Regular Contribution
Sedentary Behavior and Sleep Duration Are Associated with Both Stress Symptoms and Suicidal Thoughts in Korean Adults
2015 Volume 237 Issue 4 Pages 279-286
Details
2015 Volume 237 Issue 4 Pages 279-286
Prolonged sedentary time and sleep deprivation are associated with mental health problems such as depression and stress symptoms. Moreover, mental illness is linked with suicidal thoughts and suicide attempts. However, it is not clear whether sedentary time and sleep duration are associated with stress symptoms and suicidal thoughts independent of physical activity. Thus, our study aimed to identify if sedentary time and sleep duration were associated with both stress symptoms and suicidal thoughts. The participants in present cross-sectional study were 4,674 general Korean adults (1,938 male; 2,736 female), aged ≥ 20 years. Prolonged sedentary time (≥ 420 min/day) was significantly associated with the increased risk of stress symptoms (OR, 1.30; 95% CI, 1.04-1.62) compared with sedentary time of < 240 min/day. The OR for stress symptoms was significant for individuals who had ≤ 5 h/day of sleep time (OR, 1.88; 95% CI, 1.48-2.38) compared with sleep duration of ≥ 7 h/day. Moreover, prolonged sedentary time (OR, 1.55; 95% CI, 1.01-2.42 in ≥ 420 min/day vs. < 240 min/day) and short sleep duration (OR, 1.75; 95% CI, 1.17-2.62 in ≤ 5 h/day vs. ≥ 7 h/day) were significantly associated with an increased risk for suicidal thoughts after adjusting for confounding factors including physical activity. Thus, prolonged sedentary time and sleep deprivation are independently associated with both the risk of stress symptoms and suicidal thoughts. From a public health perspective, reducing sedentary time and improvement of sleep deprivation may serve as an effective strategy for preventing mental illness.
Mental illness is a significant contributor to the global burden of disease, and affects people in all communities across the world. The World Health Organization (WHO) reported that depression is estimated to affect 350 million people worldwide (World Health Organization 2012). The World Mental Health Survey conducted in 17 countries found that on average, one in 20 people reported having had an episode of depression (World Health Organization 2012). In South Korea, the suicide rate in 2013 was 28.5 per 100,000 population, an increase of 26.5% from the previous 10 years. This suicide rate is the highest among the Organization for Economic Cooperation and Development (OECD) countries (Statistics Korea 2013). In addition, a community-based study in Korea found that 53% to 74% of those who had attempted suicide had mental health problems (Jeon 2012). Therefore, identification of modifiable risk factors that may prevent development of mental health problems such as depression is particularly important (Teychenne et al. 2010b).
Recent mental health studies have shown that sedentary behavior is associated with metabolic syndrome, diabetes, and mortality independent of recommended physical activity levels (Ford and Caspersen 2012; Matthews et al. 2012; Kim et al. 2013). Several observational studies have also demonstrated an association between high levels of sedentary behavior and poor mental health (Teychenne et al. 2010a, b; Vallance et al. 2011). Teychenne et al. (2010b) reported that time spent in sedentary behavior was positively associated with onset of depression after adjusting for physical activity. Another meta-analysis reported similar findings on the independent effects of sedentary time and physical activity on mental health (Zhai et al. 2015). Therefore, sedentary behavior is now considered to be a distinct domain of behavior that may pose a risk to health in its own right.
