Regular Contribution
Positive Emotion and its Changes during Pregnancy: Adjunct Study of Japan Environment and Children’s Study in Miyagi Prefecture
2018 Volume 245 Issue 4 Pages 223-230
Details
2018 Volume 245 Issue 4 Pages 223-230
During pregnancy, women experience various emotional changes. Previous research has investigated positive emotion influenced childbirth outcomes positively. This study explored the extent of positive emotion which pregnant women aware of their own pregnancy life subjectively and variables related to the changes thereof. This was an adjunct study of the Japan Environment and Children’s Study which is a nationwide epidemiological study to identify the impact of environmental factors on health and development of children in Miyagi Prefecture. Data were collected at 12 weeks (T1) and 24-28 weeks (T2) of gestation. Participants were 3,513 pregnant women. Women’s degree of positive emotion was assessed through a numeric rating scale. We also measured related variables, including obstetric factors, physical health status, mental health status, and social situation, using the 8-Item Short Form Health Survey, Kessler-6, and family APGAR score, along with demographic data. Analyses included correlations among variables related to the change in positive emotion. The extent of positive emotion was significantly related with health-related quality of life and satisfaction with family relationships during pregnancy. The women whose positive emotion decreased from T1 to T2 tended to have lower morning sickness symptoms, be unemployed, lower physical and mental health status, and a higher risk of psychological distress in middle pregnancy. Importantly, even discomfort like morning sickness, physical symptoms that indicate being pregnant, might make women to confirm pregnancy. Moreover, employment and satisfaction with family relationships are especially crucial for pregnant women to spend comfortable maternity life.
Generally, most women experience anxiety and concerns regarding the physiological, psychological, and social changes through their pregnancy period. Antenatal depression and anxiety, which lead to maternal negative emotion, have been shown to be associated with not only birth outcomes, such as preterm birth and low birth weight, but also postnatal maternal mental health and infant growth, such as postnatal depression and adverse infant development (Braungart-Rieker et al. 2016; Camkurt et al. 2016; Cirik et al. 2016; Dollberg et al. 2016; Liou et al. 2016).
In contrast, research over the past several decades has shown that positive emotion during pregnancy has influenced several childbirth outcomes positively. Using 3,376 pregnant women, Pesonen et al. (2016) reported that having more positive emotion in the third trimester was associated with a decreased risk of preterm delivery as having a longer gestational period. A positive state of mind and emotional stability during pregnancy were associated with more normal delivery and better maternal childbirth experiences (Hernández-Martínez et al. 2011). In addition, the association between maternal positive psychological aspects during pregnancy and better postnatal mental health has also been explored. In a questionnaire survey of 272 postnatal women, positive emotion in late pregnancy was associated with less depression, less perceived stress, more social support, a higher quality of life (QOL), and perceiving one’s infant as less difficult; it also functioned as a buffer against postpartum depression (Bos et al. 2013). Moreover, a recent intervention study suggested that the improved well-being of pregnant women reduced their pregnancy-specific psychological stress (Matvienko-Sikar and Dockray 2016). Based on previous reports, it is important for pregnant women to spend their life with subjectively positive emotion through pregnancy period.
Midwives should be a person who understands and supports pregnant women’s emotion which includes mood swings, ambivalent feelings, and change in negative and positive emotions in their professional settings. Pesonen et al. (2016) reported that mothers who had undergone preterm delivery showed a decline in positive affect and an increase in depression and anxiety in the weeks prior to delivery. Voellmin et al. (2013) also showed that a sharp increase in positive emotion over the course of gestation was associated with a longer duration of pregnancy. However, these studies focused only on childbirth outcomes. Few studies have investigated the effects of the change in positive emotion over the course of pregnancy. It is important for healthcare providers to assess changes in positive emotions, especially to screen for women who might show a decrease in positive emotions during pregnancy.
The purpose of this study was to explore positive emotion during pregnancy and identify the variables potentially contributing to changes in positive emotion during pregnancy. The exploration of variables responsible for changes in positive emotion during pregnancy could provide healthcare professionals with important information regarding care provided to pregnant women.
