Regular Contribution
Virtual Reality Training with Cognitive Load Improves Walking Function in Chronic Stroke Patients
2015 Volume 236 Issue 4 Pages 273-280
Details
2015 Volume 236 Issue 4 Pages 273-280
Virtual reality training is considered as an effective intervention method of stroke patients, and the virtual reality system for therapeutic rehabilitation has emphasized the cognitive factors to improve walking function. The purpose of current study was to investigate the effect of virtual reality training with cognitive load (VRTCL) on walking function of chronic stroke. Chronic stroke patients were randomly assigned to the VRTCL group (11 patients, including 5 men; mean age, 60.0 years; post-stroke duration, 273.9 days) or control group (11 patients, including 2 men; mean age, 58.6 years; post-stroke duration, 263.9 days). All subjects participated in the standard rehabilitation program that consisted of physical and occupational therapies. In addition, VRTCL group participated in the VRTCL for 4 weeks (30 min per day and five times a week), while those in the control group participated in virtual reality treadmill training. Walking function under single (walking alone) and dual task (walking with cognitive tasks) conditions was assessed using an electrical walkway system. After the 4-week intervention, under both single and dual task conditions, significant improvement on walking function was observed in VRTCL and control groups (P < 0.05). In addition, in the dual task condition, greater improvement on walking function was observed in the VRTCL group, compared with the control group (P < 0.05). These findings demonstrated the efficacy of VRTCL on the walking function under the dual task condition. Therefore, we suggest that VRTCL may be an effective method for the achievement of independent walking in chronic stroke patients.
The recovery of walking ability has been recognized as a major goal of stroke rehabilitation, and 60-80% of stroke patients can walk independently after discharge from the hospital (Kelly-Hayes et al. 2003). However, according to previous studies on community ambulation, only 7% of stroke survivors resume valued activities in the home and community (Goldie et al. 1996; Park et al. 2011). In addition, therapeutic interventions performed in clinical or hospital settings are difficult to provide varied environmental factors, such as ambient conditions, terrain characteristics, and traffic level or a complex external environment for stroke patients (Carvalho et al. 2010; Lee et al. 2015). Because environmental factors act as critical determinants for the level of community ambulation of stroke patients (Lord et al. 2006), environmental factors must be considered when designing stroke rehabilitation programs aimed at improving community ambulation (Yang et al. 2008). Thus, many previous studies have included environmental factors in the therapeutic intervention and have demonstrated that training that combines environmental factors with walking is effective in the recovery of community ambulation (Lord et al. 2008; Stuart et al. 2009).
Recently, virtual reality training involving community environments is as an effective intervention for improving community ambulation of stroke patients (Yang et al. 2008; Kizony et al. 2010; Walker et al. 2010; Cho and Lee 2013, 2014). Virtual reality allows interaction between the user and a computer interface to produce real time simulation via multisensory feedback (Adamovich et al. 2009; Laver et al. 2012). In addition, virtual reality offers opportunities to increase the patient’s participation and motivation through interaction with environments similar to the real world (Kizony et al. 2010).
Several studies on virtual reality training with stroke patients have reported positive outcomes. Fung et al. (2006) demonstrated that a virtual reality treadmill system for gait training was effective in improving walking speed and the ability to learn to walk on a slight slope for stroke patients, and Yang et al. (2008) found that treadmill training combined with a virtual community environment improved the walking ability of stroke patients. Another study investigated the effectiveness of treadmill training combined with a real world video recording in patients with chronic stroke, and they reported improvements in walking ability after training for 6 weeks (Cho and Lee 2014).
