Abstract
Hepatoma-derived growth factor (HDGF) is a heparin-binding protein possessing mitogenic activity and could be secreted from necrotic cells passively or actively, thereby functioning as a damage-associated molecular pattern (DAMP). The high expression of HDGF in non-small cell lung cancer (NSCLC) tissues is associated with unfavorable prognosis. However, the clinical significance of serum HDGF has not been elucidated in NSCLC yet. In the present study, we compared the serum levels of HDGF in 235 patients with NSCLC (141 adenocarcinoma and 94 squamous cell carcinoma cases) with those in 40 healthy subjects. Moreover, we explored the correlation between serum HDGF levels and clinicopathologic factors or the overall survival rates. We thus found that the serum HDGF levels were significantly higher in NSCLC patients than those in healthy subjects (P < 0.001). Moreover, there was no significant difference in the serum HDGF levels between adenocarcinoma and squamous cell carcinoma. Importantly, the higher serum levels of HDGF were significantly associated with bone metastasis and with lower overall survival rates. Thus, serum HDGF was identified as an independent prognostic factor indicating poor prognosis of NSCLC. Using A549 human lung adenocarcinoma cell line, we demonstrated that an autophagy inhibitor, chloroquine, could inhibit the HDGF secretion, while quercetin, an autophagy inducer derived from a traditional Chinese drug, could facilitate HDGF secretion. In conclusion, high serum levels of HDGF were significantly correlated to bone metastasis and poorer prognosis of NSCLC. We suggest that anti-HDGF therapy is potential to protect NSCLC patients with advanced stages from bone metastasis.
Introduction
Lung cancer is one of the most common and death-cause malignancies worldwide (Siegel et al. 2014). Approximately 220,000 new cases are diagnosed with lung cancer and 150,000 deaths are caused correspondingly every year in the United States. Lung cancers are well identified to originate from the gene-environment interactions. In developing countries such as China, air pollution and haze are more and more serious, leading to the elevation of morbidity of lung cancers. Lung cancers mainly consist of small cell lung cancer (SCLC) and non-small cell lung cancer (NSCLC) with distinct treatment strategies and prognosis. In all the kinds of lung cancers, NSCLC accounts for about 80%, and the 5-year overall survival rate of NSCLC is only 15.9% (Chen et al. 2014). Histologically, NSCLC is further comprised of adenocarcinoma (AC) and squamous cell carcinoma (SCC), accounting for approximately 40% and 25%-30% of all lung cancers, respectively (Zhan et al. 2016).
Hepatoma-derived growth factor (HDGF) is a heparin-binding factor originally purified from the culture supernatants of Huh-7 human hepatoma cell line (Cilley et al. 2000) and its cDNA was cloned from the cDNA library of HuH-7 cells (Nakamura et al. 1989, 1994), but its expression is not restricted only in liver or hepatoma. HDGF was reported to be expressed widespread and played important roles in the development, repair and remodeling of various tissues and organs (Oliver and Al-Awqati 1998; Lepourcelet et al. 2005; Narron et al. 2006). The aberrant expression of HDGF was found in many kinds of malignancies, and HDGF in tumors was involved in tumor cell growth, angiogenesis and invasion (Lepourcelet et al. 2005). Ectopic HDGF expression in tumor tissues was also reported to be implicated in prognosis of patients and the progression of tumor including hepatocellular carcinoma, gastric carcinoma as well as colorectal stromal tumors (Yamamoto et al. 2006; Yoshida et al. 2006; Hu et al. 2009). Moreover, HDGF is also a member of damage-associated molecular patterns (DAMPs), functioning like the famous DAMP molecule, high mobility group box 1 (HMGB1) (Xu et al. 2015). As DAMPs, HDGF or HMGB1 could be released outside passively when cells are injured, and enhance the immune responses during tissue injury. Moreover, HDGF could be secreted out of cells and into circulation system actively without N-terminal signaling peptide. Intriguingly, some cancer cells are reported to secret HDGF actively such as hepatoma cells and glioblastoma stem-like cells, indicating that HDGF could be released in both passive or active ways (Shih et al. 2012; Thirant et al. 2012). The serum HDGF in patients with lung cancer is also detectable with enzyme linked immunosorbent assay (ELISA) method according to previous study (Zhang et al. 2010). However, there is no in-depth report on the clinical and prognostic significance of the serum HDGF for patients with lung cancer yet.
In our study, we collected the blood samples from 235 patients with NSCLC and 40 healthy subjects, and compared their serum HDGF levels. We further classified the NSCLC patients into high-HDGF and low-HDGF groups, and subsequently analyzed the correlations between HDGF level and clinicopathological factors. With univariate and multivariate analyses, we revealed the prognostic value of serum HDGF. Moreover, using A549 human lung adenocarcinoma cells, we explored the effects on autophagy and HDGF secretion of chloroquine, an inhibitor of autophagy, and quercetin, an inducer of autophagy, derived from a traditional Chinese drug.
