significantly low for medical students. The frequencies for “no damage” were significantly high for medical students and significantly low for graduate students. Frequencies for both items were nonsignificant for health science students.
Disaster-related harm, physical distress, mental distress, and desire for counseling
Table 8 shows the numbers of student responses indicating disaster-related harm, physical distress, and mental distress for each of the four surveys. The results of chi-square tests examining each of the three items by survey were significant, and frequencies for each item in Survey 4, conducted two years after the disaster, were significantly small, while at least 50% of the students had been affected by some type of disaster-related harm 6 months after the disaster.
Table 9 shows how students’ responses regarding their experiences of disaster-related harm and physical and mental distress changed with time after the disaster. The results of chi-square tests examining the trends in disaster-related harm and physical and mental distress were significant. The results demonstrated that each type of problem gradually decreased in the year following the disaster, although physical and mental distress took two years to resolve. However, the results also showed that a small number of students’ experiences of problems remained unchanged or worsened; further, approximately 20% of the students who were experiencing physical and mental distress did not improve over time. The results of chi-square tests examining harm status according to survey and distress status were significant for all surveys (Table 10), suggesting that students who experienced disaster-related harm complained of physical or mental distress more frequently relative to students who had not experienced harm.
Table 11 shows the responses to items concerning the desire for counseling for each survey. In Surveys 1-3, 3-4% of students required (desired or already received) counseling. The results of chi-square tests examining the three responses regarding desire for counseling for each survey were significant. Residual analysis indicated that, for Survey 1, “no desire” was chosen most frequently, followed by “desire” and “already receiving.” In contrast, for Surveys 2, 3, and 4, “no desire” was chosen most frequently, followed by “already receiving” and “desire”.
Associations between experience of disaster-related harm, physical and mental distress, and participation in voluntary activities
In order to examine the relationships between “someone was harmed,” “home and property was damaged,” “domestic finances became difficult,” “I experience physical distress,” “I experience mental distress,” and “I participated in voluntary activities,” we performed a covariance structure analysis, a cluster analysis, and an association analysis.
Covariance structure model
In the covariance structure analysis, we examined several models to identify the most suitable and chose a four-level cause-and-effect sequence model (Fig. 1). The three observed variables, “someone was harmed” (personal harm), “home and property were damaged” (building damage), and “domestic finances became difficult” (financial problems), were assigned to Level 1, and latent variables, which were not observed directly, were assigned to Levels 2 and 3. Of the observed variables, we hypothesized that the latent variables represented “impediments to daily living” and “disaster stress” and formulated a partial least squares (PLS) model, assigning the observed variables “I experience physical distress” (physical distress), “I experience mental distress” (mental distress), and “I participated in voluntary activities” (voluntary activity participation) to Level 4. Because these data were expressed as categorical or binary variables, we used Bayesian estimation. As a result, the model’s suitability level, indicated by the posterior predictive distribution probability, was p = 0.39 (p values approaching 50% indicate suitability; and conversely, values approaching zero indicate that the model has low predictive utility). In the figure, the error notations e1-e4 indicated a possibility that factors outside the observed and hypothesized latent variables may have affected each variable. The effects of “personal harm,” “building damage,” and “financial problems,” on “impediments to daily living” were 1.669, 1.043, and 1, respectively, indicating that the effect of personal harm was the strongest. In addition, “disaster stress” affected “physical distress” and “mental distress” at ratios of 0.591 and 1, respectively. The relationship between “impediments to daily living” and “disaster stress” (0.137) demonstrated that there were some students for whom physical or mental distress was affected by an increase in disaster stress when daily living was affected by some type of harm. Finally, the relationship between disaster stress and voluntary activity participation (0.104) indicated that some of the students who were experiencing disaster stress had participated in voluntary activities.

To understand these phenomena more clearly, the sample data were grouped via cluster analysis and examined. The results classified the students into the following five groups (Table 12).
Cluster 1: A group of 40% of the students who reported no harm or distress did not participate in voluntary activities.
