Abstract
Diet and food intake play an important role in the development of osteoporosis. However, apart from calcium and vitamin D, how nutrients affect bone status is not fully understood. The purpose of this study was to determine cross-sectional and longitudinal associations between dietary intake and bone mineral density (BMD) in Japanese postmenopausal women. This 5-year cohort study included 600 community-dwelling women aged 55-74 years at baseline in 2005. Information on demographics, nutrition, and lifestyle was obtained through interviews, and nutritional and dietary intake was assessed using a validated food frequency questionnaire. BMD measurements were performed by dual energy X-ray absorptiometry. In 2010, 498 women underwent follow-up BMD examinations. Multiple linear regression analysis was performed to determine associations of predictor variables with BMD, adjusting for confounders. In cross-sectional analyses, coffee or black tea consumption was positively associated with lumbar spine (P = 0.004) and total hip (P = 0.003) BMD, and alcohol intake was positively associated with femoral neck (P = 0.005) and total hip (P = 0.001) BMD. In longitudinal analyses, vitamin K (P = 0.028) and natto (fermented soybeans) (P = 0.023) were positively associated with lumbar spine BMD, and meat or meat product consumption was inversely associated with total hip (P = 0.047) BMD. In conclusion, dietary factors other than calcium and vitamin D intake are predictors of bone mass and bone loss in Japanese postmenopausal women. In particular, natto intake is recommended for preventing postmenopausal bone loss on the basis of current evidence.
Introduction
Osteoporosis, a condition characterized by generalized skeletal fragility, is a global public health concern due to increased medical costs and decreased quality of life. Reduced bone strength causes fractures (e.g., hip fracture and vertebral fracture), referred to as osteoporotic fractures, with minimal trauma (Marcus et al. 2013). The prevalence of osteoporosis is increasing in aging populations. In Japan, where the estimated number of individuals with osteoporosis exceeds 13 million (Iki 2014), prevention of osteoporosis has become a focus of attention. Osteoporosis prevention targets postmenopausal women, who suffer from postmenopausal bone loss due to decreased levels of estrogen (Norman and Henry 2015). In this context, important strategies for this population include the maintenance of bone mineral density (BMD) by controlling modifiable lifestyle factors associated with osteoporosis.
Diet and food intake play an important role in the development of osteoporosis (Levis and Lagari 2012) because foods contain skeletally beneficial nutrients including calcium, vitamin D, flavonoids, and other minerals and vitamins (Weaver et al. 2012; Nieves 2013). Previous epidemiological studies have shown that adequate dietary protein, calcium, vitamin D, fruits, and vegetables have positive effects on bone health, and that alcohol, coffee, and tea may also have some effects (Levis and Lagari 2012). However, evidence is based mainly on European and North American populations, and only a few cohort studies have investigated food intake and osteoporosis in Japanese populations (Ikeda et al. 2006; Sato et al. 2015).
We conducted a cohort study to clarify the effects of calcium and vitamin D on postmenopausal bone loss from 2005 to 2010 (Nakamura et al. 2008; Kitamura et al. 2013), and also explored dietary factors other than calcium and vitamin D that are correlated with bone mass. In this study, we aimed to determine cross-sectional and longitudinal associations between dietary intake and BMD in Japanese postmenopausal women.
Subjects and Methods
Participants and procedure
We targeted 1,310 women aged between 55 and 74 years who resided in the Yokogoshi area in Niigata City. Of these, 674 women agreed to participate in baseline examinations in November 2005, and 600 (89%) were subject to analysis after excluding 13 with a history of bilateral oophorectomy, 7 with corticosteroid use, and 54 undergoing treatment for suspected osteoporosis with bisphosphonates, selective estrogen receptor modulators, active vitamin D analogues, vitamin K, estrogen, or calcitonin. In 2010, 542 of the 674 women agreed to participate in follow-up examinations, and after excluding 44 who met the exclusion criteria, 498 were subject to longitudinal analysis. All subjects provided informed consent. The protocol of this study was approved by the Ethics Committee of Niigata University School of Medicine. Details of the baseline and follow-up examinations were published previously (Nakamura et al. 2008; Kitamura et al. 2013).