Materials and Methods
Patients and follow-ups
A total of 325 patients were diagnosed as NSCLC with stage Ⅲ-Ⅳ from 2006-2016 in Yidu Central Hospital or Shandong Academy of Medical Sciences. The patients who lost opportunity or refused operation, and underwent systemic chemotherapy were enrolled into our cohort, consisting of 235 patients. The validation cohort included 141 cases of AC and 94 cases of SCC. The venous blood samples from these patients were extracted before receiving any chemotherapy. Serum HDGF was detected using ELISA method. As the control, serum HDGF levels of 40 healthy volunteers were also tested. This study was approved by the Ethics Committee of Yidu Central Hospital and the Ethics Committee of Shandong Academy of Medical Sciences. All blood samples were obtained with prior written informed consent of the patients as well as the healthy subjects. The pathologic tumor-node-metastasis (pTNM) classification was based on the 7th American Joint Committee on Cancer/ Union for International Cancer Control (AJCC/UICC) TNM stage system (Xu et al. 2017; Liu et al. 2017).
Cells and reagents
NSCLC cell line A549 was a widely-used cell model as a human lung adenocarcinoma epithelial cell line. A549 cells were obtained from the Institute of Biochemistry and Cell Biology of the Chinese Academy of Sciences (Shanghai, China) and cultured in RPMI-1640 medium, supplemented with 10% fetal bovine serum (FBS), 100 U/ml penicillin and 100 mg/ml streptomycin in 5% CO2 resuscitation (Xu et al. 2014). RPMI-1640, penicillin, streptomycin, FBS and trypsin were all purchased from Gibco Company. All other reagents without special instruction were purchased from Sigma-Aldrich Company.
Detection of HDGF by ELISA
The levels of HDGF in serum samples or cell culture media were detected by HDGF ELISA kit (Antibodies-online Company) according to the manual and previous studies (Zhang et al. 2010; Guo et al. 2015). Both serum and medium samples were prepared by centrifuge at 2,000 rpm and filtering with 0.22 μm filter. Standard or samples (100 μL) were added to each well and incubated for 2 hours. After that, Detection Reagent A (100 μL) was added and incubated for 1 hour. The wells were subsequently washed 3 times with phosphate buffer saline (PBS), and the Substrate Solution was added and incubated for another 15 minutes. Finally, we added 50 μL stop solution and the optical density (OD) at 450 nm was detected. Our cohort was defined as high-HDGF and low HDGF groups according to the cut-off, which was calculated by the receiver operating characteristic (ROC) curve and set as the point with the highest sensitivity plus specificity according to previous studies (Liu et al. 2016).
To detect the HDGF level after stimulation with quercetin or chloroquine, the A549 cells were firstly incubated with 50 μM quercetin or 60 μM chloroquine for 24 hours, while control cells were treated with DMSO. After stimulation, the cell medium samples were prepared by centrifuge at 2,000 rpm and the supernatant was filtered with 0.22 μm filter. The HDGF level in different treatment group was detected with ELISA as described above.
Autophagy detection
The ratio of LC3-II/LC3-I was selected as the parameter to evaluate the autophagy extent. The detection of LC3-I or LC3-II was achieved by Western blotting analysis. Briefly, cells after stimulation of quercetin or chloroquine were lysed with lysis buffer. The cell lysis was centrifuged at 11,000 rpm at 4°C for 20 minutes, and the supernatant was collected. Total amount of 10 μg protein was loaded to a SDS-PAGE gel, then transferred to PVDF membrane (PALL Company, NY, USA), and incubated with primary antibody of LC3 (Santa Cruz Biotechnology, CA, USA) overnight in 4°C. Then, the membrane was washed with Tris-buffered saline (TBS) for 3 times, and was incubated in secondary antibody labeled with horseradish peroxidase for 2 hours at 37°C. The blotted proteins were visualized by ECL (Millipore Company, MA, USA).
Statistical analysis
SPSS17.0 software was used for the analysis of all the data. The comparisons between healthy subjects and NSCLC patients, between AC and SCC, were all analyzed by the Student's t-test. The correlation between the HDGF level and clinicopathologic features was analyzed with Chi-square test. Overall survival curve was plotted by the Kaplan-Meier method, and the difference among the subgroups was compared with the log-rank test. Independent prognostic factors were identified by using the Cox proportional hazards regression model. P < 0.05 was considered as statistically significant.