Currently, there is a growing interest in cognitive factors during the performance of community walking in stroke rehabilitation (Yang et al. 2007a). Virtual reality training systems has been emphasizing the cognitive factors as part of the therapeutic intervention (Kizony et al. 2010; Koenig et al. 2011). Kinzony et al. (2010) reported that the evaluation of cognitive load is important in walking training of stroke, and particularly, the evaluation of cognitive load should be included as part of a routine stroke rehabilitation program. Accordingly, the purpose of the current study was to investigate the effect of virtual reality training with cognitive load (VRTCL) on walking function in chronic stroke patients. We hypothesized that patients with chronic stroke would show improvements in walking function after VRTCL.
This study used a randomized pre- and post-test control group design. We used G*power 3.1.7 software to calculate the sample size. In this study, the mean power was set at 0.8 and the alpha error at 0.05. According to the analysis of G*power software, the total of 27 subjects were required at least; thus 28 subjects were chosen during the training period.
Twenty eight chronic stroke patients were recruited for this study. All subjects met the following inclusion criteria: (1) hemiparesis resulting from a single stroke, (2) chronic phase (at least 6 months post stroke), (3) able to walk 10 m with and without the use of an assistive device, (4) able to understand and follow simple verbal instructions (Korean version of the Mini Mental State Examination score > 24) and (5) no severe heart disease or uncontrolled hypertension. The exclusion criteria were: (1) orthopedic and other conditions that influence walking, such as arthrosis or total hip joint replacement, (2) participation in other studies or rehabilitation programs, and (3) pre-existing neurological disorders. Prior to data collection, we explained the objectives and requirements of our study to all participants, and all patients provided informed consents prior to the participation. The experimental procedures were in compliance with the ethical committee of Myongji Choonhey Hospital (IRB No. MJCHIRB - 2014 - 002).
Study protocolsBased on the calculation of the sample size using G*power software, 28 chronic stroke patients were recruited in this study; however, four of the 28 subjects were excluded for the following reasons. First, even though the cognitive level met the inclusion criteria (Korean version of the Mini Mental State Examination score > 24), two subjects were not able to understand verbal instructions for the study, and two other subjects refused to participate in the study. As a result, the total of 24 chronic stroke patients was selected as study subjects.
After the pretest, 24 subjects were randomly assigned to two groups using sealed envelopes (marked on the inside with a 1 or 2): (1) the VRTCL group (n = 12) and (2) the virtual reality training (VR) group (n = 12). During the intervention period, one subject in each group dropped out due to discharge. Thus, 11 subjects from each group were included in the final analysis. Study processes are shown in Fig. 1; and all subjects participated in a training program for 4 weeks after the pretest. The posttest was conducted 3 days after the end of the intervention period. All measurements were performed while patients were in the rehabilitation ward, and the assessor was blind to training condition. All subjects participated in the same standard rehabilitation program, which consisted of conventional physical and occupational therapies. Conventional physical therapy, including exercises for increased trunk stability, lower extremity muscle strength, and gait ability, was performed for 4 weeks (30 min a day and 5 times a week). Occupational therapy, an upper extremity training program to practice activities of daily living, was performed for 4 weeks (30 min a day and 5 times a week). In addition, subjects participated in the VRTCL for 4 weeks (30 min a day and 5 times a week), while subjects in the control group participated in a VR program for 4 weeks (30 min a day and 5 times a week). The procedures for the VRTCL and VR groups were conducted in a different therapeutic room to maintain subject blinding. All subjects successfully completed the study protocol and the attendance rate was 100% for the 4-week intervention.
