Abstract
Atrial fibrillation (AF) is currently recognized as one of the most common cardiac arrhythmias worldwide, with the increasing prevalence that has been estimated to be as high as 9% among the elderly. Health-related quality of life (HRQoL) has become an important patient-centered health outcome measurement, but the impacts created by AF and other arrhythmias with similar symptoms, such as frequent atrial and ventricular premature contractions (APCs and VPCs, defined as ≥ 3 beats/5 minutes), have not been extensively evaluated. The Yilan Study is a population-based community health survey, which in part aims to evaluate the prevalence and impacts of these arrhythmias on the HRQoL in a community dwelling elderly population. A total of 1,732 citizens from the Yilan, Taiwan, aged 65 years or older (45.8% male) were enrolled and visited at their homes, where HRQoL was measured utilizing the Short Form-12 Health Survey. Each participant’s heart rhythm was recorded with an electrocardiographic monitor for 5 minutes. The results disclosed that the prevalence of AF of this aged population was 5.8%, similar to the mean global prevalence. Besides, the prevalence of frequent APCs and frequent VPCs in these elderly people were 7.1% and 5.5%, respectively. After multiple regression analysis, elderly people with AF had lower scores in the physical component of HRQoL, while those elderly people with frequent VPCs had lower scores in the mental component. Ultimately, these findings can provide additional useful and population-specific information about AF, and assist medical professionals in designing more effective strategies for cardiac arrhythmia treatments.
Introduction
Atrial fibrillation (AF) is currently recognized as one of the most common cardiac arrhythmias with clinical significance (Go et al. 2001; Chen and Shen 2007; Chugh et al. 2014). The prevalence of this widespread affliction has been estimated to range from 0.95 to 2.13% (Go et al. 2001; Chen and Shen 2007; Wilke et al. 2013). There are several proposed factors which may influence the prevalence of AF. From earlier studies, such as the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) study, AF occurred more frequently in elderly people, and its prevalence could be up to 9.0% in people 80 years of age or older (Go et al. 2001; Chen and Shen 2007). Male subjects have also been found to be more susceptible to such disease. In a systemic review of Chugh et al. (2014), the age-adjusted prevalence of AF in 2010 might be 596.2 per 100,000 males, as compared to 373.1 in females. Regional differences have also been proposed to influence the occurrence of AF, comparable with the greater disease burden observed in developed countries and a lower burden in the Asian region (Chugh et al. 2014). In Taiwan, Chien et al. (2010) conducted a community-based prospective study and found that the prevalence of AF was 1.07%, and about 2-3% in people 65 years of age or older. However, there are still relatively few studies of AF prevalence to date obtaining their data through a community-based survey. For example, Wilke et al. (2013) have reviewed 16 studies of AF prevalence and found only 3 of these studies were population-based surveys. Iguchi et al. (2008) and Inoue et al. (2009) also conducted their studies based on the periodic health examinations in Japan.
There is a growing interest in the impact of AF on the health-related quality of life (HRQoL), which has been considered as an important patient-centered health outcome measurement (Mohanty et al. 2014). However, the results of previous studies have been conflicting. Some studies reported impaired HRQoL in patients with AF (Dorian et al. 2000; Paquette et al. 2000; van den Berg et al. 2001; Kang and Bahler 2004; Thrall et al. 2006), while others reported no significant differences of HRQoL between AF patients and the control population (Howes et al. 2001; Ariansen et al. 2011; Roalfe et al. 2012). There were also studies with results suggesting that the HRQoL in AF patients might initially decrease, but improve progressively in the next few months or years (Jenkins et al. 2005; Reynolds et al. 2006). Mohanty et al. (2014) has also found that even in patients with asymptomatic longstanding persistent AF, successful ablation could still improve HRQoL. Several types of weakness in methodology have been proposed as contributors to such conflicting results (Thrall et al. 2006; Aliot et al. 2014). Besides, other common cardiac arrhythmias, such as frequent atrial premature contractions (APCs) and frequent ventricular premature contractions (VPCs), may also induce similar bothersome symptoms as those of AF. But there are also relatively few studies regarding the impacts of these ectopic beats on the HRQoL to date (Huang et al. 2006).
In this study, we aimed to investigate the prevalence of AF and other cardiac arrhythmias with similar symptoms, such as frequent APCs and frequent VPCs, in an elderly population through the use of a community survey. We also compared the impacts of these cardiac arrhythmias on the HRQoL of these patients with those exerted by sinus rhythm in an elderly population living in the same community.
Methods
This study is part of the Yilan Study, which is a population-based community health survey conducted by the Community Medicine Research Center at the National Yang-Ming University and the National Yang-Ming University Hospital in Taiwan. The methods of this study have been described elsewhere (Hsu et al. 2014). In brief, with the assistance of the Community Angels (social volunteers) and the Yang-Ming Crusade (student volunteers of the National Yang-Ming University), all people at least 65 years of age living in the 7 most populated villages of Yilan City, a city located in the northeastern part of Taiwan, were visited at their homes by well-trained project assistants. Thereafter, information regarding basic demographic characteristics, life style, and history of chronic diseases was obtained from the target population. Additionally, measurement of anxiety, depression and the HRQoL was also performed through face-to-face interviews. If some of the survey items could not be completed, such as if some participants could not be weighed due to bed-ridden status, or some could not complete the questionnaires or define their life styles or disease status accurately, the result would be recorded as “missing”. All participants provided written informed consent, and the study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki. The Institutional Review Board of the National Yang-Ming University Hospital has also approved this study with human subjects (IRB No. 2011A016).