Baseline examinations
BMD measurements for the lumbar spine (L2-4), femoral neck, and total hip were performed with dual-energy X-ray absorptiometry (DXA) using a QDR4500a absorptiometer (Hologic Inc., Bedford, MA, USA) by a single trained X-ray technician. The in vivo coefficients of variation (CVs) for the lumbar spine, femoral neck, and total hip were 0.3%, 0.6%, and 2.0%, respectively. The relatively small CV value for the lumber spine is likely due to a small number of measurements. Long-term CVs of the BMD measurements using a quality control phantom were within 1.2%.
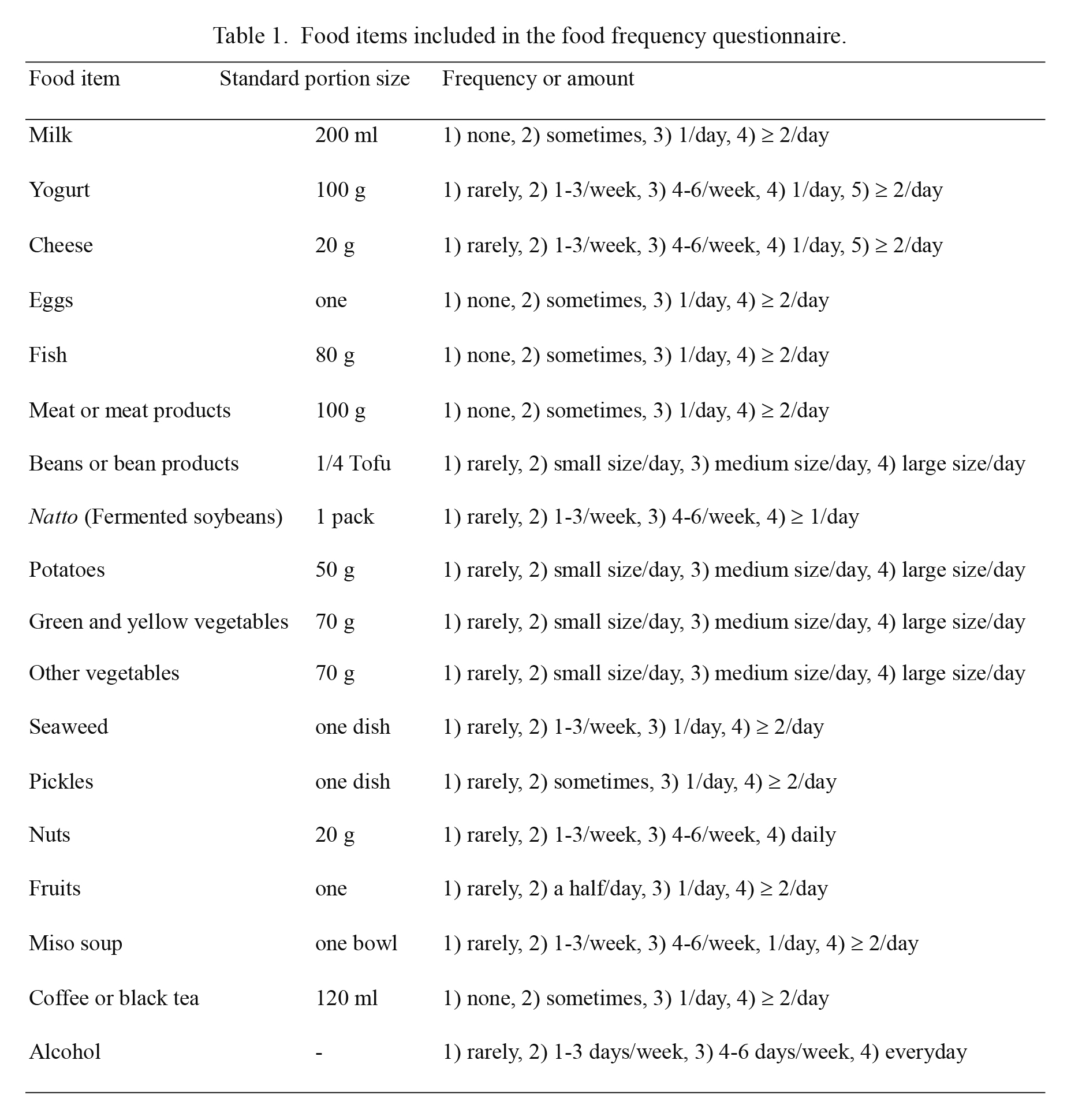
Information on nutrition, lifestyle, and disease history was obtained through interviews. Nutritional intake was assessed with a validated food frequency questionnaire (FFQ) developed to estimate dietary nutrients (Uenishi et al. 2008). Trained nutritionists interviewed subjects and checked each questionnaire item. The correlation coefficients of calcium, vitamin A, vitamin D, vitamin K, energy, proteins, lipids, and carbohydrates between values measured by the FFQ and the conventional 3-day diet record were 0.676, 0.709, 0.403, 0.669, 0.415, 0.319, 0.307, and 0.394, respectively (Uenishi et al. 2008). Food intake was also assessed based on food items included in the FFQ (Table 1). Physical activity levels were evaluated by calculating the ratio of working metabolic rate to resting metabolic rate (referred to as ‘METS index’) based on the 7-day total activity recall of the participants (Sallis et al. 1985).