Results
Information of the cohort
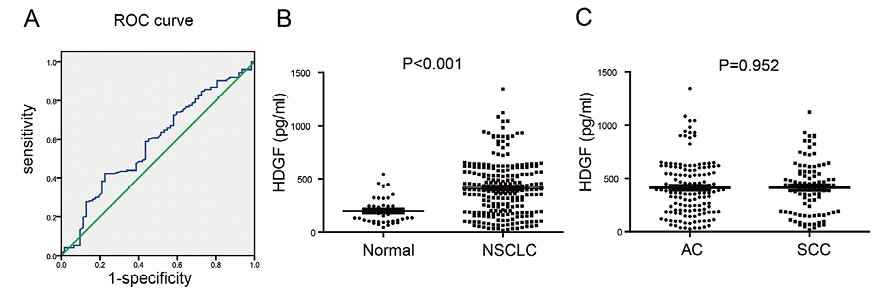
Our cohort included 235 cases of NSCLCs, consisting of 141 ACs and 94 SCCs (Table 1). There were 129 male patients and 106 female patients in our cohort, with an average age as 63.2 years old. All the patients were in an advanced TNM stage of NSCLC and could not undergo the radical surgery, comprising of 87 cases with stage IIIA, 40 cases with stage IIIB and 108 cases with stage IV. The levels of serum HDGF were detected with ELISA method, ranging from 18 to 1,344 pg/ml. The cohort was divided into high serum HDGF and low serum HDGF group according to the cut-off of HDGF confirmed by ROC curve, which was 385 pg/ml in our study (Fig. 1A). The high serum HDGF and low serum HDGF groups accounted for 47.68% and 52.32% of the total cohort, respectively. Compared with healthy subjects, NSCLC patients had much higher serum HDGF level (P < 0.001) (Fig. 1B). However, there was no significant difference of the serum HDGF levels between AC and SCC patients (P = 0.952) (Fig. 1C).

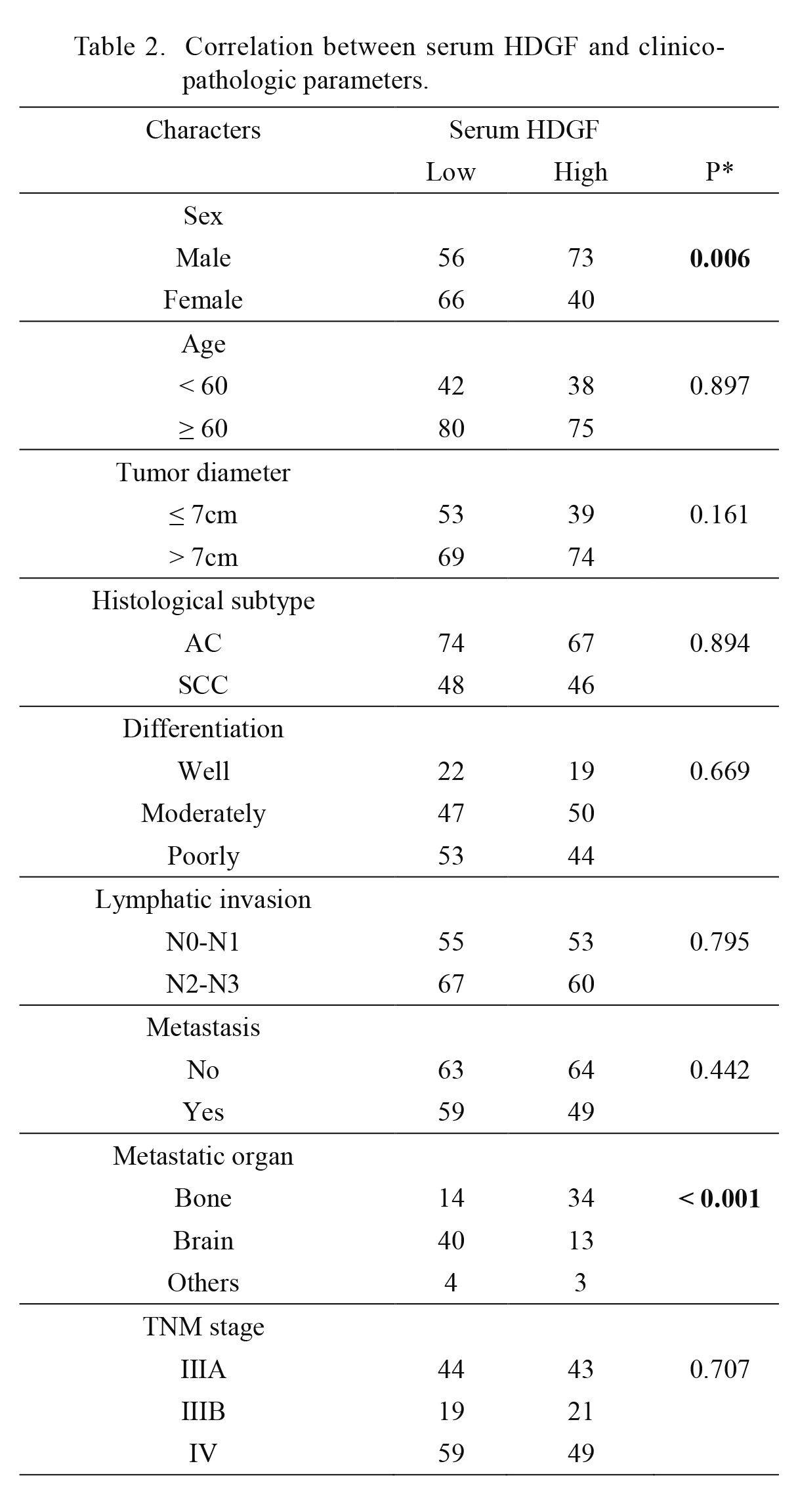
Chi-square test was used to analyze the correlation between the serum levels of HDGF and the clinicopathologic factors (Table 2). It was interesting to note that in the patients with high serum HDGF, their bones seemed more vulnerable to metastasis compared with brain (P < 0.001). Moreover, male patients seemed to have higher serum HDGF level than female patients (P = 0.006), indicating the possibility that HDGF may be affected by sex hormones.