Cluster 2: A group of 13% of the students with various combinations of personal harm, building damage, financial problems, physical or mental distress, and voluntary activity participation.
Cluster 3: A group of 18.7% of the students, who suffered no harm or distress and participated in voluntary activities.
Cluster 4: A group of 12.5% of the students with combinations of absence of personal harm, financial problems, or physical distress and presence of building damage, mental distress, and participation in voluntary activities.
Cluster 5: A group of 15.8% of the students, who only suffered building damage and did not experience physical or mental distress or participate in voluntary activities.
The five groups each showed distinct characteristics: Clusters 1, 3, and 5 did not exhibit physical or mental distress, while Clusters 2 and 4 complained of physical or mental distress or both. Cluster 2, in particular, was recognized as the group that required the most attention, because members not only experienced harm and physical or mental distress, which required intervention, but also tended to participate in voluntary activities.
Association analysis (possible motivation for participating in voluntary activities)
We performed an association analysis to generate rules according to department to determine which sets of response conditions were related to “voluntary activity participation,” “physical distress,” and “mental distress.” In the rule generation, in order to avoid producing a large number of rules and as a cutoff for rule strength, threshold values were set at 5% for support and 50% for confidence, and the maximum number of conditions in an itemset was set to 5. When no rules that exceeded the threshold values were generated, the confidence threshold was lowered to 30-40% and the analysis repeated. The rules that were generated are shown in Table 13. All of the rules generated yielded consequent voluntary activity participation. None had consequences of physical or mental stress. In Survey 1, when medical students had experienced building damage but no physical or mental distress or other harm, a cause-and-effect relationship with participation in voluntary activities was shown at support values of 16-21% and confidence values of 50%. When health science students had experienced building damage and graduate students had experienced building damage and mental distress but no other harm, a cause-and-effect relationship was also indicated. However, in the graduate student rules, support was less than 6%, which was low relative to the rules for the other departments, and the confidence value was 40%, which was also somewhat low. In Survey 2, the medical students’ main possible motivation for participation in voluntary activities was the experience of building damage, with a rather high confidence value of 45%, and although support was low, the experience of financial problems may also have been a strong motivation for participation in voluntary activities. Although confidence values in the 30% range were rather low, for health sciences students, voluntary activity participation may have been motivated by having experienced building damage but not by physical or mental distress. For the graduate students, experience of mental distress, financial problems, and building damage combined to form various reasons for participating in voluntary activities, each with a 5-10% support value and confidence values exceeding 50%.

Discussion
Based on the results of a series of four surveys completed by undergraduate and graduate students at Tohoku University School of Medicine following the March 11, 2011 Great East Japan Earthquake, this study investigated the frequencies of and interrelations between direct and indirect types of harm suffered by students, the effects of the disaster on their mental and physical health, and related behaviors.
The Great East Japan Earthquake occurred on a weekday afternoon, during which almost all of the undergraduate students were absent from the campus due to the spring break. Although the locations at which they experienced the disaster consequently differed, at least 40% of the students were at the university, in the university hospital, at home near the university, or in regional hospitals. This proportion was even larger for graduate students, of whom approximately 70% experienced the earthquake in these locations. With respect to the other students, 20% of the medical students and 25% of the health science students were from affected communities. While the hometowns of the students differed somewhat from year to year, many resided in affected areas; for example, of the students who enrolled at the university in 2012, approximately 40% and 73% of the medical and health sciences students, respectively, were from the Tohoku region. Of these students, approximately 67% of the medical students and 56% of the health sciences students were from Iwate, Miyagi, or Fukushima prefectures, which sustained extensive damage due to the disaster (e.g., the tsunami; from the 2012 Guide to the Tohoku University School of Medicine). Therefore, approximately 27-40% of the undergraduate students who had reported that they had returned home were believed to have experienced the disaster in these heavily affected areas. It is also likely that 27-40% of the homes and workplaces of the families responsible for the students’ tuition and living expenses were located in these areas, and it was highly likely that the graduate students paying their own living expenses and tuition fees would have lost their place of employment. In fact, in these surveys, the proportion of students for whom the continuation of their studies became financially difficult was highest among graduate students, at around 10%, relative to 5-6% of undergraduates. These frequencies were relatively low considering the enormity of the disaster; however, should this type of widespread disaster occur in the future, the following particularly important points should be considered: such students require assistance quickly in order to continue their studies, and the frequency of the problem may differ according to department.