Body height and weight were measured with light underwear. Body mass index (BMI) was calculated as weight (kg) divided by height squared (m2). Grip strength was measured for both hands with a digital hand dynamometer, and an average value was calculated. Serum 25-hydroxyvitamin D was determined by radioimmunoassay (DiaSorin, Stillwater, MN, USA), with an inter-assay CV value of 9.9% (Nakamura et al. 2008).
Follow-up examinations
In October 2010, measurements of BMD, height, weight, and grip strength were performed in the same manner as in the baseline examinations. In addition, information on disease history and medication during the 5-year period was obtained.
Statistical methods
The paired t-test was used to test the difference of two mean values between baseline and follow-up examinations. Candidate predictor variables were nutrients (energy, proteins, lipids, carbohydrates, vitamin A, vitamin K) and the 18 food items shown in Table 1. Nutrients (energy, proteins, lipids, carbohydrates, vitamin A, and vitamin K) were divided into quartiles in linear regression analyses. Outcomes included baseline BMD of the lumbar spine, femoral neck, and total hip in cross-sectional analyses, and 5-year changes in BMD of the lumbar spine, femoral neck, and total hip in longitudinal analyses. Simple and multiple linear regression analyses were used to determine associations between predictors and outcomes. In multiple linear regression analyses, data were adjusted for years since menopause, BMI, grip strength, 25-hydroxyvitamin D, METs index, and calcium intake in cross-sectional analyses, and for years since menopause, baseline BMD, BMI, grip strength, 25-hydroxyvitamin D, METs index, and calcium intake in longitudinal analyses. Statistical analyses were performed with SPSS software (ver. 21.0, SPSS Inc., Chicago, IL, USA). P < 0.05 was considered statistically significant.
Results
Participant characteristics at baseline and follow-up examinations and their 5-year changes are shown in Table 2. Among these variables, all 5-year changes were negative (i.e., decreased) except for grip strength.
We first explored cross-sectional associations between nutritional and dietary factors and baseline BMD. In simple linear regression analyses, significant nutritional and dietary predictors included lipids, green and yellow vegetables, other vegetables, and coffee/tea for lumbar spine BMD; proteins, lipids, beans or bean products, other vegetables, coffee/tea, and alcohol intake for femoral neck BMD; and proteins, lipids, beans or bean products, green and yellow vegetables, other vegetables, coffee/tea, and alcohol intake for total hip BMD. Table 3 shows significant nutritional and dietary predictors associated with baseline BMD after adjusting for confounders. Coffee/tea consumption was positively associated with lumbar spine and total hip BMD, whereas alcohol intake was positively associated with femoral neck and total hip BMD.
Next, we explored longitudinal associations between nutritional and dietary factors and 5-year changes in BMD. In simple linear regression analyses, significant nutritional and dietary predictors included lipids, vitamin K, and natto (fermented soybeans) for lumbar spine BMD; vitamin A for femoral neck BMD; and meat and coffee/tea for total hip BMD. Table 4 shows significant nutritional and dietary predictors associated with 5-year changes in BMD after adjusting for confounders. Vitamin K and natto were positively associated with lumbar spine BMD. When both vitamin K and natto were included in the multiple linear regression model, only natto was found to be a significant predictor. An inverse association was observed between meat and total hip BMD, but none of the predictors was associated with femoral neck BMD.
