Abstract
Nogo-B, located in the endoplasmic reticulum, is an isoform belonging to the reticulon protein family, which is expressed specifically in cholangiocytes and non-parenchymal cells in the liver. Nogo-B expression is down-regulated with the progression of liver fibrosis, but its distinct function in liver malignancies has not been fully clarified. We have hypothesized that Nogo-B expression may be altered in intrahepatic cholangiocarcinoma (ICC), a relatively rare type of primary liver cancer with highly malignant behavior. The present study aimed to investigate the relationship between Nogo-B expression, assessed by immunohistochemical staining, and clinicopathological factors and prognosis in 34 ICC patients. Positive expression was observed in 19 (56%) of 34 ICC specimens: 6 patients (18%) with positivity levels of 1+ (positive cells in 10-50% of cancer cells) and 13 patients (38%) with 2+ (positive cells over 50%). Importantly, the remaining 15 patients (44%) were categorized as negative expression (Nogo-B-positive cells, less than 10%). Conversely, the mass-forming type of ICC tended to express Nogo-B with the degree of 2+ positivity, compared to the periductal infiltration type (p = 0.064), and the mass-forming type showed a better 5-year survival rate (66% vs. 5%) after hepatectomy (p < 0.05). However, the degree of positivity was not associated with tumor relapse rate, disease-free and overall survival, although each of the periductal infiltration type, intrahepatic metastasis, larger tumor size, and lower microvessel counts was associated with lower survival rates. We propose that Nogo-B expression is down-regulated in ICC, the implication of which, however, remains to be investigated.
Introduction
Peripheral intrahepatic cholangiocarcinoma (ICC) is a relatively rare type of primary liver cancer that shows highly malignant behavior (Kokudo and Makuuchi 2002; Poultsides et al. 2010). Although hepatic resection is currently the only curative option for radical treatment of ICC, the cancer recurrence rate after resection remains high and patient survival is still unsatisfactory. Although some conventional clinicopathological and operative factors in ICC have been shown to be related to oncological features or patient prognosis, useful markers that could indicate an ICC patient’s prognosis are largely unknown (Malaguarnera et al. 2013). In addition, the mechanisms underlining malignant behavior of ICC are not fully elucidated (Sirica et al. 2009; Malaguarnera et al. 2013).
Nogo isoforms (Nogo-A, -B and -C) belong to the reticulon family of proteins (Dodd et al. 2005). These share a reticulon homology domain containing a 66-amino-acid loop domain. Nogo-B (Reticulon 4B) is a 55-kDa protein located in the endoplasmic reticulum and is widely expressed in many cell types (Harrison et al. 2009). In the liver, Nogo-B is expressed specifically in cholangiocytes and non-parenchymal cells, but not in hepatocytes (Zhang et al. 2011). Studies in cirrhotic patients and experimental models of fibrosis/cirrhosis suggest that Nogo-B is down-regulated in liver fibrotic/cirrhosis or apoptosis of hepatic stellate cells (Tashiro et al. 2013; Men et al. 2015). Further, deletion of Nogo-B results in amelioration of liver cirrhosis and portal hypertension in mice with biliary cirrhosis (Tashiro et al. 2013; Men et al. 2015). From the above previous reports, given that Nogo-B is expressed in cholangiocytes and that deletion of Nogo-B results in attenuation of biliary cirrhosis in which cholangiocyte proliferation plays a central role (Zhang et al. 2011), we hypothesized that decreased Nogo-B expression might stimulate cancer cell proliferation, tumor growth or invasion, and may play a significant role in poor prognosis of patients with ICC. Currently, the roles of Nogo-B in hepatobiliary malignancies have not been fully determined (Liu et al. 2014).
In the present study, to test our hypothesis, we examined the relationship between prognosis and expression of Nogo-B in ICC using immunohistochemical staining methods and conventional clinicopathological factors of 34 patients with ICC who underwent hepatic resection.
Materials and Methods
Patients
A total of 34 consecutive patients (20 men, 14 women) with ICC who were admitted to Nagasaki University Graduate School of Biomedical Sciences (NUGSBS) between 1997 and 2012 (minimum follow-up 24 months) were analyzed retrospectively in this study. Data were retrieved from both anesthetic and patient charts to cover the period of hospitalization following hepatectomy. The study design was approved by the Ethics Review Board of our Institute and signed consent for clinical research using tissue or blood samples was obtained from each patient. Follow-up included measurement of serum tumor markers and abdominal computed tomography (CT) every 3-6 months. Pathological and morphological parameters, macroscopic findings and Japanese tumor-node-metastasis (TNM) classification, which were compared to Nogo-B expressions, were used as defined by the Liver Cancer Study Group of Japan (Liver Cancer Study group of Japan 2003).