The International Classification of Sleep Disorders (ICSD) defines individuals with a routine pattern of sleep duration of ≤ 5 h/day as short sleepers (Thorpy 2012). Short sleep is also recognized to have an adverse effect on hypertension, diabetes, and cardiovascular disease in addition to adverse effects on mental health, including stress, depression or suicide (Cappuccio et al. 2011; Kohyama 2011; Vgontzas et al. 2012; Gangwisch 2014; Shan et al. 2015). Moreover, a prospective cohort study showed that lack of physical activity was linked to worse mental health, with participation in physical activity reported to improve the symptoms of depression (Mammen and Faulkner 2013; Kuwahara et al. 2015). However, individuals who have prolonged sedentary time or short sleep may find it difficult to be sufficiently physically active. Therefore, the health effects of sedentary time, sleep duration, and physical activity depend on various factors in addition to the specific activity. However, as most studies have not considered the association of these three types of behavior (sedentary time, sleep duration, and physical activity) with mental health, independent associations of the three behavior patterns remain unclear. In Asia-Pacific populations, a high level of sedentary time is relatively rare compared with populations in Europe and North America (Bauman et al. 2011). Moreover, there is a lack of research examining the negative effects of prolonged sedentary time and short sleep on mental health in the Korean population. Therefore, the purpose of the present study was to determine the effects of sedentary time and sleep duration on mental health, based on self-reported stress symptoms and suicidal thoughts in the general South Korean population.
Data for this cross-sectional study were drawn from the Korean National Health and Nutritional Examination Survey (KNHANES) 2013. The KNHANES is a series of cross-sectional surveys with nationally representative samples from the civilian, non-institutionalized, South Korean population, using a stratified and multistage probability cluster design (Korea Centers for Disease Control and Prevention 2012; Kweon et al. 2014). We obtained complete health interviews, as well as health examination and nutrition survey data for 5,616 adults aged ≥ 20 years. We excluded 502 participants who had any limitation in daily life due to physical disability, along with 22 pregnant women. We also excluded 365 participants with missing mental health data; 4 with incomplete data on sedentary time, sleep duration, and physical activity; and 49 with missing data on confounding factors. In total, 4,674 participants (1,938 male and 2,736 female) were included. All participants provided written informed consent, and the KNHANES study was approved by the Institutional Review Board of the Korea Centers for Disease Control and Prevention (IRB 2013-07CON-03-4C).
Sedentary time, sleep duration, and physical activitySedentary time and physical activity were measured using the Korean version of the International Physical Activity Questionnaire Short Version (IPAQ-SV), capturing data from the 7 days before the investigation (Chun 2012). To calculate sedentary time, participants were asked “How much time do you spend sitting on a week day?” This question has been commonly used in previous studies (Bauman et al. 2011). This included time spent at work, at home, while doing course work, and during leisure time (e.g., time spent sitting at a desk, visiting friends, reading, or sitting or lying down to watch television). The reported levels of sedentary time were categorized as high, middle, and low based on overall population tertiles (low: < 240 min/day; middle: 240-419 min/day; and high: ≥ 420 min/day).
The IPAQ-SV records physical activity undertaken across a comprehensive set of domains including leisure time, and work- and transport-related activities. The activities assessed are walking, and moderate- and vigorous-intensity physical activity. Participants were asked to recall information about their physical activity type, frequency (days) and duration (h) of various activities for the 7 days before the investigation. We divided participants into three total physical activity groups, calculated by summing the reported time spent walking and in moderate-vigorous physical activity (0 min/week, < 150 min/week or ≥ 150 min/week) based on achievement of the WHO-recommended physical activity levels.
Sleep duration was measured using a self-report questionnaire. Participants were asked “How much time do you sleep on a week day? We classified participants into three groups based on reported sleep time: ≤ 5 h/day, 6 h/day, or ≥ 7 h/day. Short sleep duration was defined as ≤ 5 h/day based on the ICSD definition of sleep duration (Thorpy 2012).
Stress symptoms and suicidal thoughtsStress symptoms and suicidal thoughts were assessed with a simple self-report questionnaire administered at a mobile examination center (Kweon et al. 2014). Participants answered the question “Have you felt sad or desperate for more than 2 weeks during the past 1 year, so much that it disturbed your daily life?” We defined participants who answered “Yes” to this question as having stress symptoms. Suicidal thoughts were assessed with the question: “Did you think about committing suicide in the last 12 months?” Participants who answered “Yes” were defined as having had suicidal thoughts.