Discussion
Nutrients play an important role in bone health (Nieves 2013), and a large body of evidence has shown that calcium and vitamin D are major nutritional factors associated with bone health. However, the effects of other nutrients on bone status have not been fully elucidated (Levis and Lagari 2012). Further understanding of overall dietary and nutritional factors is warranted, because diet is a modifiable risk factor for osteoporosis and represents an easy target for osteoporosis prevention and treatment programs (Levis and Lagari 2012).
In the present study, natto and meat were associated with 5-year changes in BMD in longitudinal analyses, and coffee/tea and alcohol intake were positively associated with BMD in the cross-sectional analyses. Dietary correlates of BMD differed between cross-sectional and longitudinal analyses. This discrepancy may be explained by the fact that current BMD reflects historical dietary habits in cross-sectional analyses, whereas postmenopausal bone loss reflects current dietary habits in longitudinal analyses.
The present study revealed that natto consumption was associated with reduced bone loss for the lumbar spine. The protective effect of natto on bone loss has been reported by a cross-sectional study (Fujita et al. 2012) and a longitudinal study (Ikeda et al. 2006). Fujita et al. (2012) reported that greater natto intake was significantly associated with higher total hip and femoral neck BMD in 1,662 elderly Japanese men. Ikeda et al. (2006) reported that greater natto intake was significantly associated with lower rates of changes in femoral neck and distal radius BMD in 944 Japanese postmenopausal women. Our findings are in line with these reports, except that the associated bone sites differed. Since the reason for this discrepancy is unclear, further evidence should be accumulated in the future.
The protective effect of natto on bone loss can be explained by vitamin K, which includes K1 (phylloquinone) derived from plants and K2 (menaquinones) derived from bacteria and animals (Kamao et al. 2007). Vitamin K is a cofactor of γ-carboxylase, which is essential for converting undercarboxylated osteocalcin to carboxylated osteocalcin (Booth 2001). Natto is rich in vitamin K2, especially menaquinone-7, with one pack of natto (about 40 g) reportedly containing as high as 380 μg of menaquinone-7 on average (Kamao et al. 2007). Several randomized controlled trials conducted in Japan showed that vitamin K2 supplementation reduces the incidence of vertebral and non-vertebral fractures and bone loss (Cockayne et al. 2006). However, recent trials examining Caucasian women did not find beneficial effects of vitamin K2 on BMD (Binkley et al. 2009; Emaus et al. 2010), suggesting that ethnic differences may exist regarding the effects of vitamin K.
Natto, a soy product, is also rich in isoflavones. Isoflavones confer their beneficial effects on bone health through several mechanisms. Some epidemiological studies have suggested a preventive effect of dietary isoflavone intake on osteoporosis and fractures (Weaver et al. 2012; Nieves 2013). As such, isoflavones in natto might have played a role in reducing bone loss.
Meat intake was also associated with increased total hip bone loss. Although total protein intake is unlikely to be a problem for bone health in healthy populations (average protein intake, 66.5 g/day) (Darling et al. 2009), some reports, as well as our results, suggest a potential effect of meat intake on bone loss. Sellmeyer et al. (2001) reported that high animal protein intake, relative to vegetable protein intake, was associated with hip bone loss and high risk of fracture in postmenopausal women. Moreover, Weikert et al. (2005) reported that a high ratio of dietary animal to vegetable protein intake, but not total protein intake, was inversely associated with bone strength estimated by bone ultrasound measurements in adult women. The unfavorable effects of a high animal to vegetable protein intake ratio may be explained by the fact that diets rich in animal foods and low in vegetable foods lead to a high dietary net acid load, which negatively affects calcium balance (Sellmeyer et al. 2001). A report on dietary patterns and BMD in adult Japanese women suggests that low meat intake may have a beneficial effect on radial BMD (Okubo et al. 2006). While it is apparent that sufficient protein intake is important for elderly people, ideal sources of protein for bone health should be explored further.