Immunohistochemical staining
Resected specimens were fixed in 10% formalin and embedded in paraffin. Thin sections (4 μm) were deparaffinized twice using xylene and rehydrated in an ethanol series (100%, 90%, and 80%). Sections were then treated with 3% of H2O2 for 30 minutes to inhibit intrinsic peroxidase. For Nogo-B, to inhibit non-specific reactions, specimens were treated by normal rabbit serum for 10 min. A 100-fold diluted antibody to Nogo-B (goat anti-human Nogo-B; N-18, Santa Cruz Biotechnology, Santa Cruz, CA; recognizing epitopes 1-18) (Zhang et al. 2011) was used as a primary antibody and reacted overnight at 4°C. The Simple Stain max PO (mouse, monoclonal; Cosmo Bio, Carlsbad, CA, USA) was used as a secondary antibody and reacted for 30 min.
For CD34 and proliferating cell nuclear antigen (PCNA) staining, tissue sections were digested with 0.2% trypsin in 0.01 mol/l phosphate-buffered saline (PBS) for 20 min at 37°C. Sections were incubated overnight at 4°C with mouse monoclonal antibody to CD34 (1:25, QB-END/10; Novocastra Laboratories, Newcastle, UK), or for 1 h at room temperature with 1:100 diluted monoclonal mouse antibody to PCNA antibody (PC-10; Dako) as the primary antibody. This was followed by reaction with biotinylated anti-immunoglobulin and reagent using labeled streptavidin-biotin (LSAB) kit peroxidase (Dako). The peroxidase reaction was visualized with 0.01% H2O2 and 3,3′-diaminobenzidine under light microscopy (×200) (Nanashima et al. 2004).
For Nogo-B (Fig. 1a-c), staining of fewer than 10% of cells was defined as negative expression, that between 10 and 50% was defined as positive expression (1+), and that over 50% was defined as positive expression (2+). A positive control was defined on an intra-Glissonian cholangiole in the normal liver specimen (Fig. 1d). Fig. 1e shows the 2+ positivity of Nogo-B expression in both cholangiole and cholangiocarcinoma. For microvessel counts using CD34 staining, an average count was determined for the five most vascular areas in the section examined under ×200 magnification. The average percentage of cells exhibiting positive PCNA nuclear expression among 1,000 nuclei in five areas of the tumor was estimated.
Statistical analysis
Continuous data are expressed as mean ± standard deviation. Data from different groups were compared using one-way analysis of variance and examined with Student’s t-test or Dunnett’s multiple comparison test. Categorical data were analyzed using Fisher’s exact test. Survival rates were calculated according to the Kaplan-Meier method, and differences between groups were tested for significance using the log-rank test. Two-tailed values of p < 0.05 were considered statistically significant. Statistical Package for the Social Science (SPSS) version 18.0 software (SPSS, Chicago, IL, USA) was used for all statistical analyses.
Results
Expression of Nogo-B and relationship with microvessel counts, proliferation activity or clinicopathological feature
Nogo-B is expressed in the normal cholangiole, the staining intensity of which was equivalent to (2+) positivity (Fig. 1). In contrast, negative expression of Nogo-B was observed in 15 patients (46%). Positive expression of Nogo-B was found in 19 patients (56%): (1+) positivity in 6 patients (18%) and (2+) positivity in 13 patients (38%). Thus, among the 34 patients, 21 patients (62%) showed the smaller population of Nogo-B-positive cancer cells: 15 patients with negative expression and 6 patients with (1+) positivity.