Prognostic value of serum HDGF and clinicopathologic factors
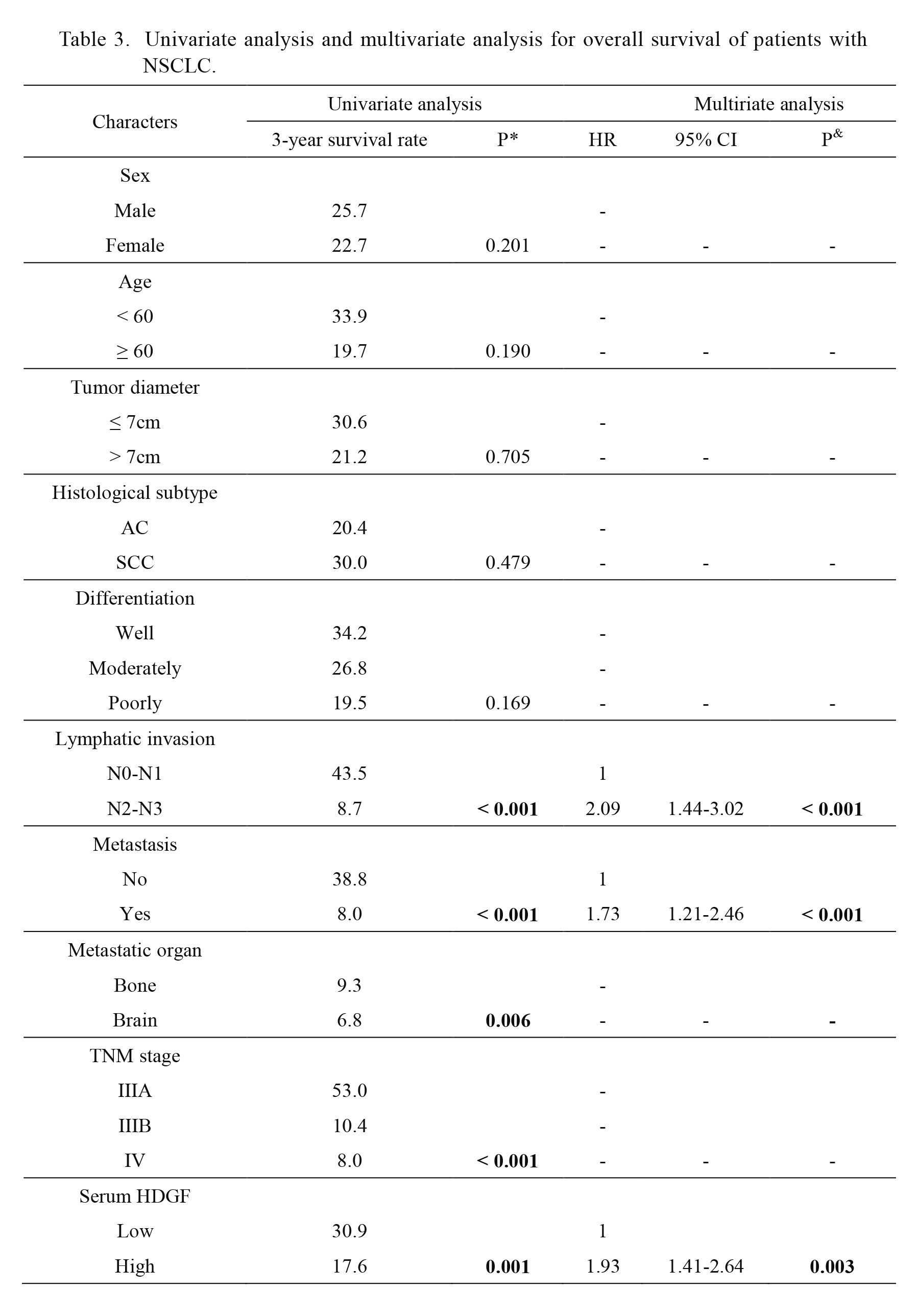
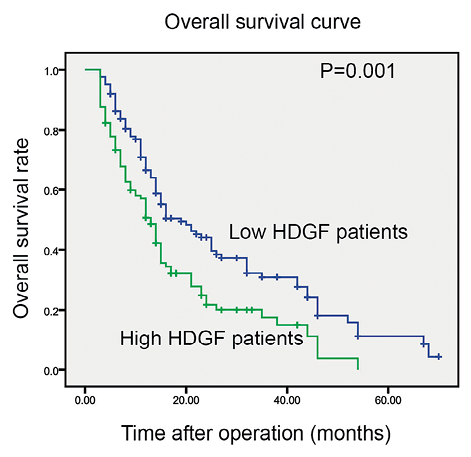
The prognostic significance of serum HDGF and clinicopathologic factors was evaluated with univariate analysis (Table 3). The survival curve was displayed by Kaplan-Meier method and statistical significance between low and high HDGF level was analyzed with log-rank test (Fig. 2). In our experiments, high level of serum HDGF was significantly associated with lower survival rate (P = 0.001), indicating that patients with high circulating HDGF had poorer prognosis. Additionally, positive lymphatic invasion (P < 0.001), metastasis (P < 0.001) and advanced TNM stage (P < 0.001) could also predict the unfavorable prognosis of NSCLC. Compared with metastasis in bones, patients with metastasis in brain usually showed poorer survival rate (P = 0.006).
Furthermore, multivariate analysis was performed to screen the independent prognostic factors with the Cox-regression hazard model (Table 3). All the prognostic factors identified in univariate analysis were enrolled into the Cox-regression model to confirm the independent prognostic factor. TNM stage was excluded due to its natural interaction with N stage and M stage. In the multivariate analysis, high level of HDGF was identified as an independent prognostic factor predicting unfavorable prognosis of NSCLC (P = 0.003, HR = 1.93, 95% CI = 1.41-2.64), which suggested that high serum HDGF alone could predict a poorer prognosis of NSCLC patients. Positive lymphatic invasion (P < 0.001, HR = 2.09, 95% CI = 1.44-3.02) and metastasis (P < 0.001, HR = 11.73, 95% CI = 1.21-2.46) were also confirmed as independent prognostic factors in our cohort.
Effect of chloroquine and quercetin on HDGF secretion