In the present study, coffee/tea consumption and alcohol intake were associated with higher BMD. Evidence suggests that black tea consumption is associated with higher hip BMD (Devine 2007) and lower risk of osteoporotic (including hip) fractures (Sheng et al. 2014; Myers et al. 2015). The possible protective effects of tea are supposedly attributable to flavonoids (Myers et al. 2015). In contrast, the association between coffee consumption and osteoporosis has been inconsistent. While some reports suggest that coffee consumption is ineffective in improving bone health (Hallström et al. 2006, 2013; Sheng et al. 2014), one recent study demonstrated that higher coffee consumption is associated with higher lumbar spine and hip BMD in an East Asian population (Choi et al. 2016). Consistently, our data also suggest a favorable effect of coffee/tea consumption, with one limitation being that we did not separate tea and coffee. Further studies will be needed to confirm the effects of coffee and tea on osteoporotic fractures.
Evidence suggests that, although heavy drinking is harmful, moderate alcohol intake is associated with higher BMD at various sites in elderly men and women (Berg et al. 2008; Kouda et al. 2011; Sommer et al. 2013). Our data are consistent with this. Future studies to clarify whether moderate drinking protects against osteoporotic fractures are warranted.
The present study has some limitations worth noting. First, given the limited sample size, potential associations might not have been detected due to insufficient statistical power. Second, self-reported information is likely to generate misclassification bias, which might have allowed us to detect potential associations. Finally, our study participants do not represent the entire Japanese population, and selection bias might have influenced the results.
The present study demonstrated that high natto consumption is protective against bone loss in Japanese postmenopausal women, while high meat consumption is not. Furthermore, higher coffee/tea consumption and alcohol intake are associated with BMD. In conclusion, dietary intake is a predictor of bone mass and bone loss in postmenopausal women. Future cohort and intervention studies will be needed to confirm these findings.
Acknowledgments
We thank the staff at Health Promotion Division, Niigata City Yokogoshi Branch Office, for their help in data collection. This study was supported in part by a Grant-in-Aid for Scientific Research (C) No. 17590537 from the Japanese Ministry of Education, Culture, Sports, Science and Technology.
Conflict of Interest
The authors declare no conflict of interest.
References
-
Berg,
K.M.,
Kunins,
H.V.,
Jackson,
J.L.,
Nahvi,
S.,
Chaudhry,
A.,
Harris,
K.A. Jr.,
Malik,
R. &
Arnsten,
J.H.
(2008) Association between alcohol consumption and both osteoporotic fracture and bone density. Am. J. Med., 121, 406-418.
-
Binkley,
N.,
Harke,
J.,
Krueger,
D.,
Engelke,
J.,
Vallarta-Ast,
N.,
Gemar,
D.,
Checovich,
M.,
Chappell,
R. &
Suttie,
J.
(2009) Vitamin K treatment reduces undercarboxylated osteocalcin but does not alter bone turnover, density, or geometry in healthy postmenopausal North American women. J. Bone Miner. Res., 24, 983-991.
-
Booth,
S.L.
(2001) Vitamin K and the skeleton. In Nutritional Aspects of Osteoporosis,
Burckhardt,
P.,
Dawson-Hughes,
B. &
Heaney,
R.P.
Academic Press, London (UK), pp. 273-284.
-
Choi,
E.,
Choi,
K.H.,
Park,
S.M.,
Shin,
D.,
Joh,
H.K. &
Cho,
E.
(2016) The benefit of bone health by drinking coffee among korean postmenopausal women: a cross-sectional analysis of the fourth & fifth Korea National Health and Nutrition Examination Surveys. PLoS One, 11, e0147762.
-
Cockayne,
S.,
Adamson,
J.,
Lanham-New,
S.,
Shearer,
M.J.,
Gilbody,
S. &
Torgerson,
D.J.
(2006) Vitamin K and the prevention of fractures: systematic review and meta-analysis of randomized controlled trials. Arch. Intern. Med., 166, 1256-1261.
-
Darling,
A.L.,
Millward,
D.J.,
Torgerson,
D.J.,
Hewitt,
C.E. &
Lanham-New,
S.A.
(2009) Dietary protein and bone health: a systematic review and meta-analysis. Am. J. Clin. Nutr., 90, 1674-1692.
-
Devine,
A.,
Hodgson,
J.M.,
Dick,
I.M. &
Prince,
R.L.
(2007) Tea drinking is associated with benefits on bone density in older women. Am. J. Clin. Nutr., 86, 1243-1247.