CovariatesPotential confounding factors included age, sex, body mass index (BMI), education level, household income, occupation status, smoking status, alcohol intake, and number of chronic diseases, were measured using a general health questionnaire. Household income was classified by quartile of the overall population. We reclassified education level as “less than high school”, “high school” or “more than high school”, and alcohol consumption as “never”, “≤ once/week”, “2-3 times/week”, or “≥ 4 times/week”. Smoking status was classified as “nonsmoker”, “former smoker” or “current smoker”. BMI was calculated from body weight and height (kg/m2), and was classified as normal weight (< 25 kg/m2) or obese (≥ 25 kg/m2) according to the Korean Society for the Study of Obesity recommendations.
Statistical analysisAll data were analyzed using SPSS Complex Samples procedures to account for the complex survey design with stratified and cluster sampling (PASW Statistics 18 for Windows, IBM Inc, Chicago, IL, USA). Values were expressed as weighted means ± standard error (SE) or weighted percentages. P < 0.05 was considered statistically significant. Statistical significance according to levels of sedentary time, sleep duration, and physical activity were evaluated using chi-square tests. Logistic regression models were used to predict the risk of stress symptoms and suicidal thoughts from the levels of sedentary time, sleep duration, and physical activity, after adjusting for age, sex, education level, household income, occupation status, living status, marital status, number of diseases, smoking status, and alcohol consumption. To examine the independent effects of sedentary time, sleep duration, and physical activity on stress symptoms and suicidal thoughts, we included the categorical variables of sedentary time, sleep duration, and physical activity into a single model.
The participants’ demographic characteristics are presented in Table 1. Participants were 4,674 Korean adults aged ≥ 20 years. Of the participants, 51.4% were female, 19.1% were aged ≥ 60 years, and 12.5% had two or more chronic diseases. Table 2 presents the participants’ sedentary time, sleep duration, and physical activity. The weighted means were 356.7 min/day for sedentary time, 6.7 h/day for sleep duration, and 482.5 min/week for physical activity.
Table 3 sets out the frequency of stress symptoms and suicidal thoughts associated with levels of sedentary time, sleep duration, and physical activity. Overall, 24.1% of the participants had felt stress (23.0% of male, and 25.1% of female). Additionally, 4.1% of participants reported having had suicidal thoughts (2.8% of male and 5.4% of female). The prevalence of suicidal thoughts was significantly higher in female compared with male (P < 0.001), but not stress symptoms (P = 0.134) (Table 3). Sedentary time was significantly and positively associated with the frequency of stress symptoms (P = 0.001), but not suicidal thoughts (P = 0.484). Table 3 also shows that sleep duration was significantly and negatively associated with the frequency of stress symptoms (P < 0.001) and suicidal thoughts (P < 0.001). Moreover, the frequency of suicidal thoughts was significantly different for the different levels of physical activity (Table 3).
The results of the logistic regression analyses comparing the odds ratio (OR) for stress symptoms and suicidal thoughts across the tertiles of sedentary time, sleep duration, and physical activity are shown in Table 4. The OR for stress symptoms in the high and middle tertiles of sedentary time were 1.30 (95% confidence interval [CI] 1.04-1.62) and 0.99 (95% CI: 0.81-1.20) compared with the low tertile after adjusting for age, sex, education level, household income, occupation status, family number, marital status, number of diseases, smoking status, alcohol consumption, sleep duration, and physical activity (Table 4). We also examined the association between sedentary time and the OR for suicidal thoughts in the past 1 year. Sedentary time was significantly associated with an increased risk for having had suicidal thoughts: for the middle tertile of sedentary time, the OR for suicidal thoughts was 1.25 (95% CI: 0.82-1.91) and 1.55 (95% CI: 1.01-2.42) for the high tertile of sedentary time.