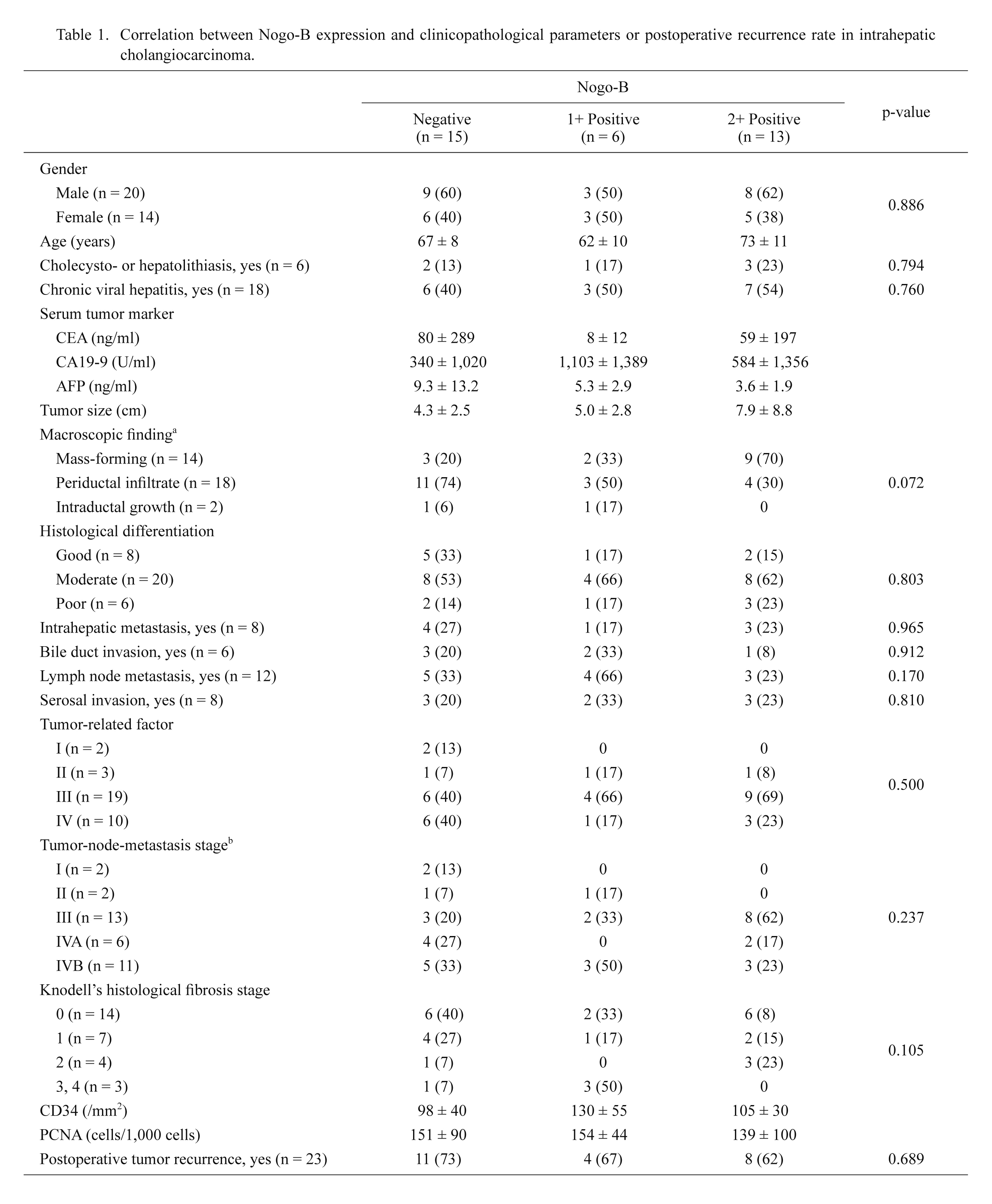
The relationships between Nogo-B expression and clinicopathological features were examined, and the results are shown in Table 1. Prevalence of strong Nogo-B expression in the mass-forming type of ICC was slightly higher than that in the periductal infiltration types (p = 0.064). Otherwise, Nogo-B expression was not significantly associated with other tumor-related clinic-pathological parameters of ICC or prevalence of tumor relapse. Nogo-B expression was not significantly associated with the presence of chronic liver injury and degree of fibrosis, microvessel counts (CD34) or PCNA labeling index of tumors (Table 1). The median microvessel count by CD34 was 126 ± 52 /mm2 and a median PCNA labeling index of 149 ± 78 /field (×200) was applied as a cutoff value (Table 2).