-
Emaus,
N.,
Gjesdal,
C.G.,
Almås,
B.,
Christensen,
M.,
Grimsgaard,
A.S.,
Berntsen,
G.K.,
Salomonsen,
L. &
Fønnebø,
V.
(2010) Vitamin K2 supplementation does not influence bone loss in early menopausal women: a randomised double-blind placebo-controlled trial. Osteoporos. Int., 21, 1731-1740.
-
Fujita,
Y.,
Iki,
M.,
Tamaki,
J.,
Kouda,
K.,
Yura,
A.,
Kadowaki,
E.,
Sato,
Y.,
Moon,
J.S.,
Tomioka,
K.,
Okamoto,
N. &
Kurumatani,
N.
(2012) Association between vitamin K intake from fermented soybeans, natto, and bone mineral density in elderly Japanese men: the Fujiwara-kyo Osteoporosis Risk in Men (FORMEN) study. Osteoporos. Int., 23, 705-714.
-
Hallström,
H.,
Byberg,
L.,
Glynn,
A.,
Lemming,
E.W.,
Wolk,
A. &
Michaëlsson,
K.
(2013) Long-term coffee consumption in relation to fracture risk and bone mineral density in women. Am. J. Epidemiol., 178, 898-909.
-
Hallström,
H.,
Wolk,
A.,
Glynn,
A. &
Michaëlsson,
K.
(2006) Coffee, tea and caffeine consumption in relation to osteoporotic fracture risk in a cohort of Swedish women. Osteoporos. Int., 17, 1055-1064.
-
Ikeda,
Y.,
Iki,
M.,
Morita,
A.,
Kajita,
E.,
Kagamimori,
S.,
Kagawa,
Y. &
Yoneshima,
H.
(2006) Intake of fermented soybeans, natto, is associated with reduced bone loss in postmenopausal women: Japanese Population-Based Osteoporosis (JPOS) Study. J. Nutr., 136, 1323-1328.
-
Iki,
M.
(2014) Epidemiology of osteoporosis and osteoporotic fracture in Japan. Clin. Calcium, 24, 657-664 (in Japanese).
-
Kamao,
M.,
Suhara,
Y.,
Tsugawa,
N.,
Uwano,
M.,
Yamaguchi,
N.,
Uenishi,
K.,
Ishida,
H.,
Sasaki,
S. &
Okano,
T.
(2007) Vitamin K content of foods and dietary vitamin K intake in Japanese young women. J. Nutr. Sci. Vitaminol., 53, 464-470.
-
Kitamura,
K.,
Nakamura,
K.,
Saito,
T.,
Kobayashi,
R.,
Oshiki,
R.,
Nishiwaki,
T.,
Iwasaki,
M. &
Yoshihara,
A.
(2013) High serum 25-hydroxyvitamin D levels do not retard postmenopausal bone loss in Japanese women: the Yokogoshi study. Arch. Osteoporos., 8, 153.
-
Kouda,
K.,
Iki,
M.,
Fujita,
Y.,
Tamaki,
J.,
Yura,
A.,
Kadowaki,
E.,
Sato,
Y.,
Moon,
J.S.,
Morikawa,
M.,
Tomioka,
K.,
Okamoto,
N. &
Kurumatani,
N.
(2011) Alcohol intake and bone status in elderly Japanese men: baseline data from the Fujiwara-kyo osteoporosis risk in men (FORMEN) study. Bone, 49, 275-280.
-
Levis,
S. &
Lagari,
V.S.
(2012) The role of diet in osteoporosis prevention and management. Curr. Osteoporos. Rep., 10, 296-302.
-
Marcus,
R.,
Dempster,
D.W. &
Bouxsein,
M.L.
(2013) The nature of osteoporosis. In Osteoporosis, Volume 1, 4th edition.,
Marcus,
R.,
Feldman,
D.,
Dempster,
D.W.,
Luckey,
M. &
Cauley,
J.A.
Academic Press, Oxford (UK), pp. 21-30.
-
Myers,
G.,
Prince,
R.L.,
Kerr,
D.A.,
Devine,
A.,
Woodman,
R.J.,
Lewis,
J.R. &
Hodgson,
J.M.
(2015) Tea and flavonoid intake predict osteoporotic fracture risk in elderly Australian women: a prospective study. Am. J. Clin. Nutr., 102, 958-965.