As a member of DAMP, HDGF lacks the signal peptide leading secretion, and is usually considered to be secreted in a non-canonical way, which is partially related to autophagy. In our study, we investigated the effect of the extract of a Chinese traditional drug-quercetin on HDGF secretion of NSCLC cells, with the well-acknowledged autophagy inhibitor chloroquine as the control. Firstly, the dose-effect of chloroquine and quercetin on autophagy was detected. The increasing concentrations of chloroquine (0, 25, 50, and 100 μM) were used to incubate lung cancer cell line A549 for 24 hours, and LC3-II/LC3-I detected by Western blotting analysis was applied to evaluate the extent of autophagy (Fig. 3A). A549 cells were incubated in EBSS medium for 2 hours for autophagy indication after incubation with different doses of chloroquine (0, 25, 50, and 100 μM) for 24 hours. The ratio of LC3-II/LC3-I, which represents the level of autophagy, decreased along with the increasing dose of chloroquine (Fig. 3A). Chloroquine at the dose of 50 μM could achieve the most inhibitory effect on EBSS-induced autophagy (Fig. 3B). Quercetin, an extract from Chinese traditional medicine, was considered as an inducer of autophagy in previous study (He et al. 2017). Here we also detected its effect on the autophagy of A549. Quercetin at different concentration was used to incubate A549 cells for 24 hours and the ratio of LC3-II/LC3-I was detected after that (Fig. 3C). Quercetin at concentration of 50 or 100 μM could promote autophagy of A549 more significantly than 25 μM concentration (Fig. 3D).
The effects of chloroquine and quercetin on HDGF secretion of A549 cells were tested. The levels of HDGF in the cell medium were detected with ELISA method before and after the incubation of chloroquine and quercetin, and the different value of medium HDGF was set as the secreted HDGF. In our experiment, chloroquine could decrease the HDGF secretion substantially (Fig. 3E) while quercetin remarkably elevated the HDGF secretion (Fig. 3F), which was corresponding to their effect on autophagy. These results indicated that HDGF secretion from A549 was associated with the autophagy level.