Relationship between Nogo-B expression and patient prognosis
Table 2 shows the relationship between disease-free and overall survival rate and clinicopathological factors including expression of Nogo-B. Periductal infiltrating type of ICC, intrahepatic metastasis and lower CD34 level were significantly associated with a lower 3-year disease-free survival rate after hepatectomy (p < 0.05). In addition, higher blood loss tended to be associated with lower 3-year disease-free survival rate (p = 0.075). Nogo-B positivity level was not significantly associated with disease-free survival rate (Table 2, Fig. 2a). With respect to 5-year overall survival rates after hepatectomy, each of periductal infiltrating type, intrahepatic metastasis, and tumor size was significantly associated with a lower 5-year survival rate (p < 0.05). Nogo-B positivity was not significantly associated with overall survival rate (Table 2, Fig. 2b).
Discussion
Various biological factors of ICC have been reported as candidates for prognostic markers (Cao 2008; Nanashima et al. 2008; Nathan et al. 2009). In both preliminary studies (Nanashima et al. 2009) and the present study, we focused on microvessel counts or tumor enhancement patterns by CT as markers of tumor angiogenesis for ICC. We propose the inclusion of this examination in conventional pathological diagnosis to predict tumor malignancy because of the simplicity of examining immunohistochemistry. Tumor angiogenesis can be related to patient prognosis in ICC for those who undergo radical hepatectomy (Cao 2008; Nanashima et al. 2008, 2009; Nathan et al. 2009; Thelen et al. 2010). However, few new markers associated with prognosis or malignant behavior of ICC has been determined (Oishi et al. 2012; Shimada et al. 2010). In this study we studied Nogo-B, which has recently been identified as a potential marker of hepatic fibrosis (Zhang et al. 2011; Gao et al. 2013; Tashiro et al. 2013; Men et al. 2015) and as a potential enhancer of bile duct proliferation (Zhang et al. 2011). In addition, studies showed that Nogo-B can be a promising parameter for lower malignancy in breast or lung carcinomas (Wang et al. 2013; Pula et al. 2014). Nogo-B expression indicates neuronal regeneration in the central nervous system, and was identical to that of the apoptosis-inducing gene in human carcinomas (Li et al. 2001). On the other hand, Nogo-B was associated with epithelial-mesenchymal transition and cellular migration of a cervical carcinoma cell line (Xiao et al. 2013). It remains unclear whether Nogo-B expression is closely related to digestive tract carcinogenesis. The mechanism of Nogo-B expression in the digestive tract has not been fully clarified at this stage. In hepatocellular carcinoma (HCC), another Nogo isoform was closely related to progression of liver cirrhosis and tumor carcinogenesis (Liu et al. 2014). Nogo-C is a tumor suppressor gene in HCC but the role of Nogo-B is known only in the development of liver fibrosis.
Regarding the cause of carcinogenesis in ICC, existence of biliary stones, chronic viral hepatitis and patient occupation have been proposed to be related factors (Poultsides et al. 2010; Malaguarnera et al. 2013). Nogo-B expression was related to the progression of chronic liver injury, hepatic fibrosis and portal hypertension as above. Thus, we proposed to examine the correlation between Nogo-B expression and clinicopathological malignant behavior of ICC in this study. However, we found that expression of Nogo-B was not associated with factors of chronic liver or biliary injuries and we were unable to speculate on the mechanism of specific carcinogenesis in ICC.
Significant Nogo-B positivity was observed in mass-forming type by macroscopic findings, and this type exhibited a lower malignant potential in ICC (Shimada et al. 2007; Yamamoto et al. 2009). This type may not infiltrate along intrahepatic ducts and invade adjacent lymphatic or venous ducts and perineural tissues, which can lead to lower tumor metastasis and better prognosis. On the other hand, periductal infiltration type, showing cancer migration to Glissonian vessels, has a worse prognosis. The role of Nogo-B expression for cell-cell adhesion in biliary cancer has not been clarified yet. Nogo-B expression induced apoptosis in cancer cells and this might indicate non-aggressiveness of biliary cancer cells. Microvessel density, as indicated by CD34 and PCNA, is a remarkable prognostic factor in malignant tumors, including ICC (Ohashi et al. 1994; Nanashima et al. 2009). However, relationship between these oncological parameters and Nogo-B positivity has also not been fully elucidated. The associations between Nogo-B expression and these markers were not significantly correlated in the present study. Thus, malignant cancer behavior of Nogo-B was not observed by our results.
