Abstract
Up to 8% of pregnant women suffer from preeclampsia (PE), a deadly disease characterized by high blood pressure (BP), blood vessel damage, called endotheliosis (vascular endothelial swelling with narrowing of capillary lumen), and high levels of protein in the urine. PE is often associated with premature delivery, which is a risk factor of cardiovascular and metabolic diseases among the offspring. Accordingly, establishing drug treatments of PE is in immediate needs. Currently, many of anti-hypertensive drugs cause malformation of the fetuses and are contraindicated for pregnant women. Anti-hypertensive drugs that are allowed to be used for treating pregnant women could lower BP of the mothers and reduce the risk of maternal death due to cardiovascular diseases such as cerebral hemorrhage. However, these anti-hypertensives do not improve endotheliosis and proteinuria. In fact, they reduce blood supply to the placentae and fetuses, which could lead to fetal growth restriction (FGR) and fetal and neonatal death. Until now, the only treatment for preeclamptic women has been delivery of the baby and placenta. Using three mechanistically different mouse models of PE, we have found that vitamin B3 nicotinamide (Nam) is the first safe drug that alleviates PE, and that Nam also alleviates or prevents miscarriage, prolongs pregnancy period, and improves the growth of the fetuses in mice with PE. Importantly, Nam has been used for pregnant and nursing women who have difficulty in taking sufficient meal. Nam could help treat or prevent PE and FGR associated with PE, if the treatment works in humans.
Introduction
Preeclampsia (PE) is a disease in pregnant women, characterized by high blood pressure (BP) and proteinuria (Levine et al. 2004). PE often rapidly deteriorates and causes maternal death due largely to cardiovascular diseases. It sometimes also leads to fetal growth restriction (FGR) and fetal or neonatal death. The number of PE patients is increasing with increasing age of child bearing women. There are about 20,000 pregnant women who develop PE in a year in Japan. It is estimated that about 4,000,000 women annually develop PE in the world. However, the fundamental treatment of PE is not established. PE is a risk factor of future cardiovascular diseases. PE is often associated with premature delivery, which is a high risk in the offspring of neurodevelopmental impairment (Sutton and Darmstadt 2013) and of cardiovascular and metabolic diseases (Nuyt et al. 2017). Accordingly, establishing drug treatments of PE is in immediate needs.
The Problem in Treating PE
Other than high BP and proteinuria, endotheliosis, swelling of endothelial cells and narrowing of capillary lumen, is also a characteristic feature of PE (Fig. 1). The problem in treating PE is that there is no effective drug treatment to save both mothers and babies. Different kinds of anti-hypertensives are clinically used. However, many of them cause malformation of the fetuses and cannot be used for pregnant women. Anti-hypertensives we can use for pregnant women can save PE mothers from cardiovascular diseases. However, because they do not improve endotheliosis, lowering maternal BP reduces placental and fetal blood flow, and leads to poor prognosis of the baby (Kingman et al. 2009; von Dadelszen et al. 2000). Until now the only way to solve this problem is to induce delivery of the premature baby and placenta, which secretes anti-angiogenic factors. Because delivery of premature baby could affect neuropsychological development, and is the risk of developing cardiovascular diseases and the metabolic syndrome in the future, it is extremely important to establish drug treatment of PE that not only reduces maternal BP, but also prolongs pregnancy period, and improves fetal growth that secures fetal/neonatal health.

Pathogenesis of PE
To develop novel treatments, it is necessary to understand the pathogenesis of PE. The most widely accepted understanding of the pathogenic mechanism of PE is that PE is primarily the consequences of an imbalance between pro-angiogenic growth factors that keep vascular health (such as vascular endothelial growth factor, VEGF), and anti-angiogenic factors, such as the soluble form of VEGF receptor-1 (sVEGFR-1, commonly referred to as sFlt-1) (Fig. 2) (Levine et al. 2004). sFlt-1 is a splice variant of VEGFR-1, which lacks transmembrane domain and cytosolic domain, and is secreted from trophoblasts of the placenta into the circulation. sFlt-1 has ligand-binding domain, traps VEGF, and works as its antagonist. Both the hypertension and the proteinuria of PE are caused by abnormally high amounts of anti-angiogenic factors derived from the placenta. FGR is often associated with PE, and is a consequence of reduced placental blood flow by anti-angiogenic factors and/or to impaired development of the placenta.