Discussion
Injured or dead cells can release a plethora of mediators, termed as damage-associated molecular patterns (DAMPs), including High Mobility Group Box 1 (HMGB1), S100 proteins, hyaluronan, heat-shock proteins, adenosine triphosphate (ATP), and calreticulin, which are retained inside the cell in the healthy state (Hernandez et al. 2016). DAMPs are potent triggers of sterile inflammation, which could facilitate tumor progression such as angiogenesis. HDGF is mainly released from necrotic cells, as well as cells with some specific forms of programmed cell death such as necroptosis and immunogenic cell death (Krysko et al. 2012). It is interesting that HDGF could also be secreted out from living cells, similar with some other DAMPs such as IL-1β. HDGF lacks a classical signal peptide and the secretion mechanism of HDGF is still not well known. Thakar et al. (2010) have demonstrated that the secretion of HDGF is regulated by its N-terminal processing. Autophagy, also called secretory autophagy, was demonstrated to be essential in some kinds of unconventional secretion (Ponpuak et al. 2015). Some other DAMPs, including HMGB1 and IL-1β, could be secreted in this autophagy-based non-conventional secretory pathway (Thorburn et al. 2009; Dupont et al. 2011). In our experiments, we demonstrated that the well-defined autophagy inhibitor chloroquine could decrease the HDGF level of cell medium, while one autophagy-inducer quercetin elevated the HDGF level, indicating HDGF secretion from NSCLC cells was also influenced by autophagy, which certainly needs more direct evidence and more experiments to prove.
As a member of DAMP, HDGF could be released from dead cells, and that is why we collected the blood samples before any chemotherapy. However, patients with NSCLC still had significantly higher HDGF than healthy subjects. This may be resulted from some dead tumor cells or due to the secretion of HDGF. Circulating HDGF could trigger immune-response and promote angiogenesis, and we also proved that serum HDGF was significantly associated with bone metastasis. In our study, chloroquine was shown to inhibit HDGF secretion, indicating it as a potential drug in chemotherapy. In fact, another report supported that chloroquine is a prospective adjunct in tumor therapy and is effective in eliminating chemotherapy-resistant cancer cells (Geng et al. 2010).
In previous studies, overexpression of HDGF was shown to predict poorer prognosis of stage I NSCLC (Ren et al. 2004), and HDGF down-regulation could inhibit anchorage-independent growth and invasion of NSCLC cells (Zhang et al. 2006). Accumulating evidence suggested HDGF was a potential therapeutic target in lung cancer treatment. Drugs or other agents blocking the HDGF function may help reduce lung cancer progression and improve patients’ survival time. HDGF-neutralizing antibody was used in heterotransplant models and demonstrated to prevent relapse of NSCLC by repressing cancer stem cells (Zhao et al. 2013). but there is no available small-molecular inhibitor of HDGF yet. The exploration of HDGF signaling inhibitors or other blockers should be more focused. Moreover, some miRNAs targeted on HDGF, such as miR16, were also demonstrated to regulate the growth in NSCLC cells. All the emerging evidence indicated anti-HDGF therapy as a promising direction in the field of lung cancer treatment.
Conflict of Interest
We declare no conflict of interest.
References
-
Chen,
Z.,
Fillmore,
C.M.,
Hammerman,
P.S.,
Kim,
C.F. &
Wong,
K.K.
(2014) Non-small-cell lung cancers: a heterogeneous set of diseases. Nat. Rev. Cancer, 14, 535-546.
-
Cilley,
R.E.,
Zgleszewski,
S.E. &
Chinoy,
M.R.
(2000) Fetal lung development: airway pressure enhances the expression of developmental genes. J. Pediatr. Surg., 35, 113-118; discussion 119.
-
Dupont,
N.,
Jiang,
S.,
Pilli,
M.,
Ornatowski,
W.,
Bhattacharya,
D. &
Deretic,
V.
(2011) Autophagy-based unconventional secretory pathway for extracellular delivery of IL-1β. EMBO J., 30, 4701-4711.
-
Geng,
Y.,
Kohli,
L.,
Klocke,
B.J. &
Roth,
K.A.
(2010) Chloroquine-induced autophagic vacuole accumulation and cell death in glioma cells is p53 independent. Neuro Oncol., 12, 473-481.
-
Guo,
S.,
Liu,
H.D.,
Liu,
Y.F.,
Liu,
L.,
Sun,
Q. &
Cui,
X.J.
(2015) Hepatoma-derived growth factor: a novel prognostic biomarker in intrahepatic cholangiocarcinoma. Tumour Biol., 36, 353-364.
-
He,
Y.,
Cao,
X.,
Guo,
P.,
Li,
X.,
Shang,
H.,
Liu,
J.,
Xie,
M.,
Xu,
Y. &
Liu,
X.
(2017) Quercetin induces autophagy via FOXO1-dependent pathways and autophagy suppression enhances quercetin-induced apoptosis in PASMCs in hypoxia. Free Radic. Biol. Med., 103, 165-176.