The results suggested that the disaster affected the students in a large variety of ways. In this disaster, many students from the affected areas were exposed to life-threatening experiences as the long, strong tremors demolished furniture and buildings; in addition, they were forced into evacuation, as the entire infrastructure that supports daily living was lost for an extended period of time following the earthquake. Because transportation and communications were paralyzed, students who had been traveling had no means of returning home and could only worry about the safety of their families and friends. Foreign students who experienced difficulty communicating in Japanese were forced to evacuate without being able to obtain sufficient information. Students working in hospitals were forced into action on the front lines of post-disaster treatment without power or other infrastructure while also required to keep patients safe. Individuals in areas impacted by tsunamis were likely to have found themselves in crisis situations in which they witnessed people and homes being swept away. According to a report by Kin and Onuma (2012), events that can traumatize victims include the following: encountering events involving certain death; actual physical experiences of harm, such as pain or being burned; witnessing death and injury; loss of family members or friends; loss of identity related to the loss of bodily functions, community, financial income, or occupation; inability to live life as usual; and exposure to various kinds of information due to evacuation or relocation. In addition, it has been reported that the feeling of the earth shaking beneath one’s feet increases the likelihood of psychological trauma (National Center of Neurology and Psychology 2012). Research has also shown that survivors may suffer “survivor’s guilt”; that is, they may feel guilty about surviving, being uninjured, or having lost little relative to others. Furthermore, when the acute phase of a disaster is over, survivors may look back on their behavior and feel guilty about what they did or did not do (Underwood 2005). Considering the disaster experiences of students described above, this research suggests that all of the students in this study may have experienced psychological trauma to a greater or lesser degree, regardless of whether they were victims, because the areas affected were fundamental parts of their lives. The results of every survey conducted during the approximate 25-month study period showed high proportions of individuals complaining of physical or mental distress. The frequency of physical or mental distress was highest in Survey 2 (four months after the disaster), followed by Survey 1 (one month after the disaster), suggesting that interventions are urgently required soon after a disaster occurs. It is notable that incidence of students with mental distress after the Great East Japan Earthquake was 20% and that observed in the Vietnam and Iraq war veterans with PTSD was 30% (Weiss et al. 1992; Hoge et al. 2006). Incidence was similar but slightly small in the present case than veterans; repetitive stress in the latter may be the main reason for such difference. While comparisons of the incidence of harm and physical or mental distress clearly showed that disaster victims were more likely to exhibit distress, every survey also showed that students who did not directly damaged also suffered from distress, suggesting that they were strongly affected by traumatic factors other than suffering disaster-related harm.
The association rules generated during data mining showed that experiencing building damage was a possible motivation for participation in voluntary activities, as it was the most frequently generated of all harm conditions in the rule antecedents across all academic departments. In Survey 2, in addition to building damage, experiencing financial problems was also generated as a rule antecedent. In contrast, experiencing personal harm was not generated as a condition related to participation in voluntary activities. In addition, of the two types of distress, mental distress was generated as a possible motivation for participating in voluntary activities, but physical distress was not. The explanation for these results could be that there are two different ways in which mental attitudes are affected, according to the nature of the harm: property loss or damage can be understood as a temporary problem, enabling expectations of resolution over time; however, there may be no resolution of personal loss or injury, even with the passage of time. Personal harm exerted the strongest effect on impediments to daily living in the results of the covariance structure analysis; an example of this effect may be that domestic financial problems could stem from loss of family income or parents or guardians, and for graduate students, the workplace. Similar to the phenomena in the association analysis, these were serious problems that the students were powerless to resolve, which may have affected interest in participating in voluntary activities. The reason that physical distress was not generated as a condition for participating in voluntary activities may have been that it would have been difficult to do so while experiencing headaches and nausea. However, the cluster analysis showed that some of the 13% of students who were in Cluster 2 participated in voluntary activities, even while suffering personal harm and physical distress, conditions that were not generated in relation to voluntary activity participation in the association analysis. Other possible reasons for motivation for participating in voluntary activities may have been that students were encouraged to do so by the people around them; they wanted to see the affected areas (Gakusei Borantia Kenkyukai 2012 (in Japanese)); or they had experienced a sense of mission as students affiliated with a school of medicine. However, students exhibiting physical and mental distress and behaving in this way should be observed particularly closely, because they could be tormented by the sight of casualties or feelings of loss while participating in voluntary activities in tsunami-damaged areas. In contrast, any intervention to restrict participation in voluntary activities should be undertaken cautiously because of the possibility that the individual may suffer survivor’s guilt at a later date. Therefore, cluster analysis of continuously collected data to identify students belonging to the group most at risk (Cluster 2) may improve intervention effectiveness.