The decrease in the levels of VEGF activates the endothelin system. We have previously shown that the renal levels of endothelin-1 (ET-1), the most powerful naturally occurring pro-hypertensive peptide, and of the endothelin type A receptor (ETAR) are increased by excessive sFlt-1 (Murphy et al. 2010; Li et al. 2012). Antagonists of ETAR greatly ameliorate the PE-like condition that develops in the kidneys with experimentally induced excessive sFlt-1 (Murphy et al. 2010; Li et al. 2012). Unfortunately, mice lacking ET-1 and ETAR are lethal, and ETAR antagonists are teratogenic and contraindicated for use in pregnant women (Kingman et al. 2009). Consequently, we cannot use this class of drugs to treat PE.
Expected effect of Vitamin B3 Nicotinamide on PE
Although inhibiting ETAR is not suitable for pregnant women, inhibiting some of ET-1 signaling could help treat PE without adverse effects. Nam does not cause malformation of the fetuses, and inhibits vasoconstriction by ET-1 through inhibiting adenosine diphosphate (ADP) ribosyl cyclase, and reducing its product cyclic ADP ribose and Ca2+ mobilization (Fig. 3) (Thai and Arendshorst 2008; Arendshorst and Thai 2009).
Moreover, nicotinic acid increases heme oxygenase-1 (HO-1) expression, which sequentially increases VEGF (Dulak et al. 2004), increases endothelial nitric oxide synthase (eNOS) expression and activity, and decreases BP (Fig. 4). Vitamin B3 nicotinamide (Nam) likely has the similar effects on HO-1 expression and BP. HO degrades heme and produces carbon monoxide and biliverdin/bilirubin. Nicotinamide adenine dinucleotide phosphate (NADPH) is required for this reaction. Nam becomes nicotinamide adenine dinucleotide (NAD+), and NAD+ kinase in cytosol and mitochondrion changes NAD+ to NADP+. NADP+ becomes NADPH by the transfer of reducing equivalent from NADH to NADP+. Because oxidative stress and inflammation causes FGR, Nam is a promising drug to ameliorate PE, premature delivery, and FGR by its anti-oxidative property.
Effects of Nam on PE in Mouse Models
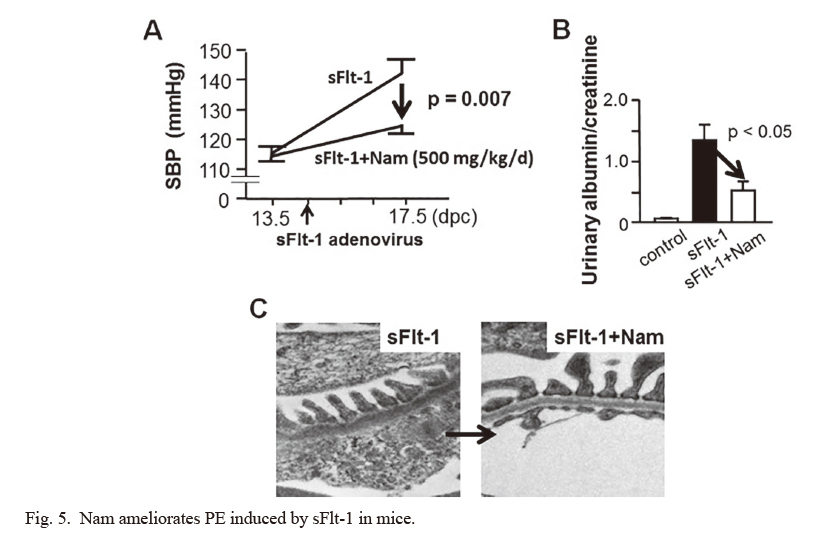
To test our hypothesis that Nam ameliorates PE, premature delivery, and FGR, we evaluated the effects of Nam on PE using three mechanistically different mouse models. We first used excessive sFlt-1 model by overexpressing sFlt-1 using adenovirus. In this model Nam alleviated all of the characteristic features of PE: hypertension, proteinuria, and endotheliosis (Fig. 5) (Li et al. 2016). Moreover, Nam prolonged the pregnancy period, reduced miscarriage rate and premature delivery, and corrected FGR (Fig. 6). Nam corrects hypertension at least partly by inhibiting ADP ribosyl cyclase. Nam prolongs pregnancy period, alleviates FGR likely through improving mitochondrial function and ATP production (Li et al. 2016).