-
Nakamura,
K.,
Tsugawa,
N.,
Saito,
T.,
Ishikawa,
M.,
Tsuchiya,
Y.,
Hyodo,
K.,
Maruyama,
K.,
Oshiki,
R.,
Kobayashi,
R.,
Nashimoto,
M.,
Yoshihara,
A.,
Ozaki,
R.,
Okano,
T. &
Yamamoto,
M.
(2008) Vitamin D status, bone mass, and bone metabolism in home-dwelling postmenopausal Japanese women: Yokogoshi Study. Bone, 42, 271-277.
-
Nieves,
J.W.
(2013) Skeletal effects of nutrients and nutraceuticals, beyond calcium and vitamin D. Osteoporos. Int., 24, 771-786.
-
Norman,
A.W. &
Henry,
H.L.
(2015) Hormones, 3rd edition., Academic Press, London (UK), pp. 275-296.
-
Okubo,
H.,
Sasaki,
S.,
Horiguchi,
H.,
Oguma,
E.,
Miyamoto,
K.,
Hosoi,
Y.,
Kim,
M.K. &
Kayama,
F.
(2006) Dietary patterns associated with bone mineral density in premenopausal Japanese farmwomen. Am. J. Clin. Nutr., 83, 1185-1192.
-
Sallis,
J.F.,
Haskell,
W.L.,
Wood,
P.D.,
Fortmann,
S.P.,
Rogers,
T.,
Blair,
S.N.,
Paffenbarger,
R.S. Jr.
(1985) Physical activity assessment methodology in the Five-City Project. Am. J. Epidemiol., 121, 91-106.
-
Sato,
Y.,
Iki,
M.,
Fujita,
Y.,
Tamaki,
J.,
Kouda,
K.,
Yura,
A.,
Moon,
J.S.,
Winzenrieth,
R.,
Iwaki,
H.,
Ishizuka,
R.,
Amano,
N.,
Tomioka,
K.,
Okamoto,
N. &
Kurumatani,
N.
(2015) Greater milk intake is associated with lower bone turnover, higher bone density, and higher bone microarchitecture index in a population of elderly Japanese men with relatively low dietary calcium intake: Fujiwara-kyo Osteoporosis Risk in Men (FORMEN) Study. Osteoporos. Int., 26, 1585-1594.
-
Sellmeyer,
D.E.,
Stone,
K.L.,
Sebastian,
A.,
Cummings,
S.R.;
Study of Osteoporotic Fractures Research Group
(2001) A high ratio of dietary animal to vegetable protein increases the rate of bone loss and the risk of fracture in postmenopausal women. Am. J. Clin. Nutr., 73, 118-122.
-
Sheng,
J.,
Qu,
X.,
Zhang,
X.,
Zhai,
Z.,
Li,
H.,
Liu,
X.,
Li,
H.,
Liu,
G.,
Zhu,
Z.,
Hao,
Y.,
Qin,
A. &
Dai,
K.
(2014) Coffee, tea, and the risk of hip fracture: a meta-analysis. Osteoporos. Int., 25, 141-150.
-
Sommer,
I.,
Erkkilä,
A.T.,
Järvinen,
R.,
Mursu,
J.,
Sirola,
J.,
Jurvelin,
J.S.,
Kröger,
H. &
Tuppurainen,
M.
(2013) Alcohol consumption and bone mineral density in elderly women. Public Health Nutr., 16, 704-712.
-
Uenishi,
K.,
Ishida,
H. &
Nakamura,
K.
(2008) Development of a simple food frequency questionnaire to estimate intakes of calcium and other nutrients for the prevention and management of osteoporosis. J. Nutr. Sci. Vitaminol., 54, 25-29.
-
Weaver,
C.M.,
Alekel,
D.L.,
Ward,
W.E. &
Ronis,
M.J.
(2012) Flavonoid intake and bone health. J. Nutr. Gerontol. Geriatr., 31, 239-253.
-
Weikert,
C.,
Walter,
D.,
Hoffmann,
K.,
Kroke,
A.,
Bergmann,
M.M. &
Boeing,
H.
(2005) The relation between dietary protein, calcium and bone health in women: results from the EPIC-Potsdam cohort. Ann. Nutr. Metab., 49, 312-318.