Evaluation of the anxiety and depression status
The Hospital Anxiety and Depression Scale (HADS) was used to measure the anxiety and depression status of the subject population. Given its longstanding use in the medical community, the HADS has been deemed a reliable method for measuring both clinical and subclinical anxiety and depression symptoms in the general population (Zigmond and Snaith 1983; Bjelland et al. 2002). The HADS scale is composed of 14 items designed to ascertain the participant’s feelings in the past one week, with 7 items rating anxiety and 7 rating depression. Each item is scored on a scale from 0 to 3, and higher scores indicate an elevated anxious and depressive tendency. The Chinese translation of the HADS has been proven valid, with the optimal cut-off points of 3 for the anxiety, and 6 for the depression subscores, respectively (Lam et al. 1995).
Evaluation of HRQoL
Our study utilized the Short Form 12 Health Survey Version 2 (SF-12v2) to evaluate the HRQoL of study participants. Twelve items derived from the Short Form 36 Health Survey Version 2 (SF-36v2) are used to constitute the mental component summary (MCS) and physical component summary (PCS) for measuring the participant’s mental and physical function status in the prior four weeks (Maruish 2009). A higher score represents better status of HRQoL. The translation of the SF-36 and SF-12 from English to Chinese has been carefully developed, and ultimately proven valid (Tseng et al. 2003).
Recording of cardiac electrical activity
Each participant was asked to rest for 5 minutes in a sitting position, and subsequently his or her cardiac electrical activity was recorded by a lead-I electrocardiogram (ECG) for 5 minutes. The signals were acquired, stored, and processed by a real-time, long-term heart rate variability analyzer (KY-3, Yang-Ying Inc., Taiwan), using a 10-bit analog-to-digital converter with a sampling rate of 512 Hz (Kuo et al. 1999; Chen et al. 2010, 2012). All electrocardiographic interpretations were personally checked by two of the lead doctors in this study. If AF rhythms were detected during the 5-minute duration of patient monitoring, either entirely or intermittently, then those patients were characterized as suffering from AF. Those subjects with intermittent episodes of fibrillation rhythm were also defined as patients with paroxysmal AF. In earlier studies, Myerburg et al. (1984) and Shinohara et al. (1999) defined frequent APC and VPC as over 30 beats/hour. Therefore, we postulated that people with 3 or more beats during the 5-minute monitoring period of either APC or VPC should experience a similar quality of life as those with frequent premature contractions. We then defined these people as having frequent APCs or frequent VPCs.
We used the IBM SPSS Statistics version 21 to analyze all data. In the univariate analysis, the Chi-square test was used to compare different demographic, life style, and comorbidity variables between people with and without various cardiac arrhythmias. The independent t-test was also utilized to compare the MCS and PCS in these populations. Those variables found to be significantly associated with HRQoL according to our previous work and by univariate analysis were included in the multiple regression analysis (Hsu et al. 2014). Subsequently, for statistical efficiency, we used the stepwise multiple regression method to analyze the relationships between HRQoL (MCS and PCS) and the factors of demographic characteristics, life style and various arrhythmias in order to ascertain those variables that played major roles in the association. We also calculated the R squares using both the Stepwise method and the Enter method for further comparison. The dichotomous values of the HADS were used for univariate analysis, with the raw scores applied to multivariate analysis. All reported P values are two-tailed and considered significant if P ≤ 0.05.
Results
There was a total of 1,732 elderly citizens, aged 65 years and above, that participated in this study. Their mean age was 74.9 years, with a standard deviation (SD) of 6.9 years, and 793 of them were male (45.8%). The demographic characteristics, including age and sex, were similar to those of the elderly population living in this city. There were 100 patients that were identified as suffering from AF, with a mean age of 78.7 years (SD: 7.7 years). Among these patients, twenty-nine suffered from paroxysmal AF. The estimated AF prevalence was 5.8%. It was also noted that AF prevalence was elevated in males and increased with advancing age. There were 123 participants found to have frequent APCs (7.1%), and 95 had frequent VPCs (5.5%). The prevalence of these two cardiac arrhythmias also increased with advancing patient age and appeared to be higher in males. Other than age and gender, only cardiovascular disease and stroke occurred more frequently in AF patients. In patients with frequent VPCs, hypertension, gout and cardiovascular disease occurred more commonly. However, except for age, there were no signifiant differences of all other variables between participants with and without frequent APCs (Tables 1 and 2).