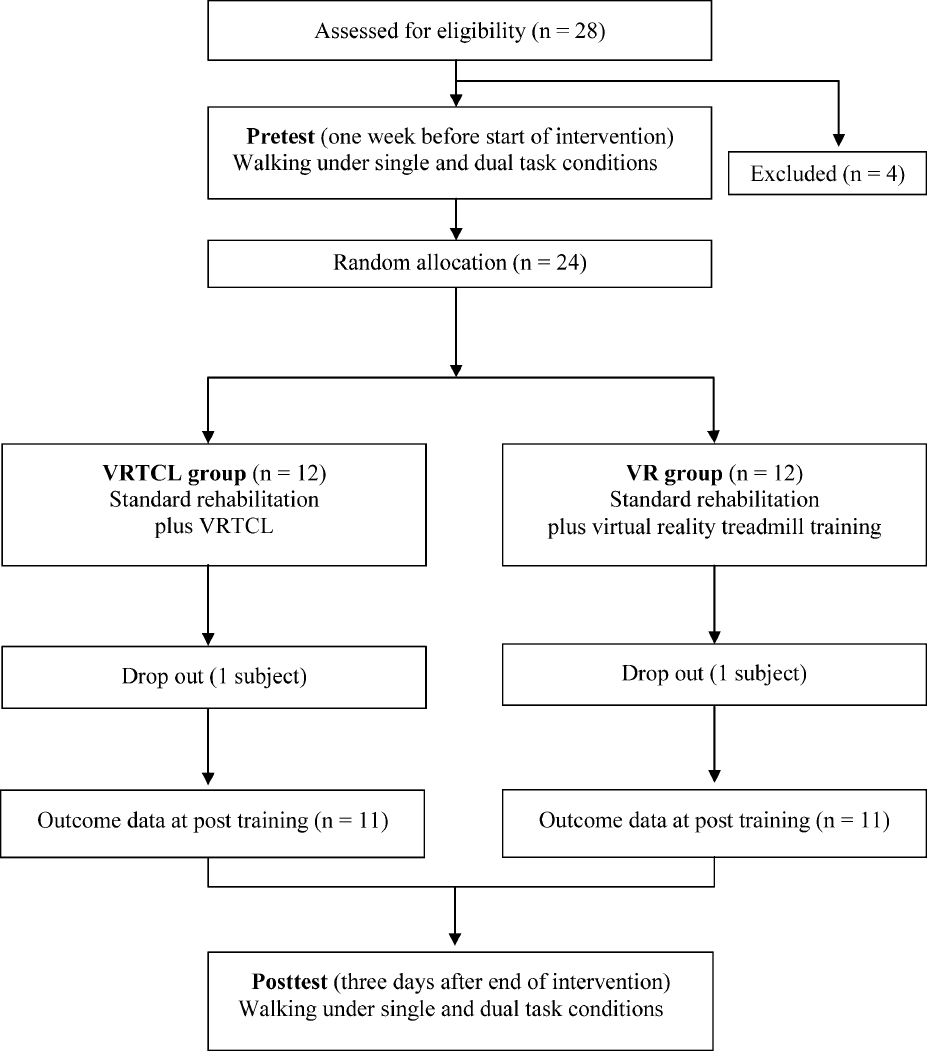
Flow diagram of the study.
Total 24 subjects were randomly assigned to two groups: the virtual reality training with cognitive load (VRTCL) group (n = 12) and the virtual reality training (VR) group (n = 12). During the intervention period, one subject in each group dropped out due to discharge. Thus, 11 subjects from each group were included in the final analysis.
The VRTCL was performed using a treadmill (FITEX T-5050, Korea, 2007) with an overhead harness system (CBJH1 8000000004, LINAK, Denmark, 2009). The overhead harness was used only for safety purposes, but not for supporting body weight. The virtual reality environment was projected onto an 1,800 × 1,900 mm (width × length) screen in front of the treadmill (1 m) using a projector (EB-97, EPSON, Japan, 2010) and a laptop (Fig. 2). At the same time, loudspeakers were connected to the laptop to provide auditory input. The treadmill belt speed and the virtual reality scene movement were synchronized in three levels (1.6, 2.4 and 3.2 km/h). Depending on the change of treadmill belt speed, the virtual reality scene movement speed was changed. While walking on the treadmill, subjects viewed the virtual environment and performed cognitive load task.