The goal of this study was to clarify the relationship between promising biological parameters and survival in patients with ICC. Predictive factors for patient prognosis have been proposed by many investigators, but no consensus has yet been reached (Cao 2008; Nathan et al. 2009; Sempoux et al. 2011). The present study showed that periductal infiltration type and intrahepatic metastasis were associated with lower disease-free survival rate, as in previous reports (Yamamoto et al. 2009; Yamamoto and Ariizumi 2011; Yeh et al. 2013). Expression of Nogo-B was not significantly associated with disease-free and overall survival rate. In the present study, the number of participants was limited and therefore multivariate analysis was not performed. If a larger number of subjects could be obtained, discrimination of survivals between staining intensity would be significant. Peripheral ICC is a relatively rare liver malignancy, comprising around 3% of resectable primary liver cancers, and therefore it is difficult to increase the sample size at a single institute (Ikai et al. 2004). To resolve this problem, a further study in a larger population of patients at multiple institutes is necessary. As ICC is not a common disease, a multi-institutional comprehensive study to investigate various candidate factors is required.
In conclusion, the present study examined the relationship of Nogo-B expression as a marker of chronic liver injury with clinicopathological features and survival in 34 patients with ICC. Out of the 34 patients, 21 patients (62%) showed the smaller population of Nogo-B-positive cancer cells: negative expression in 15 patients and (1+) positivity in 6 patients. Thus, Nogo-B expression might be down-regulated in ICC, which may cause the malignant behavior of ICC, including tumor infiltration. As a tumor biological factor, Nogo-B expression was associated with mass-forming type of ICC, the most popular phenotype. However, Nogo-B expression was not significantly associated with any clinicopathological parameters, tumor relapse rate or prognosis at all. A further study in a larger population of patients with ICC undergoing surgical resection will clarify the role of Nogo-B expression in ICC.
Acknowledgments
We would like to thank Dr. Kazunori Shibao (the First Department of Surgery, University of Occupational and Environmental Health, Fukuoka, Japan) for kindly providing us with Nogo-B antibody.
Conflict of Interest
The authors declare no conflict of interest.
References
-
Cao,
Y.
(2008) Molecular mechanisms and therapeutic development of angiogenesis inhibitors. Adv. Cancer Res., 100, 113-131.
-
Dodd,
D.A.,
Niederoest,
B.,
Bloechlinger,
S.,
Dupuis,
L.,
Loeffler,
J.P. &
Schwab,
M.E.
(2005) Nogo-A, -B, and -C are found on the cell surface and interact together in many different cell types. J. Biol. Chem., 280, 12494-12502.
-
Gao,
L.,
Utsumi,
T.,
Tashiro,
K.,
Liu,
B.,
Zhang,
D.,
Swenson,
E.S. &
Iwakiri,
Y.
(2013) Reticulon 4B (Nogo-B) facilitates hepatocyte proliferation and liver regeneration in mice. Hepatology, 57, 1992-2003.
-
Harrison,
K.D.,
Miao,
R.Q.,
Fernandez-Hernándo,
C.,
Suárez,
Y.,
Dávalos,
A. &
Sessa,
W.C.
(2009) Nogo-B receptor stabilizes Niemann-Pick type C2 protein and regulates intracellular cholesterol trafficking. Cell Metab., 10, 208-218.
-
Ikai,
I.,
Itai,
Y.,
Okita,
K.,
Omata,
M.,
Kojiro,
M.,
Kobayashi,
K.,
Nakanuma,
Y.,
Futagawa,
S.,
Makuuchi,
M. &
Yamaoka,
Y.
(2004) Report of the 15th follow-up survey of primary liver cancer. Hepatol. Res., 28, 21-29.
-
Kokudo,
N. &
Makuuchi,
M.
(2002) Extent of resection and outcome after curative resection for intrahepatic cholangiocarcinoma. Surg. Oncol. Clin. N. Am., 11, 969-983.
-
Li,
Q.,
Qi,
B.,
Oka,
K.,
Shimakage,
M.,
Yoshioka,
N.,
Inoue,
H.,
Hakura,
A.,
Kodama,
K.,
Stanbridge,
E.J. &
Yutsudo,
M.
(2001) Link of a new type of apoptosis-inducing gene ASY/Nogo-B to human cancer. Oncogene, 20, 3929-3936.
-
Liu,
X.,
Cui,
S.J.,
Zhu,
S.J.,
Geng,
D.C. &
Yu,
L.
(2014) Nogo-C contributes to HCC tumorigenesis via suppressing cell growth and its interactome analysis with comparative proteomics research. Int. J. Clin. Exp. Pathol., 7, 2044-2055.