Significantly higher ORs for stress symptoms were found in participants who reported sleep duration of ≤ 5 h/day (OR: 1.88, 95% CI: 1.48-2.38) and 6 h/day (OR: 1.36, 95% CI: 1.14-1.63) compared with those in the longer sleep duration group (≥ 7 h/day) (Table 4). We also found a higher risk for suicidal thoughts in participants who had sleep duration of ≤ 5 h/day (OR: 1.75, 95% CI: 1.17-2.62) and 6 h/day (OR: 1.49, 95% CI: 1.06-2.11) compared with those with a longer sleep duration. The OR for stress symptoms and suicidal thoughts in participants who reported never engaging in physical activity were 1.29 (95% CI: 1.02-1.66) and 1.41 (95% CI: 0.90-2.20) compared with participants who reported the recommended level of physical activity (Table 4).
To examine sex- or age-based interactions in the associations between sedentary time, sleep duration, and physical activity, and stress symptoms and suicidal thoughts, we used a subgroup analysis separated by sex and age groups (Tables 5, 6). The interaction term between sedentary time and sex was statistically significant for stress symptoms in male (P = 0.009) (Table 5). We also found a significant interaction between sleep duration and age for stress symptoms; with the effect size larger in participants aged 20-39 years. In addition, a significant interaction by age was found in the association between sedentary time and the risk of suicidal thoughts (P = 0.041, Table 6).

Participant characteristics (n = 4,674).
Values were weighted percentages (SE, standard error).
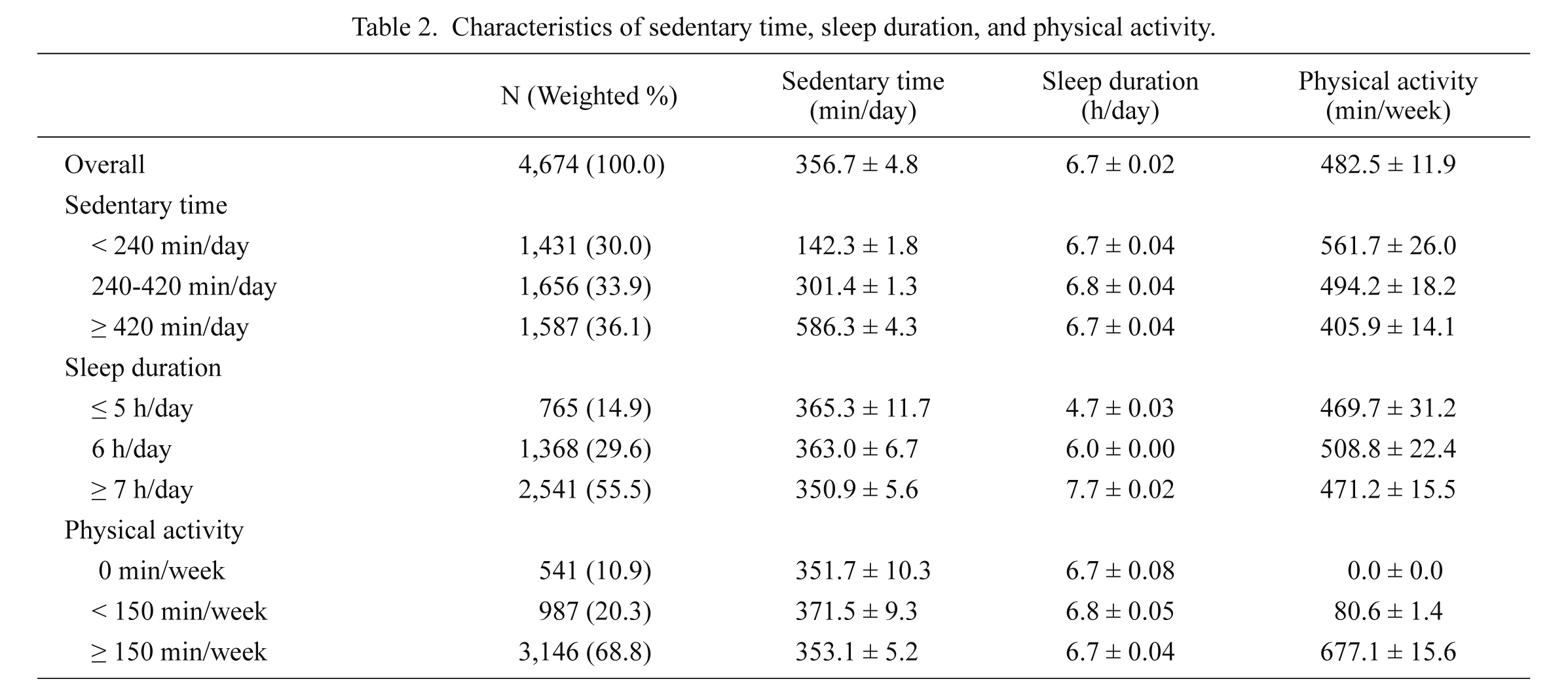
Characteristics of sedentary time, sleep duration, and physical activity.