This study was performed as a part of Japan Environment and Children’s Study (JECS) Adjunct Study (outlined in the JECS protocol paper: Kawamoto et al. 2014). The JECS, a national birth cohort study involving 100,000 parent-child pairs, commenced in 2011 and investigated the effects of various environmental factors on children’s health and development. Recruitment occurred from January 2011 to March 2014 from 15 Regional Unit Centers in Japan. Health outcome and exposure measurements will continue until the participating children are 13 years old (For more details at http://www.env.go.jp/chemi/ceh/en/). Pregnant women were recruited during early pregnancy. After providing informed consent, participants completed the questionnaire at 12 weeks (T1) and 24-28 weeks (T2) of gestation, and several times after childbirth. At Miyagi Unit Center (MUC), 9,031 pregnant women participated in the main study and 3,578 agreed to participate in an adjunct study. In this study, we used data collected at T1 and T2.
MeasurementPositive emotion: It is comfortable feeling which pregnant women aware of their own pregnancy life subjectively. The Numerical Rating Scale (NRS) on the subjective degree of comfort during pregnancy was used. The NRS used an 11-point scale (Are you comfortable with your current pregnancy life? “very uncomfortable” [0] to “very comfortable” [10]) at T1 and T2.
Obstetrical variables: Delivery history, infertility treatment (“yes”/”no”), morning sickness symptoms at T1, and perception of fetal movement at T2 were used as obstetrical variables. Morning sickness symptoms were evaluated with the following options: none (1), only nausea (2), vomiting, but able to eat (3), and vomiting and unable to eat (4). Perception of fetal movement also entailed four options: frequently (4), sometimes (3), occasionally (2), and rarely (1).
Physical health status: The physical component of physical health summary score (PCS) which was estimated from the 8-Item Short Form Health Survey (SF-8) (Fukuhara and Suzukamo 2005) and a single item on physical domestic violence (p-DV) were used at T1 and T2. The SF-8 comprises eight items measuring health-related concepts such as physical function (PF), role limitations because of physical health problems (RP), bodily pain (BP), general health perception (GH), vitality (VT), social function (SF), role limitations because of emotional problems (RE), and mental health (MH). The higher score shows better health-related QOL. These scores are comparable to the standardized Japanese population norm-based score (NBS). The Cronbach’s αcoefficients were .82-.84 in this study.
Mental health status: The mental component of mental health summary score (MCS) which was calculated using each SF-8 item, an item on mental domestic violence (m-DV), and the Kessler-6 (K6) scale (Kessler et al. 2002; Furukawa et al. 2008), was used at T1 and T2. A was also The K6 comprises six items on a 5-point Likert scale (from “none” [1], to “all of the time” [5]); a score of > 5 was considered a clinically high risk of psychological distress (Kawakami et al. 2005). The Cronbach’s αcoefficients were .84-.87 in this study.
Social situation status: The Family APGAR (Smilkstein 1978) was used to assess family functioning which estimating family member’s satisfaction with family relationships at both T1 and T2. It comprises five items including adaptation, partnership, growth, affection, and resolve. Each item is rated on a 0-2 scale. Total scores of 0-3 indicated family dysfunction, 4-7 moderate dysfunction, and ≥ 8 good function. Two items relating to a social support (the presence of someone who shows affection and a consultation partner) were also administered, both assessed on a 5-point Likert scale. The Cronbach’s αcoefficients were .95-.96 in this study.
Demographic data: Age at delivery, type of family, marital status, education, income, and employment was assessed as demographic data.
AnalysisAmong the 3,578 women who agreed to participate in the MUC adjunct study, the data of 3,513 who provided information on comfort during pregnancy at both T1 and T2 were analyzed (we used provisional data set at 2015). The degree of comfort during pregnancy was statistically described, and its correlations with all other variables at T1 and T2 were assessed using Pearson’s correlation coefficient (interval scales) or Spearman’s rank correlation coefficient (nominal scales).