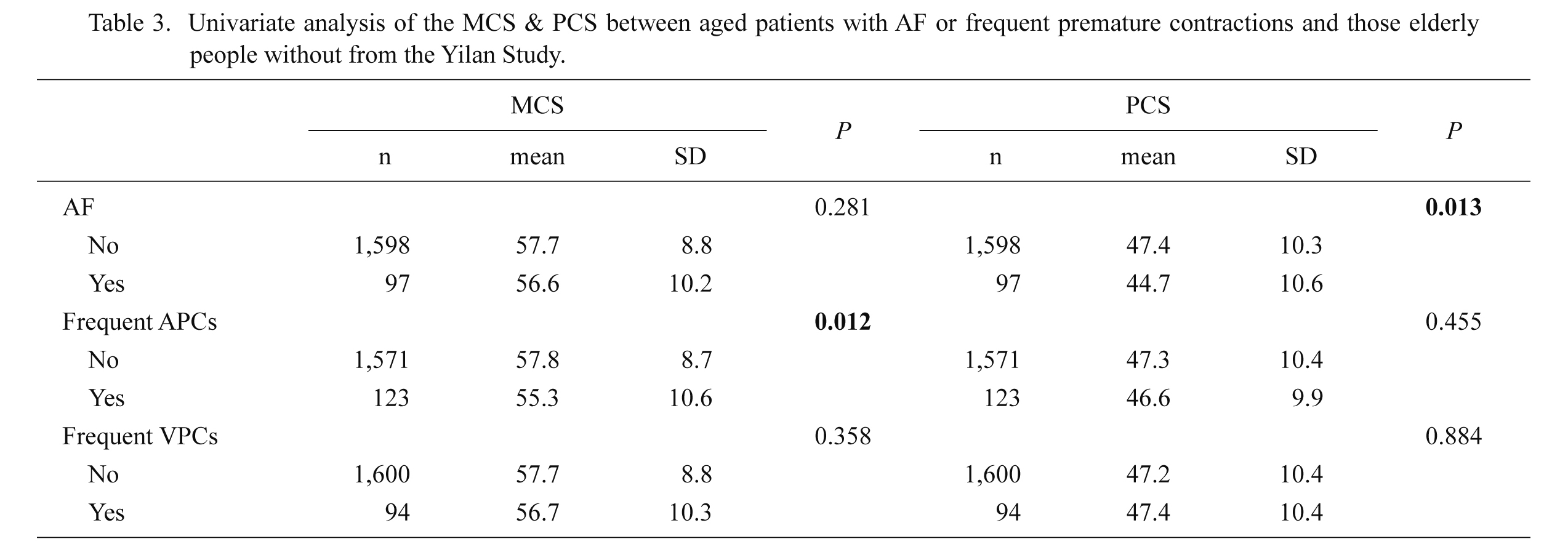
As compared to a population without these arrhythmias by univariate analysis, the scores of the MCS seemed to be lower in patients with frequent APCs, while no significant differences were found in patients with the other 2 kinds of cardiac arrhythmias. Interestingly, the scores of the PCS were found to be lower in AF patients, while no significant changes were found in patients with frequent APCs or VPCs, as compared to those study subjects without such arrhythmias (Table 3).
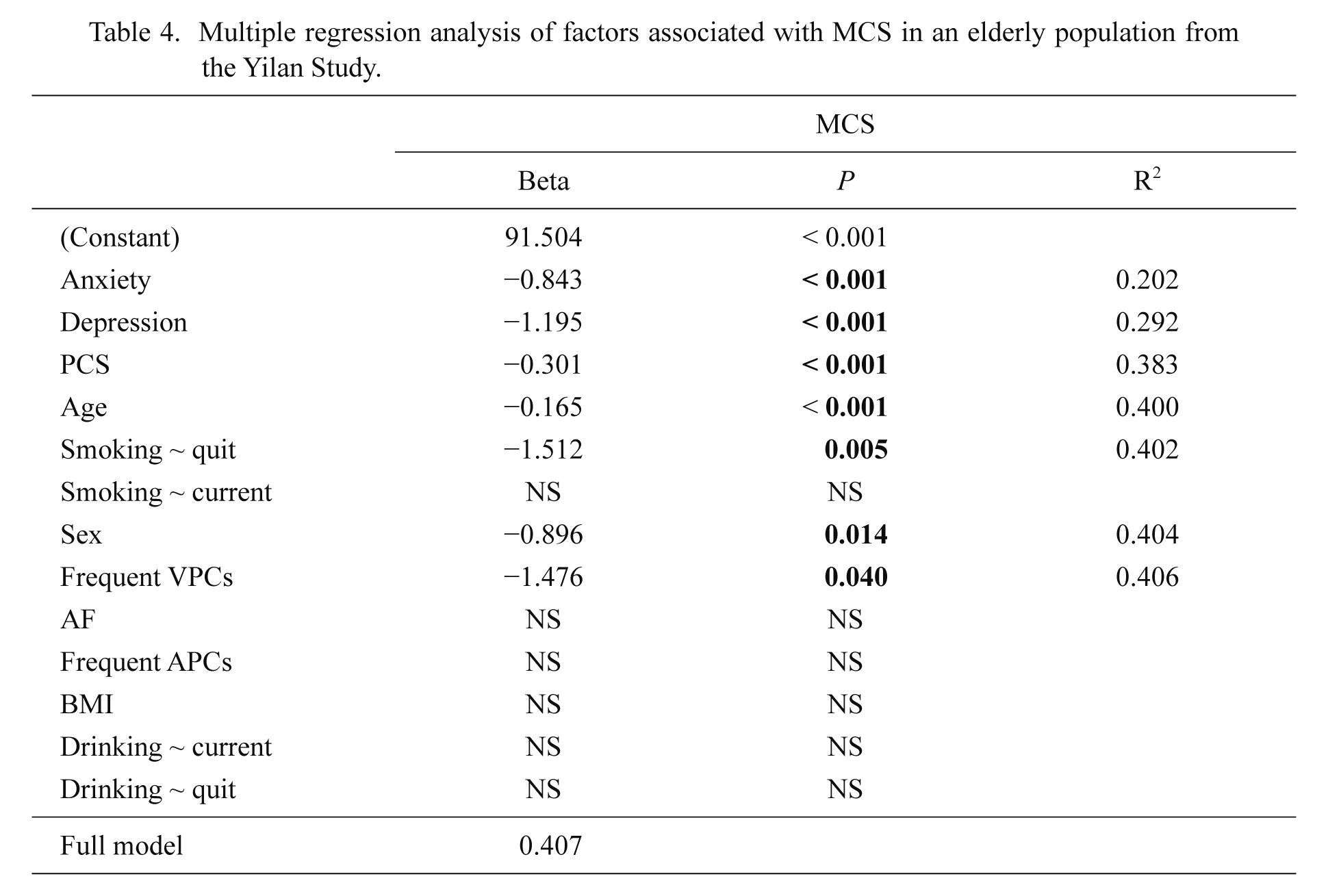
However, after controlling for those demographic characteristics, mental status (anxiety or depression), and life style, the study results disclosed that those patients with frequent VPCs, rather than with frequent APCs, had significantly lower scores of MCS of HRQoL as compared to those without. Regarding the PCS of HRQoL, the AF patients still had significant and lower scores as compared to those participants without AF (Tables 4 and 5).