Values were weighted mean (SE, standard error).
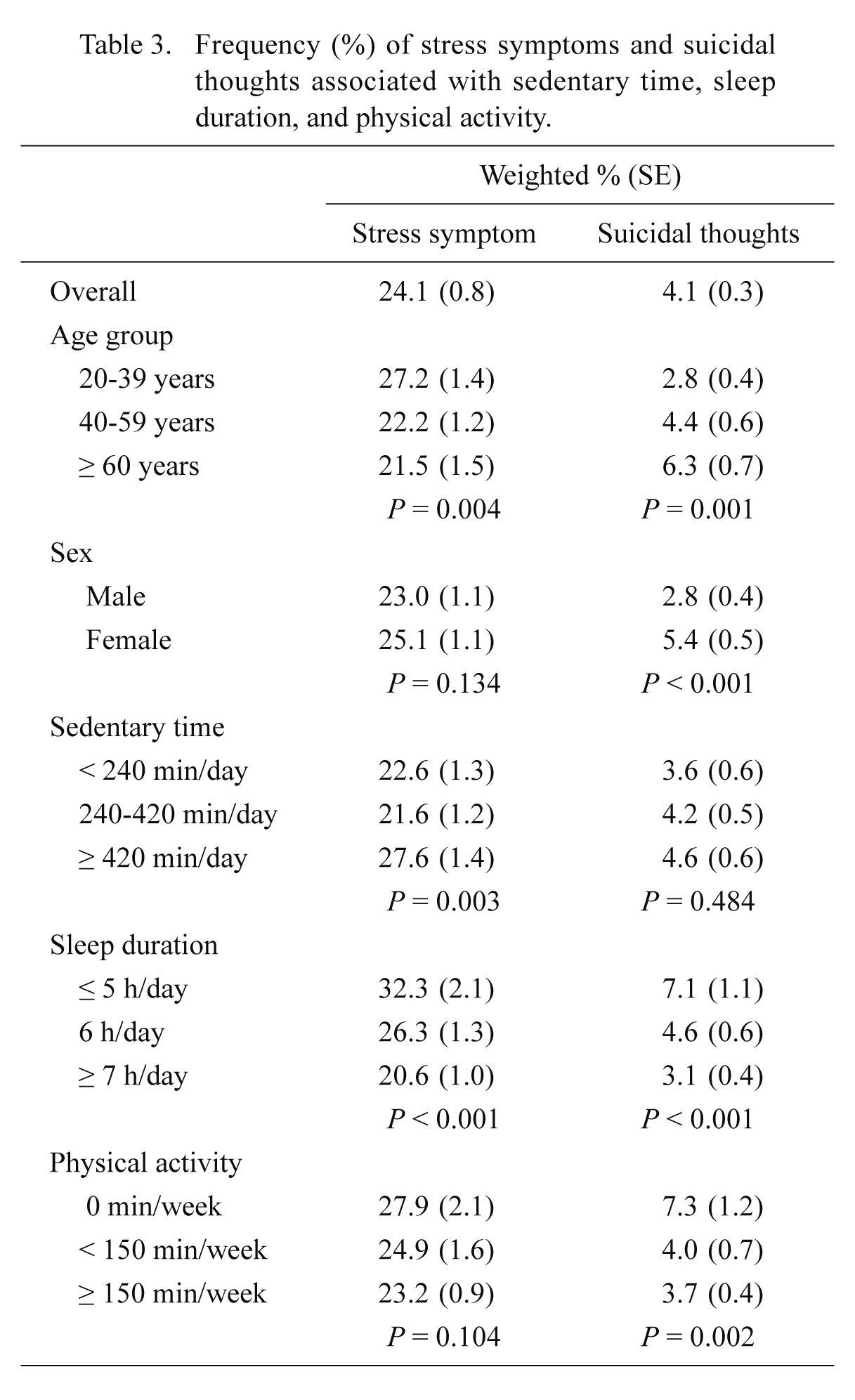
Frequency (%) of stress symptoms and suicidal thoughts associated with sedentary time, sleep duration, and physical activity.