The second mouse model of PE is the mice lacking Asb4 (Ankiryn-repeat-and-suppressor of cytokine signaling (SOCS)-box-containing-protein 4). These mice have a problem in implantation of embryos and development of placenta, and causes PE and fetal death (Townley-Tilson et al. 2014). In these mice Nam improves the characteristic features of PE, prolongs the pregnancy, and increased fetal survival rate (Li et al. 2016).
The third mouse model of PE is reduced uterine perfusion pressure (RUPP) model. RUPP model in rats has been widely used, and is produced by surgically ligating arteries to the uterus. To investigate the role of genes on PE, we need to study using mice, because there are already many different kinds of genetically engineered mice. However, it has been difficult to develop mouse RUPP model. We developed a mouse RUPP model for the first time by ligating vessels feeding uterus, placenta and fetuses with nylon thread, and immediately removing it to give a space in the vessels for blood to flow (Fig. 7) (Fushima et al. 2016). Using this mouse RUPP model, we have confirmed that Nam also alleviates PE, premature birth, and FGR (Fushima et al. 2017).
Perspectives
Nam is water-soluble vitamin B3 and used for treating various diseases, such as pellagra, bullous pemphigoid, schizophrenia, depression, insomnia, and Alzheimer’s disease. It is a safe drug and is also used for pregnant and nursing women who have difficulty in taking sufficient meal (Knip et al. 2000). In the three mouse models of PE that recapitulate human PE, we have demonstrated that Nam is the first drug that improves and prevents all of hypertension, proteinuria, endotheliosis, miscarriage/premature birth, and FGR. After confirming the safety and efficacy of Nam to preeclamptic women and successful clinical trials, indication of Nam should be expanded to treatment and prevention of PE. Nam is likely to save both mothers and fetuses, to improve development, and to prevent the metabolic syndrome and cardiovascular diseases of the babies all over the world because it is inexpensive.
Acknowledgments
We thank H.W. Davin Townley-Tilson, Hironobu Nakada, John R. Hagaman, Jennifer Wilder, and Manyu Li, J. Charles Jennette, Nobuyo Maeda, and Oliver Smithies.
Our work was supported by a Grant-In-Aid from the Japan Society of Promotion of Science (JSPS, 24659409), Translational Research Network Program of Ministry of Education, Culture, Sports, Science and Technology of Japan (J140001192), a major grant from the National Institutes of Health (HL049277), funds from the Department of Pathology and Laboratory Medicine at UNC Chapel Hill, the Naito Foundation and Miyagi Kidney Foundation.
Conflict of Interest
The authors declare no conflict of interest.
References
-
Arendshorst,
W.J. &
Thai,
T.L.
(2009) Regulation of the renal microcirculation by ryanodine receptors and calcium-induced calcium release. Curr. Opin. Nephrol. Hypertens., 18, 40-49.
-
Dulak,
J.,
Loboda,
A.,
Zagorska,
A. &
Jozkowicz,
A.
(2004) Complex role of heme oxygenase-1 in angiogenesis. Antioxid. Redox Signal., 6, 858-866.
-
Fushima,
T.,
Sekimoto,
A.,
Minato,
T.,
Ito,
T.,
Oe,
Y.,
Kisu,
K.,
Sato,
E.,
Funamoto,
K.,
Hayase,
T.,
Kimura,
Y.,
Ito,
S.,
Sato,
H. &
Takahashi,
N.
(2016) Reduced uterine perfusion pressure (RUPP) model of preeclampsia in mice. PLoS One, 11, e0155426.