Discussion
Our study results revealed that the prevalence of AF in an elderly Taiwanese population (≥ 65 years) was 5.8%. This was higher than that found in the study of Chien et al. (2010) in Chin-Shan, another city in Taiwan, but consistent with the results from the ATRIA study (with an AF prevalence of 6.1% in people 65 years or older in North America) (Go et al. 2001). As shown in Table 6, our study results suggest that the prevalence of AF in an elderly population living in Taiwan is not only higher than the estimated prevalence in the Asia-Pacific region, but also no less than the estimated global prevalence, even approaching that found in the North America region (Go et al. 2001; Chugh et al. 2014).
Why Taiwan may have the higher prevalence of AF?
Several reasons may explain such differences. First, we recorded participants’ cardiac electrical activity for 5 minutes, which was longer than those studies using the standard 12-lead surface ECG measurements for 20 seconds. When this process was utilized, more cases with paroxysmal AF might be detected (Yap et al. 2008; Chien et al. 2010). Second, because a significant proportion of AF attacks were asymptomatic, there would inevitably be a segment of AF patients not visiting clinics for medical assistance (Defaye et al. 1998; Strickberger et al. 2005; Yamamoto et al. 2014). Therefore, this might cause some studies relying on medical records or claims to underestimate the AF patient population (Go et al. 2001; Piccini et al. 2012). On the contrary, we made an effort to visit people living at home, which could in fact reduce such possible bias. In fact, several recent study results also found or estimated the increasing global AF prevalence (Ohlmeier et al. 2013; Wilke et al. 2013; Chugh et al. 2014; Schnabel et al. 2015). After prolonged observation of the Framingham cohort, Schnabel et al. (2015) suggested that the 400% rise of AF prevalence in this population might be attributable to enhanced surveillance methods and longer survival duration due to improved treatment of AF and its risk factors. This conclusion may also partly explain our study findings. Therefore, in conducting this community survey, we have provided evidences that the prevalence of AF in Taiwan may be no less than the prevalence in other parts of the world, which is different from the results of previous studies before (Lee et al. 2007; Chien et al. 2010).
A decrease in the physical but not mental component of HRQoL in AF patients
Our study results also suggest that the physical component of HRQoL is decreased in AF patients, while the mental component is not. These findings are compatible with those in Ariansen’s study (Ariansen et al. 2011). Besides, most other studies also disclosed an impaired physical part of HRQoL (Dorian et al. 2000; Paquette et al. 2000; van den Berg et al. 2001; Kang and Bahler 2004; Jenkins et al. 2005). Stewart et al. (1989) and Alonso et al. (2004) have pointed out that chronic medical conditions which were more symptomatic and disabling, such as congestive heart failure and myocardial infarction, had the lowest PCS score. Furthermore, the Framingham Heart Study also suggested that cardiovascular disease might be a risk factor predisposing a person to AF (Stewart et al. 1989; Benjamin et al. 1994; Alonso et al. 2004). We also believe that the bothersome symptoms associated with AF, such as palpitation, dizziness and dyspnea, may also restrict the daily activities of these patients and thus decrease PCS. Besides, the average age of the AF patients in our study was older than the ordinary population (78.7 ± 7.7 vs. 74.6 ± 6.7, p < 0.001), and Singer et al. (1999) demonstrated that physical functioning would decline with advancing age. Therefore, even after controlling for psychological status (such as depression, which played a major role in the association with PCS shown in Table 5), AF is still found to have a reverse association with PCS.
Why our results differ from other studies?