In assessing change in positive affect during pregnancy, women were classified into three groups based on their change in positive emotion from T1 to T2: no change, positive emotion-increase (IG), and positive emotion-decrease (DG). The factors related to the change in positive emotion were examined by comparing background variables between the IG and DG using Student’s t-test and the chi-square test. The significance level was set at < .05.
Ethical considerationsThis study was approved by the Ethics Committee of Tohoku University Graduate School of Medicine and the Ministry of Environment. The research coordinator of MUC explained the study and obtained consent. As this was an additional survey of pregnant women participating in the JECS, we obtained written consent separately from the JECS. Participants were assigned identification numbers to anonymize the data; these were further changed to other identifying numbers for double anonymization.
The frequency distribution for subjective degree of positive emotion is shown in Fig. 1. Mean degree of positive emotion at T1 was 6.13 (SD = 2.3), and at T2 was 6.18 (SD = 2.1), and there was no significant difference between the two time frames. The shape of distribution trends biased to the right side that was the more women who answered higher score.
Demographic data are shown in Table 1. Women’s mean age at delivery was 30.5 years; about one-third were primigravida; most were married, which is extremely common in Japan; more than half of households were nuclear family households; and two-thirds of the women were employed at T1, whereas at T2, only about half were employed.
The result of the correlations between positive emotion at each period and obstetrical, physical health, mental health, and social situation are shown in Table 2 (statistically significant variables only). Positive emotion at T1 was positively correlated with health-related QOL (r = .263-.400, p < .001) and family functioning at T1 (r = .270, p < .001), as well as health-related QOL (r = .272-.313, p < .001) at T2. Positive emotion at T2 was correlated positively with health-related QOL (r = .278-.473, p < .001) and family functioning (r = .303, p < .001) at T2, along with health-related QOL (r = .261-.281, p < .001) at T1.
To explore factors related to change in positive emotion from T1 to T2, we compared the IG and DG. To create the groups, we calculated differences in positive emotion between T2 and T1 (mean = 0.0495, SD = 2.27, and range = 10 to –10); those with differences higher than the first quartile (2 to 10) were classified as the IG (n = 794), while those with differences of lower than the third quartile (–2 and –10) were classified as the DG (n = 723). Demographic data for the groups are shown in Table 1. Women in the DG had significantly more deliveries (t = 2.44, p = .015), while a greater proportion of women in the IG were unmarried (𝜒2 = 4.701, p = .030) and employed at T1 (𝜒2 = 14.276, p < .001) and T2 (𝜒2 = 6.303, p = .012). There were no significant differences between the two groups in terms of family type, infertility treatment, education, or family income.
Comparison of the variables between the two groups is shown in Table 3. Women in the IG had significantly more severe morning sickness symptoms (t = 4.52, p < .001). Both the PCS and MCS at T1 and T2 differed significantly between the two groups (p < .001). There were no significant differences in p-DV or m-DV, except for p-DV at T1. The groups also differed in their perceptions of fetal movement and the proportion of women that with K6 scores ≥ 5. Family functioning at T1 differed significantly between the groups, with the DG group having a significantly higher percentage of women with good family functioning than the IG group.

Positive emotion of pregnancy life (n = 3,513).
Shown is the frequency distribution for subjective degree of comfort (positive emotion) at T1,12 weeks of pregnancy and T2, 24-28weeks of pregnancy. Note the two peaks at point 5 and point 8 in both periods.

Demographic data.
IG and DG were compared using Student’s t-test and chi-square test.
*p < .05, ***p < .001.
IG, positive emotion-increase group; DG, positive emotion-decrease group; T1, 12 gestational weeks; T2, 24-28 gestational weeks; one million yen = around 8,500 US dollars.