P-values calculated using chi-square tests.
SE, standard error.

Odds ratios for stress symptoms and suicidal thoughts by sedentary time, sleep duration, and physical activity in South Korean adults (n = 4,647).
Values were odds ratio (95% confidence intervals [CI]), *P < 0.05.
Adjusted for age, sex, education level, household income, occupation status, living status, marital status, number of diseases, smoking status, alcohol consumption, sedentary time, sleep duration, and physical activity.
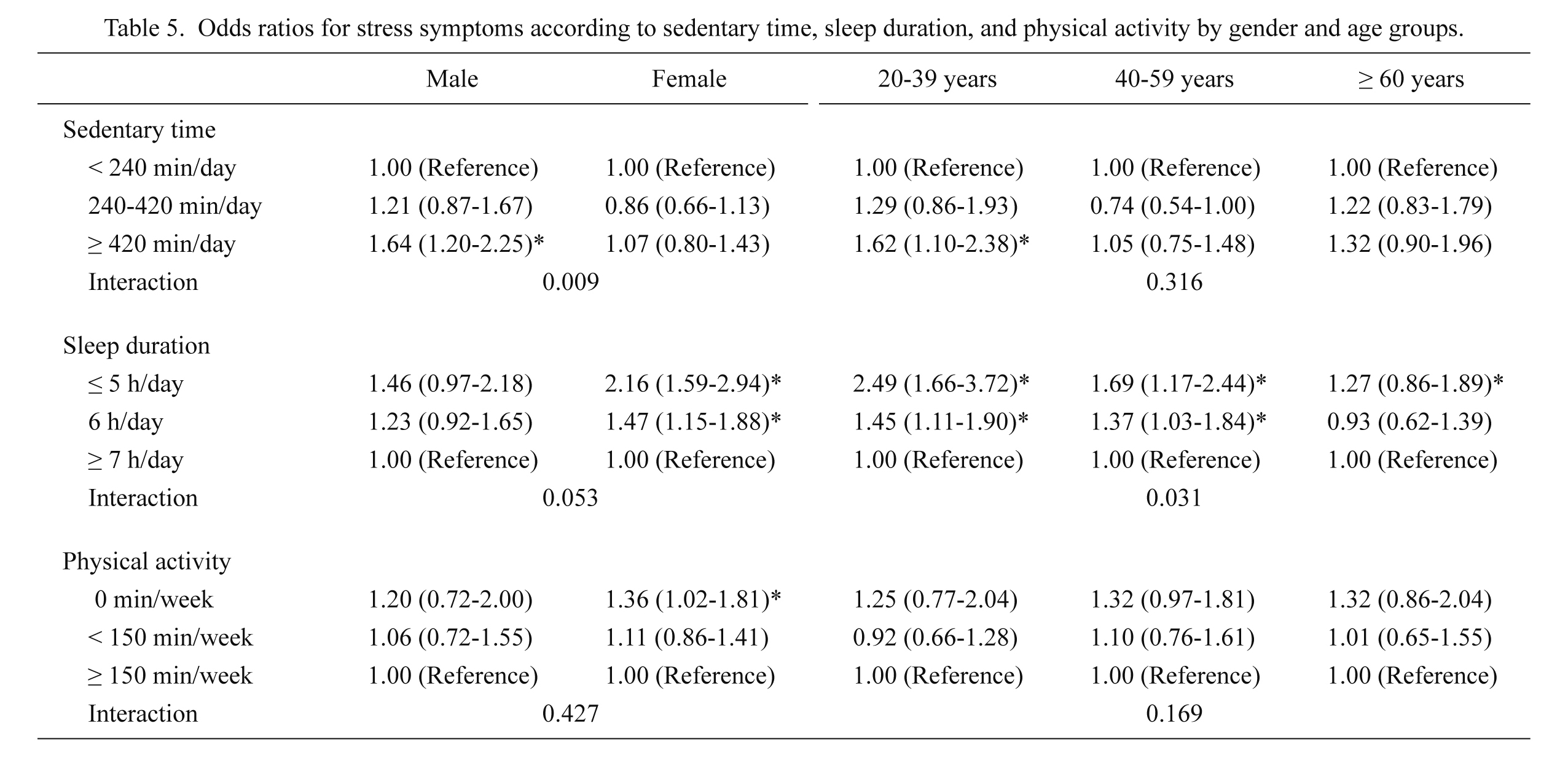
Odds ratios for stress symptoms according to sedentary time, sleep duration, and physical activity by gender and age groups.
Values were odds ratio (95% confidence intervals [CI]), *P < 0.05; adjusted for age, sex, education level, household income, occupation status, living status, marital status, number of diseases, smoking status, and alcohol consumption.

Odds ratios for suicidal thoughts according to sedentary time, sleep duration, and physical activity by gender and age groups.
Values were odds ratio (95% confidence intervals [CI]), *P < 0.05; adjusted for age, sex, education level, household income, occupation status, living status, marital status, number of diseases, smoking status, and alcohol consumption.
We investigated the associations between three types of behavior (sedentary time, sleep duration, and physical activity) and mental health in the general South Korean population, using a large, population-based cross-sectional study. We found that higher levels of sedentary time and short sleep duration were independently significantly associated with an increased risk of stress symptoms and suicidal thoughts. Moreover, we found significant interaction effects of sedentary time and sex, and sleep duration and age on the risk of stress symptoms; sedentary time was significantly associated with stress symptoms in male, and sleep duration showed a stronger association in younger participants (the group aged 20-39 years) compared with older participants.