However, the results of our study which suggest that MCS may not be affected by AF is not compatible with the results of several other studies (Dorian et al. 2000; Paquette et al. 2000; van den Berg et al. 2001; Kang and Bahler 2004; Jenkins et al. 2005; Reynolds et al. 2006). There are several explanations for such differences. First, the target AF populations of most prior studies were selected from patients joining large clinical trials, being newly diagnosed, or visiting clinics for assistance (Dorian et al. 2000; Paquette et al. 2000; van den Berg et al. 2001; Kang and Bahler 2004; Jenkins et al. 2005; Reynolds et al. 2006; Roalfe et al. 2012). It would be reasonable to estimate that these patients might be more anxious or depressed, which has been proven to be reversely associated with MCS (Creed et al. 2002; Lim et al. 2012). Second, most of the previous trials did not control the psychological status during the analysis. Considering the suggestion of Thrall et al. (2006) that a third of AF patients might have elevated levels of anxiety or depression, these study results could be affected by the comorbid mental disorders. Third, as we earlier mentioned, all of our AF patients were relatively elderly and invited from the surrounding community. Therefore, a process of psychological adjustment or adaptation to AF might play a role in stabilizing the patient’s mental status while accommodating the frequently encumbered physical status of this part of the population, as proposed by Singer et al. (1999). Furthermore, both the Fibrillation Registry Assessing Costs, Therapies, Adverse events and Lifestyle study (FRACTAL) and the Atrial Fibrillation Follow-up Investigation of Rhythm Management study (AFFIRM) disclosed that the HRQoL of the AF patients impaired at the beginning of the study, and recovered progressively in the next six months to one year. This finding might also provide evidence of psychological adjustment or adaptation to AF (Jenkins et al. 2005; Reynolds et al. 2006). Finally, frequent premature contractions, originating from either the atrium or the ventricle, are common and may also have impacts on the mental part of the HRQoL, as shown in our study (Huang et al. 2006).
Frequent VPCs, but not APCs, are reversely associated with mental part of HRQoL
Our study results disclosed that patients with frequent VPCs had lower scores of MCS as compared to those without. This finding may further suggest that frequent VPCs, rather than frequent APCs or AF, are significantly and reversely associated with the mental part of HRQoL after controlling for demographic characteristics, life style, psychological status and the physical part of quality of life. Huang et al. (2006) proposed that patient’s HRQoL could improve after eliminating the frequent VPCs by radiofrequency ablation in symptomatic patients. But the underlying mechanism is not clearly understood. Whang et al. (2012) summarized that sympathetic activation was a well-recognized trigger for ventricular arrhythmia, while a portion of AF seemed to be initiated by parasympathetic triggers (Chen et al. 1998; Chen et al. 2007). Therefore, there could be an association between diminished heart rate variability (HRV) and ventricular arrhythmia. Additionally, depression, which has been reproducibly shown to exert negative impacts on MCS, has also been noted to be associated with reduced HRV (Musselman et al. 1998; Chen et al. 2010, 2012). Consequently, it would be reasonable to postulate that the autonomic nervous system might play a role in the reverse association between frequent VPCs and the mental part of HRQoL. However, this hypothesis requires further investigation.
This study did have certain limitations. First, even after persistent attempts to visit all of the elderly citizens in our community around the Yilan area, over 20% of the registered inhabitants refused to join this study. Even with similar age and sex distributions between the participants and the registered inhabitants, those inhabitants who for any reason failed to participate in the study might have more physical or mental disabilities. This could lead to an underestimation of the correlation between diseases and HRQoL. Second, although our study did involve using the 5-minute ECG recorder as a longer duration of monitoring, there could still be some patients with paroxysmal attacks of cardiac arrhythmias that went undetected, which might lead to underestimation of the prevalence of AF and the frequency of APCs and VPCs. However, this study still provides sound evidence of the prevalence of AF in an elderly population, and the interactions between various cardiac arrhythmia and the HRQoL from a community-based survey.
In conclusion, this study suggests that the prevalence of AF in an elderly population in Taiwan is 5.8%, which is no less than the mean global prevalence. Therefore, more aggressive strategies for improving prevention and management of AF should be undertaken. Our study results also suggest that AF patients have significantly lower scores of the physical part of HRQoL, while patients with frequent VPCs have significant and lower scores of the mental component. As HRQoL has been considered to be an important patient-centered health outcome measurement, these findings can provide more information to design effective strategies of AF management.
Acknowledgments
We are grateful for the tremendous help from Mr. De-Wei Lin and Miss Yu-Huei Lin, the conscientious project assistants who visited all of the study participants and recorded the data. We also thank Yu-Chun Chen, M.D., Ph.D., for his valuable suggestions during the preparation of this article.
This study was funded by the Research Foundation of Cardiovascular Medicine.
Conflict of Interest
The authors declare no conflict of interest.
References
-
Aliot,
E.,
Botto,
G.L.,
Crijns,
H.J. &
Kirchhof,
P.
(2014) Quality of life in patients with atrial fibrillation: how to assess it and how to improve it. Europace, 16, 787-796.
-
Alonso,
J.,
Ferrer,
M.,
Gandek,
B.,
Ware,
J.E. Jr.,
Aaronson,
N.K.,
Mosconi,
P.,
Rasmussen,
N.K.,
Bullinger,
M.,
Fukuhara,
S.,
Kaasa,
S. &
Leplege,
A.
(2004) Health-related quality of life associated with chronic conditions in eight countries: results from the International Quality of Life Assessment (IQOLA) Project. Qual. Life Res., 13, 283-298.
-
Ariansen,
I.,
Dammen,
T.,
Abdelnoor,
M.,
Tveit,
A. &
Gjesdal,
K.