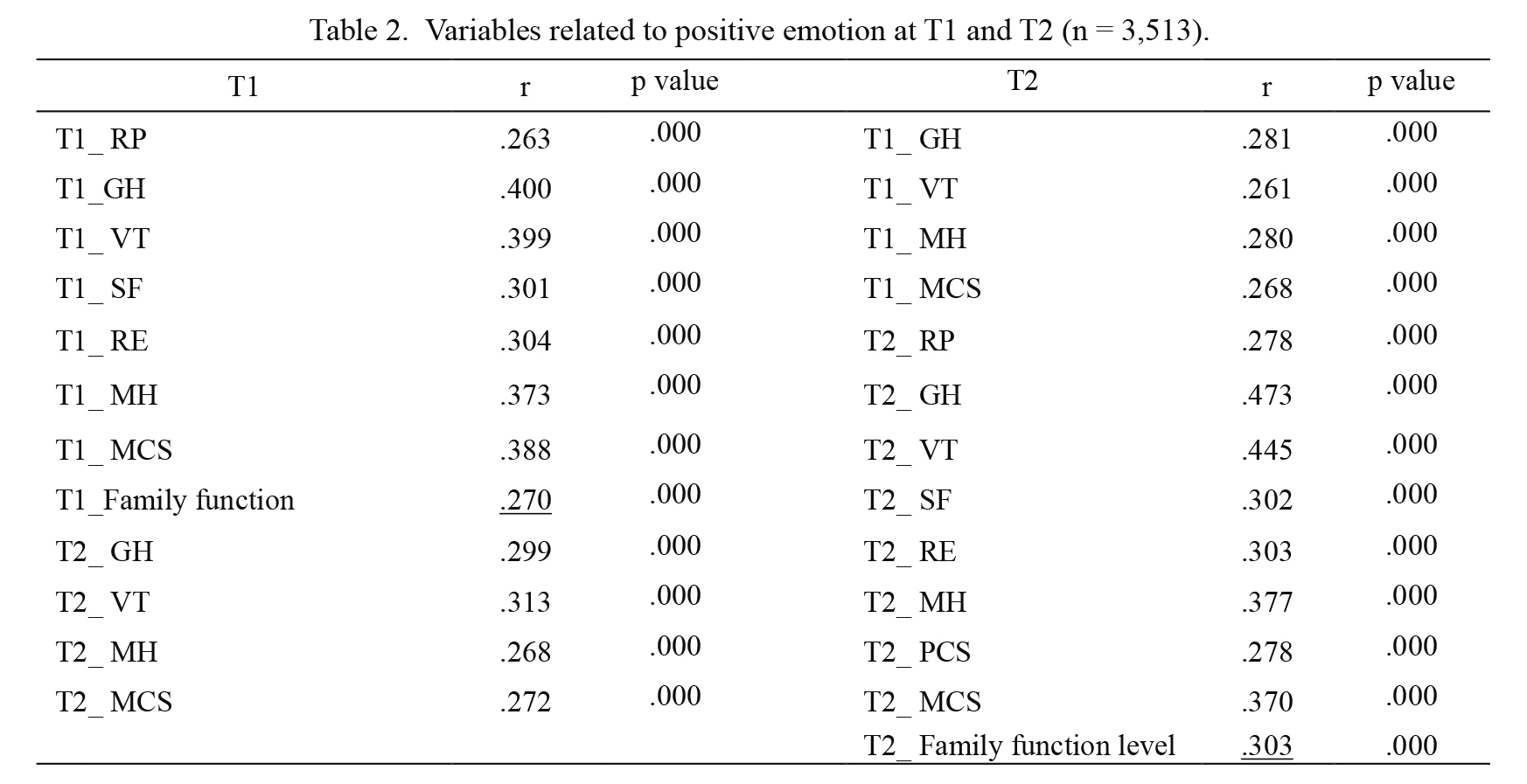
Variables related to positive emotion at T1 and T2 (n = 3,513).
Underline shows Spearman rank correlation coefficient (Pearson otherwise).
T1, 12 gestational weeks; T2, 24-28 gestational weeks; PF, physical function; RP, role limitations because of physical health problems; BP, bodily pain; GH, general health perception; VT, vitality; SF, social function; RE, role limitations because of emotional problems; MH, mental health; PCS, physical component summary; MCS, mental component summary.

Comparison between IG and DG.
Student’s t-test, *p < .05, **p < .01, ***p < .001.