In this study, the virtual environment was configured with a video recording of a real community environment including elements such as a crosswalk, garden and a marketplace, and the virtual environment video was played for 30 min. The cognitive load task performed within the virtual environment was composed of four cognitive tasks including memory, arithmetic, and verbal tasks. According to previous studies (Bowen et al. 2001; van Iersel et al. 2007; Kizony et al. 2010), these secondary cognitive tasks cause dual task gait decrement (dual task gait decrement means the deterioration of walking ability caused by perform cognitive task and walking simultaneously).
The four cognitive load tasks were each performed for 1 week during the intervention period. In the first week, the memory task was used as cognitive load task. During the 30-min VRTCL, familiar objects such as an apple, an umbrella, and flowers appeared in the virtual environment video (one object per a minute) and subjects were asked to remember the objects from the virtual environment video and their recollection was tested after the training session. In the second week, the arithmetic task was used as a cognitive load task. During the 30-min VRTCL, simple addition and subtraction problems were provided in the virtual environment video (one problem per a minute). In the third week, a verbal task that involved citing words that start with letters presented on the screen such as, “가, 바 and 아” (가, 바 and 아 means first syllable of the following word: 가방 (bag), 바지 (pants) and 아들 (son)), was used as a cognitive load task. During the 30-min VRTCL, letters were shown in the virtual environment video (one letter per a minute). In the fourth week, another verbal task (casual conversation with the assistant) was used as a cognitive load task. During the 30-min VRTCL, simple casual conversation (for example, what did you eat for breakfast?) was progressed with assistant during VRTCL. Subjects participated in the total 20 sessions over 4 week’s period, which include a total of 30-min walking during each session. Even though rest breaks were upon request, it was not included in the overall walking time.
In the control (virtual reality alone) group, the speed and duration of treadmill walking and virtual environment video were controlled using the same method used in the VRTCL group, but the cognitive load task were not performed.

Setting for the virtual reality training with cognitive load.
The virtual reality training with cognitive load program was performed using a treadmill with an overhead harness system. The virtual reality environment was projected onto the screen in front of the treadmill. The virtual environment was configured with a video recording of a real community environment including elements such as a crosswalk, garden and marketplace.
Walking function (spatio-temporal gait parameters) under single and dual task conditions was measured using the GAITRite walkway system. (GAITRite, CIR System Inc., New Jersey, USA). The GAITRite is a portable gait analysis tool for the automated measurement of spatio-temporal gait parameters. The system captured the spatio-temporal gait parameters and was connected to a computer. It consisted of an 810 × 89 × 0.625 cm (length × width × height) instrumented mat with 27,648 embedded pressure sensitive sensors spaced 1.27 cm apart and arranged in a 48 × 576 grid. The active area of the mat is approximately 7.32 m long and 0.61 m wide. The sampling rate was 80 Hz and the data obtained were analyzed using gait analysis software (GAITRite GOLD version 3.2b, CIR System Inc., New Jersey, USA). The measurement of gait parameters using the GAITRite system was performed based on published guidelines in a quiet closed room without auditory or visual interference (Kressig and Beauchet 2006; Cho et al. 2015). In accordance with a previously published study (Cho et al. 2015), the spatio-temporal gait parameters were measured under two conditions: (1) walking alone (single task) and (2) walking while counting backward (dual task). The instructions for each test condition were as follows: (1) “Please walk at your usual speed, now!” and (2) “Please walk at your usual speed while counting backward from the presented number.” To prevent a learning effect, subjects were only informed of the start number just before the measurement and each measurement was given a different number. The subjects initiated and terminated walking for a minimum of 3 m from the start to the end of the walkway in order to maintain gait speed on the mat. A verbal command was given to initiate walking, and one of the examiners accompanied the subjects to prevent them from falling while walking. Subjects were allowed to use assistive devices that were used during testing. All values were averaged over three trials. The gait parameters recorded were velocity, cadence, paretic side step length, and stride length.