-
Hernandez,
C.,
Huebener,
P. &
Schwabe,
R.F.
(2016) Damage-associated molecular patterns in cancer: a double-edged sword. Oncogene, 35, 5931-5941.
-
Hu,
T.H.,
Lin,
J.W.,
Chen,
H.H.,
Liu,
L.F.,
Chuah,
S.K. &
Tai,
M.H.
(2009) The expression and prognostic role of hepatoma-derived growth factor in colorectal stromal tumors. Dis. Colon Rectum, 52, 319-326.
-
Krysko,
D.V.,
Garg,
A.D.,
Kaczmarek,
A.,
Krysko,
O.,
Agostinis,
P. &
Vandenabeele,
P.
(2012) Immunogenic cell death and DAMPs in cancer therapy. Nat. Rev. Cancer, 12, 860-875.
-
Lepourcelet,
M.,
Tou,
L.,
Cai,
L.,
Sawada,
J.,
Lazar,
A.J.,
Glickman,
J.N.,
Williamson,
J.A.,
Everett,
A.D.,
Redston,
M.,
Fox,
E.A.,
Nakatani,
Y. &
Shivdasani,
R.A.
(2005) Insights into developmental mechanisms and cancers in the mammalian intestine derived from serial analysis of gene expression and study of the hepatoma-derived growth factor (HDGF). Development, 132, 415-427.
-
Liu,
H.,
Xu,
Y.,
Zhang,
Q.,
Yang,
H.,
Shi,
W.,
Liu,
Z.,
Li,
K.,
Gong,
Z.,
Ning,
S.,
Li,
S. &
Chen,
Y.
(2017) Prognostic significance of TBL1XR1 in predicting liver metastasis for early stage colorectal cancer. Surg. Oncol., 26, 13-20.
-
Liu,
H.,
Zhang,
Q.,
Li,
K.,
Gong,
Z.,
Liu,
Z.,
Xu,
Y.,
Swaney,
M.H.,
Xiao,
K. &
Chen,
Y.
(2016) Prognostic significance of USP33 in advanced colorectal cancer patients: new insights into β-arrestin-dependent ERK signaling. Oncotarget, 7, 81223-81240.
-
Nakamura,
H.,
Izumoto,
Y.,
Kambe,
H.,
Kuroda,
T.,
Mori,
T.,
Kawamura,
K.,
Yamamoto,
H. &
Kishimoto,
T.
(1994) Molecular cloning of complementary DNA for a novel human hepatoma-derived growth factor. Its homology with high mobility group-1 protein. J. Biol. Chem., 269, 25143-25149.
-
Nakamura,
H.,
Kambe,
H.,
Egawa,
T.,
Kimura,
Y.,
Ito,
H.,
Hayashi,
E.,
Yamamoto,
H.,
Sato,
J. &
Kishimoto,
S.
(1989) Partial purification and characterization of human hepatoma-derived growth factor. Clin. Chim. Acta, 183, 273-284.
-
Narron,
J.V.,
Stoops,
T.D.,
Barringhaus,
K.,
Matsumura,
M. &
Everett,
A.D.
(2006) Hepatoma-derived growth factor is expressed after vascular injury in the rat and stimulates smooth muscle cell migration. Pediatr. Res., 59, 778-783.
-
Oliver,
J.A. &
Al-Awqati,
Q.
(1998) An endothelial growth factor involved in rat renal development. J. Clin. Invest., 102, 1208-1219.
-
Ponpuak,
M.,
Mandell,
M.A.,
Kimura,
T.,
Chauhan,
S.,
Cleyrat,
C. &
Deretic,
V.
(2015) Secretory autophagy. Curr. Opin. Cell Biol., 35, 106-116.
-
Ren,
H.,
Tang,
X.,
Lee,
J.J.,
Feng,
L.,
Everett,
A.D.,
Hong,
W.K.,
Khuri,
F.R. &
Mao,
L.
(2004) Expression of hepatoma-derived growth factor is a strong prognostic predictor for patients with early-stage non-small-cell lung cancer. J. Clin. Oncol., 22, 3230-3237.
-
Shih,
T.C.,
Tien,
Y.J.,
Wen,
C.J.,
Yeh,
T.S.,
Yu,
M.C.,
Huang,
C.H.,
Lee,
Y.S.,
Yen,
T.C. &
Hsieh,
S.Y.
(2012) MicroRNA-214 downregulation contributes to tumor angiogenesis by inducing secretion of the hepatoma-derived growth factor in human hepatoma. J. Hepatol., 57, 584-591.
-
Siegel,
R.,
Ma,
J.,
Zou,
Z. &
Jemal,
A.
(2014) Cancer statistics, 2014. CA Cancer J. Clin., 64, 9-29.
-
Thakar,
K.,
Krocher,
T.,
Savant,
S.,
Gollnast,
D.,
Kelm,
S. &
Dietz,
F.