(2011) Mental health and sleep in permanent atrial fibrillation patients from the general population. Clin. Cardiol., 34, 327-331.
-
Benjamin,
E.J.,
Levy,
D.,
Vaziri,
S.M.,
D’Agostino,
R.B.,
Belanger,
A.J. &
Wolf,
P.A.
(1994) Independent risk factors for atrial fibrillation in a population-based cohort. The Framingham Heart Study. JAMA, 271, 840-844.
-
Bjelland,
I.,
Dahl,
A.A.,
Haug,
T.T. &
Neckelmann,
D.
(2002) The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J. Psychosom. Res., 52, 69-77.
-
Chen,
H.C.,
Yang,
C.C.,
Kuo,
T.B.,
Su,
T.P. &
Chou,
P.
(2010) Gender differences in the relationship between depression and cardiac autonomic function among community elderly. Int. J. Geriatr. Psychiatry, 25, 314-322.
-
Chen,
H.C.,
Yang,
C.C.,
Kuo,
T.B.,
Su,
T.P. &
Chou,
P.
(2012) Cardiac vagal control and theoretical models of co-occurring depression and anxiety: a cross-sectional psychophysiological study of community elderly. BMC Psychiatry, 12, 93.
-
Chen,
L.S.,
Zhou,
S.,
Fishbein,
M.C. &
Chen,
P.S.
(2007) New perspectives on the role of autonomic nervous system in the genesis of arrhythmias. J. Cardiovasc. Electrophysiol., 18, 123-127.
-
Chen,
L.Y. &
Shen,
W.K.
(2007) Epidemiology of atrial fibrillation: a current perspective. Heart Rhythm, 4, S1-6.
-
Chen,
Y.J.,
Chen,
S.A.,
Tai,
C.T.,
Wen,
Z.C.,
Feng,
A.N.,
Ding,
Y.A. &
Chang,
M.S.
(1998) Role of atrial electrophysiology and autonomic nervous system in patients with supraventricular tachycardia and paroxysmal atrial fibrillation. J. Am. Coll. Cardiol., 32, 732-738.
-
Chien,
K.L.,
Su,
T.C.,
Hsu,
H.C.,
Chang,
W.T.,
Chen,
P.C.,
Chen,
M.F. &
Lee,
Y.T.
(2010) Atrial fibrillation prevalence, incidence and risk of stroke and all-cause death among Chinese. Int. J. Cardiol., 139, 173-180.
-
Chugh,
S.S.,
Havmoeller,
R.,
Narayanan,
K.,
Singh,
D.,
Rienstra,
M.,
Benjamin,
E.J.,
Gillum,
R.F.,
Kim,
Y.H.,
McAnulty,
J.H. Jr.,
Zheng,
Z.J.,
Forouzanfar,
M.H.,
Naghavi,
M.,
Mensah,
G.A.,
Ezzati,
M. &
Murray,
C.J.
(2014) Worldwide epidemiology of atrial fibrillation: a Global Burden of Disease 2010 Study. Circulation, 129, 837-847.
-
Creed,
F.,
Morgan,
R.,
Fiddler,
M.,
Marshall,
S.,
Guthrie,
E. &
House,
A.
(2002) Depression and anxiety impair health-related quality of life and are associated with increased costs in general medical inpatients. Psychosomatics, 43, 302-309.
-
Defaye,
P.,
Dournaux,
F. &
Mouton,
E.
(1998) Prevalence of supraventricular arrhythmias from the automated analysis of data stored in the DDD pacemakers of 617 patients: the AIDA study. The AIDA Multicenter Study Group. Automatic Interpretation for Diagnosis Assistance. Pacing Clin. Electrophysiol., 21, 250-255.
-
Dorian,
P.,
Jung,
W.,
Newman,
D.,
Paquette,
M.,
Wood,
K.,
Ayers,
G.M.,
Camm,
J.,
Akhtar,
M. &
Luderitz,
B.
(2000) The impairment of health-related quality of life in patients with intermittent atrial fibrillation: implications for the assessment of investigational therapy. J. Am. Coll. Cardiol., 36, 1303-1309.
-
Go,
A.S.,
Hylek,
E.M.,
Phillips,
K.A.,
Chang,
Y.,
Henault,
L.E.,
Selby,
J.V. &
Singer,
D.E.
(2001) Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA, 285, 2370-2375.
-
Howes,
C.J.,
Reid,
M.C.,
Brandt,
C.,
Ruo,
B.,
Yerkey,
M.W.,
Prasad,
B.,
Lin,
C.,
Peduzzi,
P. &
Ezekowitz,
M.D.
(2001) Exercise tolerance and quality of life in elderly patients with chronic atrial fibrillation. J. Cardiovasc. Pharmacol. Ther., 6, 23-29.
-
Hsu,
N.W.,
Tsao,
H.M.,
Chen,
H.C. &
Chou,
P.
(2014) Anxiety and depression mediate the health-related quality of life differently in patients with cardiovascular disease and stroke-preliminary report of the Yilan Study: a population-based community health survey. PLoS One, 9, e107609.
-
Huang,
C.X.,
Liang,
J.J.,
Yang,
B.,
Jiang,
H.,
Tang,
Q.Z.,
Liu,
X.J.,
Wan,
W.G. &
Jian,
X.L.