-
Fushima,
T.,
Sekimoto,
A.,
Oe,
Y.,
Sato,
E.,
Ito,
S.,
Sato,
H. &
Takahashi,
N.
(2017) Nicotinamide ameliorates a preeclampsia-like condition in mice with reduced uterine perfusion pressure. Am. J. Physiol. Renal Physiol., 312, F366-F372.
-
Kingman,
M.,
Ruggiero,
R. &
Torres,
F.
(2009) Ambrisentan, an endothelin receptor type A-selective endothelin receptor antagonist, for the treatment of pulmonary arterial hypertension. Expert Opin. Pharmacother., 10, 1847-1858.
-
Knip,
M.,
Douek,
I.F.,
Moore,
W.P.,
Gillmor,
H.A.,
McLean,
A.E.,
Bingley,
P.J. &
Gale,
E.A.
(2000) Safety of high-dose nicotinamide: a review. Diabetologia, 43, 1337-1345.
-
Levine,
R.J.,
Maynard,
S.E.,
Qian,
C.,
Lim,
K.H.,
England,
L.J.,
Yu,
K.F.,
Schisterman,
E.F.,
Thadhani,
R.,
Sachs,
B.P.,
Epstein,
F.H.,
Sibai,
B.M.,
Sukhatme,
V.P. &
Karumanchi,
S.A.
(2004) Circulating angiogenic factors and the risk of preeclampsia. N. Engl. J. Med., 350, 672-683.
-
Li,
F.,
Fushima,
T.,
Oyanagi,
G.,
Townley-Tilson,
H.W.,
Sato,
E.,
Nakada,
H.,
Oe,
Y.,
Hagaman,
J.R.,
Wilder,
J.,
Li,
M.,
Sekimoto,
A.,
Saigusa,
D.,
Sato,
H.,
Ito,
S.,
Jennette,
J.C., et al.
(2016) Nicotinamide benefits both mothers and pups in two contrasting mouse models of preeclampsia. Proc. Natl. Acad. Sci. USA, 113, 13450-13455.
-
Li,
F.,
Hagaman,
J.R.,
Kim,
H.S.,
Maeda,
N.,
Jennette,
J.C.,
Faber,
J.E.,
Karumanchi,
S.A.,
Smithies,
O. &
Takahashi,
N.
(2012) eNOS deficiency acts through endothelin to aggravate sFlt-1-induced pre-eclampsia-like phenotype. J. Am. Soc. Nephrol., 23, 652-660.
-
Murphy,
S.R.,
LaMarca,
B.B.,
Cockrell,
K. &
Granger,
J.P.
(2010) Role of endothelin in mediating soluble fms-like tyrosine kinase 1-induced hypertension in pregnant rats. Hypertension, 55, 394-398.
-
Nuyt,
A.M.,
Lavoie,
J.C.,
Mohamed,
I.,
Paquette,
K. &
Luu,
T.M.
(2017) Adult consequences of extremely preterm birth: cardiovascular and metabolic diseases risk factors, mechanisms, and prevention avenues. Clin. Perinatol., 44, 315-332.
-
Sutton,
P.S. &
Darmstadt,
G.L.
(2013) Preterm birth and neurodevelopment: a review of outcomes and recommendations for early identification and cost-effective interventions. J. Trop. Pediatr., 59, 258-265.
-
Thai,
T.L. &
Arendshorst,
W.J.
(2008) ADP-ribosyl cyclase and ryanodine receptors mediate endothelin ETA and ETB receptor-induced renal vasoconstriction in vivo. Am. J. Physiol. Renal Physiol., 295, F360-368.
-
Townley-Tilson,
W.H.,
Wu,
Y.,
Ferguson,
J.E. 3rd &
Patterson,
C.
(2014) The ubiquitin ligase ASB4 promotes trophoblast differentiation through the degradation of ID2. PLoS One, 9, e89451.
-
von Dadelszen,
P.,
Ornstein,
M.P.,
Bull,
S.B.,
Logan,
A.G.,
Koren,
G. &
Magee,
L.A.
(2000) Fall in mean arterial pressure and fetal growth restriction in pregnancy hypertension: a meta-analysis. Lancet, 355, 87-92.