IG, positive emotion-increase group; DG, positive emotion-decrease group; T1, 12 gestational weeks; T2, 24-28 gestational weeks; PCS, physical component summary; MCS, mental component summary; K6 positive, Score of Kessler-6 was > 5, and considered a clinically high risk of psychological distress.
This study is the first to explore the change in positive emotion from the early to the middle of pregnancy and the variables associated with that change. In both early and middle of pregnancy, participants had a moderate degree of positive emotion at around 6 out of 10 points, indicating an inclination towards experiencing positive emotion. It is generally recognized that the second trimester is a period in which the pregnancy stabilizes, which was reflected in the results for the degree of positive emotion during this period.
Positive emotion at T1 was significant, positively correlated with health-related QOL and family functioning at T1, and health-related QOL at T2. Positive emotion at T2 was significantly, positively correlated with health-related QOL and family functioning at T2, and health-related QOL at T1. Although health-related QOL and positive emotion are similar concepts, the results of this study showed that there were no significant correlations between all health-related QOL items and positive emotion and that these correlations were weak to moderate. This means that positive emotion and QOL should be treated as different emotional dimensions and that the mental and physical health of pregnant women is important for a positive emotion during pregnancy. A previous study exploring subjective comfort using a visual analog scale ranging from 0 to 100 showed significant differences between hospitalized and outpatient pregnant women (Nakamura et al. 2012). Moreover, hospitalized pregnant women had significantly lower health-related QOL score than did outpatient pregnant women. Nakamura et al. (2011) also support our results. The physical changes associated with pregnancy places pregnant women at risk of developing various diseases and complications. Therefore, to ensure positive emotion during pregnancy, women should maintain a healthy lifestyle during the course of pregnancy.
Family functioning was also related to positive emotion during pregnancy, meaning that assessing pregnant women’s family functioning and support could help ensure their positive emotion. In a Pakistani cross-sectional survey, family support was highlighted as a protective factor against the prevalence of psychological distress during pregnancy (Khan et al. 2015). A cross-sectional study in Canada of 2,282 pregnant women also showed the importance of family support, demonstrating that lack of family support was associated with a lower diet quality during pregnancy (Nash et al. 2013). Additionally, less family support during pregnancy was significantly related to greater leisure time and physical activity barriers (Doran and Davis 2011; Da Costa and Ireland 2013). Family functioning is one of the most important factors for the mental health of pregnant women in crisis situations (Ren et al. 2014). Therefore, family functioning should be assessed by antenatal healthcare providers to ensure a positive emotion for pregnant women.
In this study, we focused on the change in positive emotion during pregnancy, and this is the first such report about the pregnancy population. Women whose positive emotion level increased from early to middle pregnancy were more likely to be unmarried and employed in early or middle pregnancy, and have a high risk of psychological distress and poor family functioning in early pregnancy. In contrast, women with decreased positive emotion levels from early to middle pregnancy had lower morning sickness symptoms, lower Physical and Mental health status, and a higher risk of psychological distress in middle pregnancy. In a previous longitudinal study on positive emotion during pregnancy, Pesonen et al. (2016) reported no significant differences for maternal positive emotion between the first, second, and third trimester, although depression and anxiety were significantly higher in the second trimester than in the first and third trimesters. Moreover, pregnant women’s perceptions of well-being at weeks 10-12 were significantly better than were those at weeks 34-36 (Sjostrom et al. 2004). Positive emotion in late pregnancy was associated with less intense depressive symptomatology, less self-perceived stress, more self-reported social support, higher QOL (Bos et al. 2013), and a decreased risk of preterm delivery (Pesonen et al. 2016). Positive emotion is also associated with having a normal delivery (Hernández- Martínez et al. 2011) and the perception of having a less difficult infant, which protected against postpartum depression (Bos et al. 2013) and facilitated maternal role attainment in the early postpartum period (Nakamura et al. 2015). Thus, while there are no consistent results regarding changes in pregnant women’s positive emotion, having positive emotion is associated with positive outcomes of pregnancy, delivery, and postpartum. Therefore, appropriate nursing care that targets positive emotion in middle pregnancy based on observed changes in pregnant women’s positive emotion could contribute to a more comfortable pregnancy and positively influence delivery and childrearing.