(2006) Quality of life and cost for patients with premature ventricular contractions by radiofrequency catheter ablation. Pacing Clin. Electrophysiol., 29, 343-350.
-
Iguchi,
Y.,
Kimura,
K.,
Aoki,
J.,
Kobayashi,
K.,
Terasawa,
Y.,
Sakai,
K. &
Shibazaki,
K.
(2008) Prevalence of atrial fibrillation in community-dwelling Japanese aged 40 years or older in Japan: analysis of 41,436 non-employee residents in Kurashiki-city. Circ. J., 72, 909-913.
-
Inoue,
H.,
Fujiki,
A.,
Origasa,
H.,
Ogawa,
S.,
Okumura,
K.,
Kubota,
I.,
Aizawa,
Y.,
Yamashita,
T.,
Atarashi,
H.,
Horie,
M.,
Ohe,
T.,
Doi,
Y.,
Shimizu,
A.,
Chishaki,
A.,
Saikawa,
T., et al.
(2009) Prevalence of atrial fibrillation in the general population of Japan: an analysis based on periodic health examination. Int. J. Cardiol., 137, 102-107.
-
Jenkins,
L.S.,
Brodsky,
M.,
Schron,
E.,
Chung,
M.,
Rocco,
T. Jr.,
Lader,
E.,
Constantine,
M.,
Sheppard,
R.,
Holmes,
D.,
Mateski,
D.,
Floden,
L.,
Prasun,
M.,
Greene,
H.L. &
Shemanski,
L.
(2005) Quality of life in atrial fibrillation: the Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) study. Am. Heart J., 149, 112-120.
-
Kang,
Y. &
Bahler,
R.
(2004) Health-related quality of life in patients newly diagnosed with atrial fibrillation. Eur. J. Cardiovasc. Nurs., 3, 71-76.
-
Kuo,
T.B.,
Lin,
T.,
Yang,
C.C.,
Li,
C.L.,
Chen,
C.F. &
Chou,
P.
(1999) Effect of aging on gender differences in neural control of heart rate. Am. J. Physiol., 277, H2233-H2239.
-
Lam,
C.L.,
Pan,
P.C.,
Chan,
A.W.,
Chan,
S.Y. &
Munro,
C.
(1995) Can the Hospital Anxiety and Depression (HAD) Scale be used on Chinese elderly in general practice? Fam. Pract., 12, 149-154.
-
Lee,
C.H.,
Liu,
P.Y.,
Tsai,
L.M.,
Tsai,
W.C.,
Ho,
M.T.,
Chen,
J.H. &
Lin,
L.J.
(2007) Characteristics of hospitalized patients with atrial fibrillation in Taiwan: a nationwide observation. Am. J. Med., 120, 819. e1-7.
-
Lim,
L.,
Jin,
A.Z. &
Ng,
T.P.
(2012) Anxiety and depression, chronic physical conditions, and quality of life in an urban population sample study. Soc. Psychiatry Psychiatr. Epidemiol., 47, 1047-1053.
-
Maruish,
M.E. &
Turner-Bowker,
D.M.
(2009) A guide to the development of certified modes of Short Form survey administration, QualityMetric Incorporated, RI.
-
Mohanty,
S.,
Santangeli,
P.,
Mohanty,
P.,
Di Biase,
L.,
Holcomb,
S.,
Trivedi,
C.,
Bai,
R.,
Burkhardt,
D.,
Hongo,
R.,
Hao,
S.,
Beheiry,
S.,
Santoro,
F.,
Forleo,
G.,
Gallinghouse,
J.G.,
Horton,
R., et al.
(2014) Catheter ablation of asymptomatic longstanding persistent atrial fibrillation: impact on quality of life, exercise performance, arrhythmia perception, and arrhythmia-free survival. J. Cardiovasc. Electrophysiol., 25, 1057-1064.
-
Musselman,
D.L.,
Evans,
D.L. &
Nemeroff,
C.B.
(1998) The relationship of depression to cardiovascular disease: epidemiology, biology, and treatment. Arch. Gen. Psychiatry, 55, 580-592.
-
Myerburg,
R.J.,
Kessler,
K.M.,
Luceri,
R.M.,
Zaman,
L.,
Trohman,
R.G.,
Estes,
D. &
Castellanos,
A.
(1984) Classification of ventricular arrhythmias based on parallel hierarchies of frequency and form. Am. J. Cardiol., 54, 1355-1358.
-
Ohlmeier,
C.,
Mikolajczyk,
R.,
Haverkamp,
W. &
Garbe,
E.
(2013) Incidence, prevalence, and antithrombotic management of atrial fibrillation in elderly Germans. Europace, 15, 1436-1444.
-
Paquette,
M.,
Roy,
D.,
Talajic,
M.,
Newman,
D.,
Couturier,
A.,
Yang,
C. &
Dorian,
P.
(2000) Role of gender and personality on quality-of-life impairment in intermittent atrial fibrillation. Am. J. Cardiol., 86, 764-768.
-
Piccini,
J.P.,
Hammill,
B.G.,
Sinner,
M.F.,
Jensen,
P.N.,
Hernandez,
A.F.,
Heckbert,
S.R.,
Benjamin,
E.J. &
Curtis,
L.H.
(2012) Incidence and prevalence of atrial fibrillation and associated mortality among Medicare beneficiaries, 1993-2007. Circ. Cardiovasc. Qual. Outcomes, 5, 85-93.