Statistical analysesStatistical analysis was performed using SPSS 18.0 version. The Shapiro-Wilk test was used to confirm the normal distribution of all outcome variables. Groups were compared at baseline using t tests for independent samples for continuous variables and Chi-squared tests for categorical data. All outcome variables were normally distributed; therefore, we chose analysis of variance with repeated measures with a between subject factor at 2 levels (the two groups) and a within subject factor at 2 levels (the time: pre-intervention and post-intervention). The interaction of group and time determined the efficacy of the VRTCL on the outcome measures. Statistical significance was accepted for P values less than 0.05.
A summary of the general characteristics of the 22 subjects with chronic stroke who fulfilled the inclusion criteria for the study is shown in Table 1. No significant differences in baseline values were observed between the experimental and control groups.
Table 2 shows the gait analysis with the single task condition. Both groups showed a main effect of time on gait speed (F = 185.131, P = 0.000), cadence (F = 103.505, P = 0.000), step length (F = 59.967, P = 0.000), and stride length (F = 58.873, P = 0.000). However, the group × time interaction was not significant for any variables.
Table 3 shows the gait analysis with the dual task condition. Both groups showed a main effect of time on gait speed (F = 10.265, P = 0.004), cadence (F = 61.681, P = 0.000), step length (F = 43.813, P = 0.000), and stride length (F = 74.277, P = 0.000). In addition, significant differences were observed for the group x time interactions for gait speed (F = 5.905, P = 0.025), cadence (F = 45.093, P = 0.000), step length (F = 26.975, P = 0.000), and stride length (F = 34.516, P = 0.000).

Homogeneity test for general characteristics and dependent variables of the subjects.
Values are expressed as n or Mean ± SD.
VRTCL, virtual reality training with cognitive load; VR, virtual reality training; BMI, body mass index; MMSE-K, Mini Mental State Examination-Korea; BBS, berg balance scale.
*Chi-square test, +Independent-t test.
A summary of the general characteristics of the 22 subjects with chronic stroke who fulfilled the inclusion criteria for the study is shown. No significant differences in baseline values were observed between the VRTCL and VR groups.

Gait analysis with single task condition.
Values are expressed as Mean ± SD.
VRTCL, virtual reality training with cognitive load; VR, virtual reality training.
*significant differences between pre- and post-test, P < 0.05.
After 4 weeks of intervention, significant improvement on walking function was observed in both VRTCL and control groups (P < 0.05).

Gait analysis with dual task condition.
Values are expressed as Mean ± SD.
VRTCL, virtual reality training with cognitive load; VR, virtual reality training.
*significant differences between pre- and post-test, P < 0.05.
+significant differences between ADTVR group and VR group, P < 0.05.
After 4 weeks of intervention, in dual task condition, greater improvement on walking function was observed in the VRTCL group compared with the VR group (P < 0.05).
The specific aim of the current randomized controlled study was to examine whether the VRTCL could produce more beneficial effects on walking function under single and dual task conditions than compared to the virtual reality alone. Overall walking function in the single task condition significantly improved for the both the VRTCL and virtual reality groups.
Interactive virtual reality systems designed to simulate the real environment provide an enriched environment for motor relearning for stroke patients (Adamovich et al. 2009). Virtual reality has been used in neurological rehabilitation to enhance upper and lower extremity function as well as cognition and the performance of activities of daily living (Laver et al. 2012). The virtual reality training including real environmental situations can provide effective simulated practice for functional walking tasks (Kwakkel et al. 2004; Cho and Lee 2013; Laver et al. 2012). In addition, by providing real time feedback and controlling the level of difficulty, virtual reality systems can optimize the motor relearning process for walking function (Sveistrup 2004). Kim et al. (2009) demonstrated that IREX virtual reality training using a video capture system could be incorporated into conventional rehabilitation programs to advance walking function in chronic stroke patients. Another study reported that treadmill training within a virtual environment displayed on a screen improved community walking function in stroke patients (Yang et al. 2008). In this way, many previous investigations (Yang et al. 2008; Kim et al. 2009; Cho and Lee 2014) have demonstrated the beneficial effects of virtual reality on walking function in stroke patients; therefore, it is not surprising that enhancements of walking function under the single task condition was observed in this study.