Mild morning sickness symptoms in early pregnancy were associated with decreased positive emotion from early to middle pregnancy. Pregnant women with severe nausea and vomiting are known to have lower health-related QOL compared to women not experiencing these symptoms (Bai et al. 2016). Moreover, the severity of nausea is associated with lower physical and mental QOL among pregnant women (Lacasse et al. 2008; McCarthy et al. 2011). Nonetheless, some pregnant women perceive morning sickness as a positive experience, regarding it as being a sign of fetal health and a valuable experience that can only be felt by someone who is pregnant (Iwakuni 2016). Therefore, pregnant women with mild morning symptoms in early pregnancy might require nursing care that not only targets their physical comfort but also affirms their pregnancy.
Another characteristic of pregnant women showed decreasing comfort towards middle pregnancy was unemployment in early and/or middle pregnancy. Some previous studies on the psychological aspects of employed pregnant women revealed that they had a significantly better psychological status than did unemployed pregnant women (Yubune et al. 2008; Anan et al. 2010; Ogawa et al. 2015; Sagayadevan et al. 2015), on the other hand, some studies found no difference between the groups (Japan Association for The Advancement of Working Women 2006; Minazuki 2015). Still, other studies on employed pregnant Japanese women reported that those who had stopped working during pregnancy had significantly lower mental health statuses (Matsuzaki et al. 2011). Thus, there was a possibility that discontinued employment led to reduced comfort during pregnancy. There is also the possibility of leaving work due to being worse for the health condition of pregnancy. It is important to assess the reason why women have left work, and whether they are convinced that they quit their jobs. There is a need for further research, including on the employment situation during pregnancy.
In a longitudinal study on changes in comfort (a comfort scale comprising five subscales), Ogawa et al. (2015) reported that a significant increase in comfort during pregnancy is related to employed pregnant women’s relationships with their husbands, who are approaching fatherhood; such a relationship was not found for unemployed pregnant women. In this study, positive emotion was evaluated using the NRS in terms of a comfortable. Therefore, further research is needed to clarify which aspects of positive emotions had decreased to enable the provision of relevant nursing support for pregnant women.
There were several limitations to this study. First, all participants resided around Miyagi, in the northeast of Japan, which is a semi-urban area. The structure of childcare support differs across regions, especially between urban and rural areas; so, there might be differences in family function and sources of social support (Ochiai 1989; Matsuda 2002; Mizugaki and Takeda 2015). Second, we measured positive emotion in terms of pregnancy comfort. In a previous concept analysis of prenatal well-being, this concept was highlighted as multi-dimensional (consisting of physical, psychological, social, spiritual, economic, and ecological elements) (Allan et al. 2013). In contrast, Pinto et al. (2017) stated that comfort is a broader holistic concept, whereas well-being is primarily a psycho-spiritual dimension. Thus, a multi-dimensional measurement of positive emotion should be used during pregnancy, in order to provide more specific care to pregnant women and thus ensure a more positive and/or comfortable pregnancy. Despite these limitations, this study is the first to explore the change in positive emotion from early to middle of pregnancy and the variables related to this change. These results could contribute to the knowledge of screening and assessment for healthcare providers.
Health-related QOL and family function were related to positive emotion during pregnancy. Moreover, decreased positive emotion from early to middle pregnancy was especially associated with less severe morning sickness symptoms and being unemployed in early and/or middle pregnancy. Healthcare providers must assess not only physical health but also the psychological and social dimensions of pregnancy, to facilitate a better antenatal period.
This Adjunct Study was conducted in Miyagi Unit Center as a part of Japan Environment and Children’s Study of the Ministry of the Environment, Government of Japan. The findings and conclusions of this article are solely the responsibility of the authors and do not represent the official views of the above government. This study was partly supported by a grant for the JECS from the Ministry of Environment, This study was partly supported by Japan and Research Promotion and Practical Use for Women’s Health, AMED, and financial support of a program to supporting research activities of female researchers of Tohoku University.
The authors declare no conflict of interest.