-
Reynolds,
M.R.,
Lavelle,
T.,
Essebag,
V.,
Cohen,
D.J. &
Zimetbaum,
P.
(2006) Influence of age, sex, and atrial fibrillation recurrence on quality of life outcomes in a population of patients with new-onset atrial fibrillation: the Fibrillation Registry Assessing Costs, Therapies, Adverse events and Lifestyle (FRACTAL) study. Am. Heart J., 152, 1097-1103.
-
Roalfe,
A.K.,
Bryant,
T.L.,
Davies,
M.H.,
Hackett,
T.G.,
Saba,
S.,
Fletcher,
K.,
Lip,
G.Y.,
Hobbs,
F.D. &
Mant,
J.
(2012) A cross-sectional study of quality of life in an elderly population (75 years and over) with atrial fibrillation: secondary analysis of data from the Birmingham Atrial Fibrillation Treatment of the Aged study. Europace, 14, 1420-1427.
-
Schnabel,
R.B.,
Yin,
X.,
Gona,
P.,
Larson,
M.G.,
Beiser,
A.S.,
McManus,
D.D.,
Newton-Cheh,
C.,
Lubitz,
S.A.,
Magnani,
J.W.,
Ellinor,
P.T.,
Seshadri,
S.,
Wolf,
P.A.,
Vasan,
R.S.,
Benjamin,
E.J. &
Levy,
D.
(2015) 50 year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham Heart Study: a cohort study. Lancet, 386, 154-162.
-
Shinohara,
M.,
Kobayashi,
Y.,
Obara,
C.,
Miyata,
A.,
Chiyoda,
K.,
Nakagawa,
H.,
Tanno,
K.,
Kikushima,
S.,
Baba,
T. &
Katagiri,
T.
(1999) Neurally mediated syncope and arrhythmias: a study of syncopal patients using the head-up tilt test. Jpn. Circ. J., 63, 339-342.
-
Singer,
M.A.,
Hopman,
W.M. &
MacKenzie,
T.A.
(1999) Physical functioning and mental health in patients with chronic medical conditions. Qual. Life Res., 8, 687-691.
-
Stewart,
A.L.,
Greenfield,
S.,
Hays,
R.D.,
Wells,
K.,
Rogers,
W.H.,
Berry,
S.D.,
McGlynn,
E.A. &
Ware,
J.E. Jr.
(1989) Functional status and well-being of patients with chronic conditions. Results from the Medical Outcomes Study. JAMA, 262, 907-913.
-
Strickberger,
S.A.,
Ip,
J.,
Saksena,
S.,
Curry,
K.,
Bahnson,
T.D. &
Ziegler,
P.D.
(2005) Relationship between atrial tachyarrhythmias and symptoms. Heart Rhythm, 2, 125-131.
-
Thrall,
G.,
Lane,
D.,
Carroll,
D. &
Lip,
G.Y.
(2006) Quality of life in patients with atrial fibrillation: a systematic review. Am. J. Med., 119, 448. e1-e19.
-
Tseng,
H.M.,
Lu,
J.F. &
Tsai,
Y.J.
(2003) Assessment of health-related quality of life in Taiwan (II): norming and validation of SF-36 Taiwan version. Taiwan Journal of Public Health, 22, 512-518.
-
van den Berg,
M.P.,
Hassink,
R.J.,
Tuinenburg,
A.E.,
van Sonderen,
E.F.,
Lefrandt,
J.D.,
de Kam,
P.J.,
van Gelder,
I.C.,
Smit,
A.J.,
Sanderman,
R. &
Crijns,
H.J.
(2001) Quality of life in patients with paroxysmal atrial fibrillation and its predictors: importance of the autonomic nervous system. Eur. Heart J., 22, 247-253.
-
Whang,
W.,
Davidson,
K.W.,
Conen,
D.,
Tedrow,
U.B.,
Everett,
B.M. &
Albert,
C.M.
(2012) Global psychological distress and risk of atrial fibrillation among women: the Women’s Health Study. J. Am. Heart Assoc., 1, e001107.
-
Wilke,
T.,
Groth,
A.,
Mueller,
S.,
Pfannkuche,
M.,
Verheyen,
F.,
Linder,
R.,
Maywald,
U.,
Bauersachs,
R. &
Breithardt,
G.
(2013) Incidence and prevalence of atrial fibrillation: an analysis based on 8.3 million patients. Europace, 15, 486-493.
-
Yamamoto,
M.,
Watanabe,
E.,
Suzuki,
T.,
Yamazaki,
T.,
Ohtsu,
H.,
Ozaki,
Y.,
Ogawa,
S. &
Yamashita,
T.
(2014) Association between the quality of life and asymptomatic episodes of paroxysmal atrial fibrillation in the J-RHYTHM II study. J. Cardiol., 64, 64-69.
-
Yap,
K.B.,
Ng,
T.P. &
Ong,
H.Y.
(2008) Low prevalence of atrial fibrillation in community-dwelling Chinese aged 55 years or older in Singapore: a population-based study. J. Electrocardiol., 41, 94-98.
-
Zigmond,
A.S. &
Snaith,
R.P.
(1983) The hospital anxiety and depression scale. Acta Psychiatr. Scand., 67, 361-370.