-
Liver Cancer Study group of Japan
(2003) Part I Clinical findings. In: The General Rules for the Clinical and Pathological Study of Primary Liver Cancer, 2nd English ed., Kanehara Co., Ltd., Tokyo, pp. 6-28.
-
Malaguarnera,
G.,
Paladina,
I.,
Giordano,
M.,
Malaguarnera,
M.,
Bertino,
G. &
Berretta,
M.
(2013) Serum markers of intrahepatic cholangiocarcinoma. Dis. Markers, 34, 219-228.
-
Men,
R.,
Wen,
M.,
Dan,
X.,
Zhu,
Y.,
Wang,
W.,
Li,
J.,
Wu,
W.,
Liu,
X. &
Yang,
L.
(2015) Nogo-B: A potential indicator for hepatic cirrhosis and regulator in hepatic stellate cell activation. Hepatol. Res., 45, 113-122.
-
Nanashima,
A.,
Shibata,
K.,
Nakayama,
T.,
Tobinaga,
S.,
Araki,
M.,
Kunizaki,
M.,
Takeshita,
H.,
Hidaka,
S.,
Sawai,
T.,
Nagayasu,
T. &
Tagawa,
T.
(2009) Relationship between microvessel count and postoperative survival in patients with intrahepatic cholangiocarcinoma. Ann. Surg. Oncol., 16, 2123-2129.
-
Nanashima,
A.,
Sumida,
Y.,
Abo,
T.,
Oikawa,
M.,
Murakami,
G.,
Takeshita,
H.,
Fukuoka,
H.,
Hidaka,
S.,
Nagayasu,
T.,
Sakamoto,
I. &
Sawai,
T.
(2008) Relationship between pattern of tumor enhancement and clinicopathologic characteristics in intrahepatic cholangiocarcinoma. J. Surg. Oncol., 98, 535-539.
-
Nanashima,
A.,
Yano,
H.,
Yamaguchi,
H.,
Tanaka,
K.,
Shibasaki,
S.,
Sumida,
Y.,
Sawai,
T.,
Shindou,
H. &
Nakagoe,
T.
(2004) Immunohistochemical analysis of tumor biological factors in hepatocellular carcinoma: relationship to clinicopathological factors and prognosis after hepatic resection. J. Gastroenterol., 39, 148-154.
-
Nathan,
H.,
Aloia,
T.A.,
Vauthey,
J.N.,
Abdalla,
E.K.,
Zhu,
A.X.,
Schulick,
R.D.,
Choti,
M.A. &
Pawlik,
T.M.
(2009) A proposed staging system for intrahepatic cholangiocarcinoma. Ann. Surg. Oncol., 16, 14-22.
-
Ohashi,
K.,
Nakajima,
Y.,
Tsutsumi,
M.,
Kanehiro,
H.,
Fukuoka,
T.,
Hisanaga,
M.,
Taki,
J.,
Nakae,
D.,
Konishi,
Y. &
Nakano,
H.
(1994) Clinical characteristics and proliferating activity of intrahepatic cholangiocarcinoma. J. Gastroenterol. Hepatol., 9, 442-446.
-
Oishi,
N.,
Kumar,
M.R.,
Roessler,
S.,
Ji,
J.,
Forgues,
M.,
Budhu,
A.,
Zhao,
X.,
Andersen,
J.B.,
Ye,
Q.H.,
Jia,
H.L.,
Qin,
L.X.,
Yamashita,
T.,
Woo,
H.G.,
Kim,
Y.J.,
Kaneko,
S., et al.
(2012) Transcriptomic profiling reveals hepatic stem-like gene signatures and interplay of miR-200c and epithelial-mesenchymal transition in intrahepatic cholangiocarcinoma. Hepatology, 56, 1792-1803.
-
Poultsides,
G.A.,
Zhu,
A.X.,
Choti,
M.A. &
Pawlik,
T.M.
(2010) Intrahepatic cholangiocarcinoma. Surg. Clin. North Am., 90, 817-837.
-
Pula,
B.,
Werynska,
B.,
Olbromski,
M.,
Muszczynska-Bernhard,
B.,
Chabowski,
M.,
Janczak,
D.,
Zabel,
M.,
Podhorska-Okolow,
M. &
Dziegiel,
P.