Our investigation of the impact of sedentary time on the prevalence of stress symptoms and suicidal thoughts found that the prevalence of stress symptoms and suicidal thoughts were approximately 1.3 times and 1.6 times higher in the high sedentary time tertile compared with the low sedentary time tertile. Our results are consistent with those of previous studies that found an objectively measured total sedentary time, and screen-based sedentary time (TV viewing or internet use) was associated with the risk of depression symptoms (Kendall-Tackett et al. 2011; Brunet et al. 2014; Hamer and Stamatakis 2014; Teychenne et al. 2014). For example, a review of previous studies described sedentary time (e.g., TV viewing, internet use, or overall sedentary time) was positively associated with mental health problems such as stress and depression (Teychenne et al. 2010b). Moreover, screen-based sedentary time was associated with the increased risk of a mental disorder in longitudinal study (Sanchez-Villegas et al. 2008). However, there is a lack of information about the association between sedentary time and suicidal thoughts. To our knowledge, there have been no studies that have examined the association between sedentary time and suicidal ideation; therefore, our study is the first to examine these associations.
There are several factors that may explain this association between sedentary time and mental health. First, many studies have reported that sedentary time was associated with cardiometabolic risk factors (Cappuccio et al. 2011; Zhai et al. 2015). In addition, colonic disease was associated with poor mental health (Cole and Dendukuri 2003). Therefore, the links with mental health might partly act through these mechanisms. Second, social and psychosocial mechanisms might also be important (Cole and Dendukuri 2003); for example, increased sedentary time may encourage social isolation, limit the development of social networks, and remove individuals from social interactions and as a result, increase their risk of mental health problems.