The survey performed two years after the earthquake demonstrated that problems involving harm and mental and physical distress were, relatively speaking, progressing toward resolution; however, it also showed that some students were exhibiting a six-month delay in onset of symptoms resulting from stress factors listed in the post-traumatic stress disorder diagnostic criteria (American Psychiatric Association 2000). This suggests a need to continue surveying this population in the longer term.
While considering how long we should continue these surveys, we thought that we should initiated this kind of survey shortly after the occurrence of the disaster to help the mental health care for our students. We think that this attempt gave benefits for medical students. Thanks to this early implementation, funding was received from many institutions, and scholarships could be offered to students in need, pre-empting the formation of barriers to their continued study. We included spaces for free responses in the surveys, and in response to feedback from foreign students indicating that they did not know how to secure disaster counseling services or evacuation shelters, we created maps in English showing the relevant locations near the university. Therefore, by capturing the needs of students early and being able to progress toward the resolution of their problems, it was possible to alleviate their anxiety. Furthermore, the various analyses of factors in this study, which investigated the possibility of future problems occurring as a result of harm, distress, and behavior patterns, facilitated the preparation of appropriate interventions, even when students had not asked for assistance. This may have contributed to the prevention of the exacerbation of problems in the long term. Finally, because we were able to contact students who were interested in counseling swiftly and formulate plans to address their problems, we may have been able to prevent a secondary disaster resulting from the mental and physical challenges and various other problems caused by the first disaster.
Study limitations
The questions in this study included items regarding trauma, which could be considered invasive; therefore, students who did not wish to remember the disaster were able to choose to not participate. In addition, we were unable to distribute the surveys to some of the graduate students directly, due to their absence from the campus, and they may have been unable to respond to the survey if they were busy providing medical treatment or conducting around-the-clock research. Further, in the first survey, because second-, third-, and fourth-year students in the health sciences were excluded, we only received responses from the first-year students, and this may have affected our present study. It was not possible to further analyze on differences by gender because we did not collect such data. The survey questionnaires included items regarding participation in voluntary activities; however, some of the graduate students were providing treatment in the affected areas as medical staff, which was neither considered a voluntary activity nor included in the survey questions. Studies have been conducted to examine the effects of the disaster on the mental and physical health of veteran medical practitioners who were engaged in treatment activities in affected areas (Yamazaki and Tanno 2009) however, they were unable to determine how graduate students were affected. Future surveys should include the question “Did you perform any treatment in disaster areas as a member of a medical team?” and a survey of psychological factors related to survivor’s guilt, such as whether the respondents participated in voluntary activities and, if not, whether they had wanted to but had been unable to do so.
Acknowledgments
We would like to thank the following people for their guidance, without which we would not have completed this research: Associate Professor Seiichi Ishii and Associate Professor Junichi Kameoka of the Tohoku University Graduate School of Medicine, Office of Medical Education; Professor Naoto Ishii of the Department of Microbiology and Immunology; Associate Professor Seiichi Saitoh of the Kobe University Graduate School of Human Development and Environment; Instructor Yoshimi Suzukamo of the Tohoku University Department of Physical Medicine and Rehabilitation for her guidance on the analysis methodology. In addition, we would like to express our sincere appreciation to the Tohoku University School of Medicine’s Medical Student Welfare Committee, the school affairs office, and the students for the support we received in conducting the surveys.