(2010) Secretion of hepatoma-derived growth factor is regulated by N-terminal processing. J. Biol. Chem., 391, 1401-1410.
-
Thirant,
C.,
Galan-Moya,
E.M.,
Dubois,
L.G.,
Pinte,
S.,
Chafey,
P.,
Broussard,
C.,
Varlet,
P.,
Devaux,
B.,
Soncin,
F.,
Gavard,
J.,
Junier,
M.P. &
Chneiweiss,
H.
(2012) Differential proteomic analysis of human glioblastoma and neural stem cells reveals HDGF as a novel angiogenic secreted factor. Stem Cells, 30, 845-853.
-
Thorburn,
J.,
Horita,
H.,
Redzic,
J.,
Hansen,
K.,
Frankel,
A.E. &
Thorburn,
A.
(2009) Autophagy regulates selective HMGB1 release in tumor cells that are destined to die. Cell Death Differ., 16, 175-183.
-
Xu,
Y.,
Yang,
X.,
Li,
Z.,
Li,
S.,
Guo,
S.,
Ismail,
S.,
Liu,
H.,
Huang,
Z.,
Zhang,
Z.,
Chen,
Y. &
Sun,
Q.
(2017) Sprouty2 correlates with favorable prognosis of gastric adenocarcinoma via suppressing FGFR2-induced ERK phosphorylation and cancer progression. Oncotarget, 8, 4888-4900.
-
Xu,
Y.F.,
Ge,
F.J.,
Han,
B.,
Yang,
X.Q.,
Su,
H.,
Zhao,
A.C.,
Zhao,
M.H.,
Yang,
Y.B. &
Yang,
J.
(2015) High-mobility group box 1 expression and lymph node metastasis in intrahepatic cholangiocarcinoma. World J. Gastroenterol., 21, 3256-3265.
-
Xu,
Y.F.,
Yang,
X.Q.,
Lu,
X.F.,
Guo,
S.,
Liu,
Y.,
Iqbal,
M.,
Ning,
S.L.,
Yang,
H.,
Suo,
N. &
Chen,
Y.X.
(2014) Fibroblast growth factor receptor 4 promotes progression and correlates to poor prognosis in cholangiocarcinoma. Biochem. Biophys. Res. Commun., 446, 54-60.
-
Yamamoto,
S.,
Tomita,
Y.,
Hoshida,
Y.,
Takiguchi,
S.,
Fujiwara,
Y.,
Yasuda,
T.,
Doki,
Y.,
Yoshida,
K.,
Aozasa,
K.,
Nakamura,
H. &
Monden,
M.
(2006) Expression of hepatoma-derived growth factor is correlated with lymph node metastasis and prognosis of gastric carcinoma. Clin. Cancer Res., 12, 117-122.
-
Yoshida,
K.,
Tomita,
Y.,
Okuda,
Y.,
Yamamoto,
S.,
Enomoto,
H.,
Uyama,
H.,
Ito,
H.,
Hoshida,
Y.,
Aozasa,
K.,
Nagano,
H.,
Sakon,
M.,
Kawase,
I.,
Monden,
M. &
Nakamura,
H.
(2006) Hepatoma-derived growth factor is a novel prognostic factor for hepatocellular carcinoma. Ann. Surg. Oncol., 13, 159-167.
-
Zhan,
P.,
Lv,
X.J.,
Ji,
Y.N.,
Xie,
H. &
Yu,
L.K.
(2016) Increased lysyl oxidase-like 2 associates with a poor prognosis in non-small cell lung cancer. Clin. Respir. J., doi: 10.1111/crj.12584. [Epub ahead of print].
-
Zhang,
A.,
Long,
W.,
Guo,
Z.,
Liu,
G.,
Hu,
Z.,
Huang,
Y.,
Li,
Y.,
Grabinski,
T.M.,
Yang,
J.,
Zhao,
P.X.,
Everett,
A.D.,
Zhang,
Y. &
Cao,
B.B.
(2010) Development and clinical evaluation of a multi-purpose mAb and a sandwich ELISA test for hepatoma-derived growth factor in lung cancer patients. J. Immunol. Methods, 355, 61-67.
-
Zhang,
J.,
Ren,
H.,
Yuan,
P.,
Lang,
W.,
Zhang,
L. &
Mao,
L.
(2006) Down-regulation of hepatoma-derived growth factor inhibits anchorage-independent growth and invasion of non-small cell lung cancer cells. Cancer Res., 66, 18-23.
-
Zhao,
J.,
Ma,
M.Z.,
Ren,
H.,
Liu,
Z.,
Edelman,
M.J.,
Pan,
H. &
Mao,
L.
(2013) Anti-HDGF targets cancer and cancer stromal stem cells resistant to chemotherapy. Clin. Cancer Res., 19, 3567-3576.