However, although many previous studies have provided positive clinical evidence for the effectiveness of virtual reality on walking function in stroke patients, it still remains unclear whether virtual reality has an additional effect when it is combined with cognitive overload. In this study, we found that overall walking function under the dual task condition improved significantly more in the VRTCL group compared to the group that received VR alone.
Due to the fact that achievement of independent community ambulation can provide opportunities to participate more easily in the home and community (Park et al. 2011); the stroke rehabilitation designed to improve walking function has focused on independence in community ambulation (Lord et al. 2004). In addition, the one of the most important factors for achieving community ambulation is the ability to manage a cognitive load while walking (Bowen et al. 2001). According to a previous study on dual task gait training of stroke patients, when a stroke patient walks while performing a cognitive task, they have a less stable gait pattern than when walking alone (Plummer et al. 2014). Since the traditional stroke rehabilitation is difficult to reflect the gait decrement while dual tasking (Cockburn et al. 2003); recent advances in stroke rehabilitation is designed to improve community ambulation and tend to emphasize the dual task gait assessment (Bowen et al. 2001; Yang et al. 2007b), and this phenomenon may reflect the broader dimensions of community ambulation (Yang et al. 2007b).
Of the theories explaining the gait decrement while dual tasking, two of the most influential classes of explanations are the bottleneck and capacity sharing models (Pashler 1994; Yang et al. 2007a). According to these two theoretical models, when multiple tasks are performed simultaneously, a central mechanism selects the appropriate additional resources to perform the tasks, and it changes continuously depending on the level of difficulty of the tasks. Gait decrement while dual tasking is caused by this central process, which may lead to a reduction of community ambulation or an increase of falling during daily living (Bowen et al. 2001; Plummer et al. 2014). Thus, through the mitigation of gait decrement while dual tasking, it may possible to improve stroke patients’ social participation and independent performance of activities of daily living. In addition, according to a previous study on the dual task effect of stroke patients (Bowen et al. 2001), higher level cognitive tasks including, memory, language processing, and attention, can increase the community interaction between the patient and the environment or situation.
In this study, through addition of the cognitive load task in the virtual reality training protocol, stroke patients were provided with the training environment and situations similar to real community activities. According to previous studies (Kizony et al. 2010; Cho and Lee 2013), realistic training method leads to the improvement on walking function in chronic stroke patients. Therefore, the findings of the present study indicate that VRTCL may be an effective method for facilitating independent community ambulation. We believe that this finding provides basic information for the development of rehabilitation programs for stroke patients.
In conclusion, the current study demonstrated a beneficial effect of VRTCL on walking function under single and dual task conditions in chronic stroke patients. However, this study had some limitations. First, the small sample size may have influenced the results for certain variables. Although the sample size was calculated using G*power software, it may not be enough to generalize of results of this study. Second, this study included only high functioning stroke patients; therefore, these results cannot be generalized to all stroke patients. Third, in spite of previous finding (the degree of dual task gait decrement can differ with the type of secondary cognitive task), this study could not determine whether the degree of dual task gait decrement varied according to the type of secondary cognitive task (Haggard et al. 2000; Al-Yahya et al. 2011). Thus, in the future, it will be investigated the effects of the type of secondary cognitive task on dual task gait decrement in stroke patients. Finally, since many previous studies demonstrated the effectiveness of real community ambulation training on walking function of stroke patients (Park et al. 2011; Kim et al. 2014); we think that the comparative studies on community ambulation training and virtual reality training for improvement of walking function of stroke patients are require.
This study was supported by a research grant from Sahmyook University in 2014.
The authors declare no conflict of interest.