Our results also showed that sleep deprivation was significantly associated with a 1.9-fold higher risk of stress symptoms, and a 1.8-fold higher risk of suicidal thoughts. Prolonged, excessive stress or depression are linked with thinking about suicide and attempted suicide (Goldman-Mellor et al. 2014); and most suicide attempts are by those who have previously thought of suicide (Bronisch and Wittchen 1994). For example, a 14-year follow-up study reported that stress and suicidal ideation were associated with action of suicidal thoughts (Fujino et al. 2005). Short sleep duration may affect both psychological and physiological health conditions, with negative effects on judgment, fatigue, stress, and impulse control. Moreover, a review of recent studies on sleep and suicidal ideation found clear evidence that short sleep duration was associated with serotonin levels, and may be linked to suicide, although the direction of causation required clarification (Kohyama 2011). Some studies have also reported that mental health problems might contribute to short sleep duration or poor sleep quality. Thus, these two factors affect each other, suggesting a possible vicious cycle.
In the present study, we found a significant association between physical activity and stress symptoms, a result consistent with a recent systematic review of prospective studies (Mammen and Faulkner 2013). Many studies examining independent associations between sedentary time or sleep duration and mental health have considered physical activity as a confounding factor. However, no previous studies have considered the effects of three types of behavior (sedentary time, sleep duration, and physical activity) on mental health. Our results suggest that sedentary time and sleep duration are directly and independently associated with mental health.
In the present study, we also determined interaction terms in the associations between sedentary time, sleep duration, and physical activity, and the risk of stress symptoms and suicidal thoughts by sex and age. We found that sedentary time was associated with stress symptoms only in male. Moreover, the association between sleep duration and stress symptoms was more clear and stronger in younger participants aged 20-39 years. In this respect, our results were inconsistent with the results of a previous study that found no significant interaction between sedentary time and sex or age on the risk for depression in general US adults (Vallance et al. 2011). However, Teychenne et al. (2014) reported that greater amounts of TV viewing predicted the risk of depression, although sedentary behavior might not predict subsequent depressive symptoms. In addition, similar to the results of previous studies, our findings showed that the prevalence of stress symptoms was higher among younger participants. Thus, these sex and age differences, and differences in the types and pattern of activities and lifestyles including sedentary behavior; particularly, the sex and age differences in occupation-related sedentary time, are considerable. However, as in the present study we only evaluated total sedentary time, we could not analyze the effect by the domain of sedentary time. Further research investigating the effect of sex- and age-based sedentary time differences on stress symptoms is needed.
The present study has several limitations that should be considered. A major limitation was that we could not infer causality or specify the direction of the effect because of the cross-sectional survey design. As mental health is a relevant factor in sleep disorders, it may also act as a cause of increased sedentary time. Second, we could not rule out recall-bias for self-reported sedentary time, sleep duration and physical activity, although the reliability and criterion validity have previously been reported (Oh et al. 2007). Moreover, because we measured total sedentary time and sleep duration, we could not show the effects of the sedentary domain and sleep quality on mental health. In addition, the presence of a sleep disorder or drug therapy due to a sleep-related disorder may have acted as a bias in the measurement of total sleep time in our study. An important strength of the present study is that the KNHANES data were nationally representative, multistage probability samples of South Korean adults (Kweon et al. 2014). Therefore, it is possible that our findings may be generalized to the South Korean population. Our findings are also important from a public health perspective, particularly in terms of designing interventions aimed at promoting mental health by focusing on preventing suicidal thoughts in the wider Korean population.
In conclusion, we found that prolonged sedentary time and sleep deprivation are associated with both the risk of stress symptoms and suicidal thoughts. Moreover, in these associations, we observed significant interaction terms, with more clear associations between sedentary time in male and sleep duration in younger adults. Further investigating the nature of the associations between sedentary behavior, sleep duration, stress symptoms, and suicidal thoughts should be a consideration for future intervention studies.
The present study was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF), funded by the Korea Ministry of Education (2014R1A1A2059106).
The authors declare no conflict of interest.