(2014) Expression of Nogo isoforms and Nogo-B receptor (NgBR) in non-small cell lung carcinomas. Anticancer Res., 34, 4059-4068.
-
Sempoux,
C.,
Jibara,
G.,
Ward,
S.C.,
Fan,
C.,
Qin,
L.,
Roayaie,
S.,
Fiel,
M.I.,
Schwartz,
M. &
Thung,
S.N.
(2011) Intrahepatic cholangiocarcinoma: new insights in pathology. Semin. Liver Dis., 31, 49-60.
-
Shimada,
K.,
Sano,
T.,
Sakamoto,
Y.,
Esaki,
M.,
Kosuge,
T. &
Ojima,
H.
(2007) Surgical outcomes of the mass-forming plus periductal infiltrating types of intrahepatic cholangiocarcinoma: a comparative study with the typical mass-forming type of intrahepatic cholangiocarcinoma. World J. Surg., 31, 2016-2022.
-
Shimada,
M.,
Sugimoto,
K.,
Iwahashi,
S.,
Utsunomiya,
T.,
Morine,
Y.,
Imura,
S. &
Ikemoto,
T.
(2010) CD133 expression is a potential prognostic indicator in intrahepatic cholangiocarcinoma. J. Gastroenterol., 45, 896-902.
-
Sirica,
A.E.,
Dumur,
C.I.,
Campbell,
D.J.,
Almenara,
J.A.,
Ogunwobi,
O.O. &
Dewitt,
J.L.
(2009) Intrahepatic cholangiocarcinoma progression: prognostic factors and basic mechanisms. Clin. Gastroenterol. Hepatol., 7, S68-78.
-
Tashiro,
K.,
Satoh,
A.,
Utsumi,
T.,
Chung,
C. &
Iwakiri,
Y.
(2013) Absence of Nogo-B (reticulon 4B) facilitates hepatic stellate cell apoptosis and diminishes hepatic fibrosis in mice. Am. J. Pathol., 182, 786-795.
-
Thelen,
A.,
Scholz,
A.,
Weichert,
W.,
Wiedenmann,
B.,
Neuhaus,
P.,
Gessner,
R.,
Benckert,
C. &
Jonas,
S.
(2010) Tumor-associated angiogenesis and lymphangiogenesis correlate with progression of intrahepatic cholangiocarcinoma. Am. J. Gastroenterol., 105, 1123-1132.
-
Wang,
B.,
Zhao,
B.,
North,
P.,
Kong,
A.,
Huang,
J. &
Miao,
Q.R.
(2013) Expression of NgBR is highly associated with estrogen receptor alpha and survivin in breast cancer. PLoS One, 8, e78083.
-
Xiao,
W.,
Zhou,
S.,
Xu,
H.,
Li,
H.,
He,
G.,
Liu,
Y. &
Qi,
Y.
(2013) Nogo-B promotes the epithelial-mesenchymal transition in HeLa cervical cancer cells via Fibulin-5. Oncol. Rep., 29, 109-116.
-
Yamamoto,
M. &
Ariizumi,
S.
(2011) Surgical outcomes of intrahepatic cholangiocarcinoma. Surg. Today, 41, 896-902.
-
Yamamoto,
Y.,
Shimada,
K.,
Sakamoto,
Y.,
Esaki,
M.,
Nara,
S.,
Ban,
D.,
Kosuge,
T. &
Ojima,
H.
(2009) Clinicopathological characteristics of intrahepatic cholangiocellular carcinoma presenting intrahepatic bile duct growth. J. Surg. Oncol., 99, 161-165.
-
Yeh,
C.N.,
Yeh,
T.S.,
Chen,
T.C.,
Jan,
Y.Y. &
Chen,
M.F.
(2013) Gross pathological classification of peripheral cholangiocarcinoma determines the efficacy of hepatectomy. J. Gastroenterol., 48, 647-659.
-
Zhang,
D.,
Utsumi,
T.,
Huang,
H.C.,
Gao,
L.,
Sangwung,
P.,
Chung,
C.,
Shibao,
K.,
Okamoto,
K.,
Yamaguchi,
K.,
Groszmann,
R.J.,
Jozsef,
L.,
Hao,
Z.,
Sessa,
W.C. &
Iwakiri,
Y.
(2011) Reticulon 4B (Nogo-B) is a novel regulator of hepatic fibrosis. Hepatology, 53, 1306-1315.