Conflict of Interest
The authors declare no conflict of interest.
References
-
Agrawal,
R.,
Imielinski,
T. &
Swami,
A.
(1993) Mining association rules between sets of items in large databases. ACM SIGMOD Record, 22, 207-216.
-
American Psychiatric Association
(2000) Diagnostic and Statistical Manual of Mental Disorders, 4th ed., Amer Psychiatric Pub, Arlington, VA.
-
Fire and Disaster Management Agency
(2013) The 2011 Tohoku Earthquake (Great East Japan Earthquake), Report no. 148. http://www.fdma.go.jp/bn/higaihou/pdf/jishin/148.pdf [Accessed: December 9, 2014].
-
Gakusei Borantia Kenkyukai
(2012) Bulletin: Summary Report of the Disaster Volunteer Survey. https://sites.google.com/site/gfsovas/research/questionnaireaboutvolunteeractivitiesbystudent [Accessed: December 9, 2014].
-
Haberman,
S.J.
(1973) The analysis of residuals in cross-classified tables. Biometrics, 29, 205-220.
-
Hoge,
C.W.,
Auchterlonie,
J.L. &
Milliken,
C.S.
(2006) Mental health problems, use of mental health services, and attrition from military service after returning from deployment to Iraq or Afghanistan. JAMA, 295, 1023-1032.
-
Japan Meteorological Agency
(2013) The 2011 off the Pacific Coast of Tohoku Earthquake. http://www.jma.go.jp/jma/en/Publications/publications.html [Accessed: December 9, 2014].
-
Kano,
Y. &
Miura,
A.
(2002) Graphical Multivariate Analysis Using AMOS, EQS, and CALIS: Visualizing Covariance Structure Analysis, Gendai-Sugakusha, Kyoto (in Japanese).
-
Kin,
Y. &
Onuma,
A.
(2012) Disaster mental health treatment and understanding trauma. Occup. Ment. Health., 20, Special Supplement, 2-9.
-
National Center of Neurology and Psychology
(2012) Disaster Mental Health Guidelines. http://cocorocare.jp/n/guideline/guideline/ [Accessed: December 9, 2014].
-
National Police Agency
(2015) Countermeasures for the Great East Japan Earthquake (NPA). http://www.npa.go.jp/archive/keibi/biki/index_e.htm [Accessed: January 18, 2015].
-
Shibahara,
S.
(2011) The 2011 Tohoku earthquake and devastating tsunami. Tohoku J. Exp. Med., 223, 305-307.
-
Toyoda,
H.
(2007) Covariance Structure Analysis: Structural Equation Modeling, Tokyo Tosho, Tokyo (in Japanese).
-
Underwood,
P.
(2005) Survivor’s guilt: understanding the aftermath of disaster. J. Jpn. Soc. Disaster Nurs., 7, 23-30 (in Japanese).
-
Weiss,
D.S.,
Marmar,
C.R.,
Schlenger,
W.E.,
Fairbank,
J.A.,
Jordan,
B.K.,
Hough,
R.L. &
Kulka,
R.A.
(1992) The prevalence of lifetime and partial post-traumatic stress disorder in Vietnam theater veterans. Journal of Traumatic Stress, 5, 365-376.
-
Yamaguchi,
K.,
Takahashi,
J. &
Takeuchi,
A.
(2004) Understanding the Basics and Structure of Multivariate Analysis: An Introduction to a Technique for Analyzing Large Databases, Shuwa System, Tokyo (in Japanese).
-
Yamazaki,
T. &
Tanno,
H.
(2009) Stress Responses of nurses in the 2004 Niigata-Ken Chuetsu Earthquake. J. J. Disast. Med., 14, 157-163.