Abstract
With the decreasing global trend in the Helicobacter pylori infection rate, compositional changes in the gastric cancer subsites have occurred worldwide. However, the compositional changes in Asian countries, including Japan, remain to be clarified. The aim of this study is to investigate the latest chronological changes in the gastric cancer subsite using a hospital-based registration system in Akita prefecture in Japan. From 2007-2015, subsites of gastric cancers were coded according to the International Classification of Diseases for Oncology (ICD-03). The nine-year registration period was divided into the three 3-year periods: 2007-2009, 2010-2012, and 2013-2015. A total of 10,804 cases of gastric cancer were registered. The proportion of cardiac cancer among total gastric cancer slightly but significantly declined from 12.1% in 2007-2009 to 9.2% in 2013-2015 (P < 0.01). Among non-cardia cancer, the proportion of corpus cancer significantly increased from 41.3% to 50.2% during the study period (P < 0.01), while that of antropylorus cancer significantly decreased from 37.6% to 34.3% (P < 0.05). Such compositional changes in the gastric cancer subsite were observed largely in men, regardless of the histologic subtype of cancer. With the decreasing H. pylori infection rate, compositional changes in the gastric cancer subsite are occurring in Japan. While the proportion of cardia and antropylorus cancer is declining, that of corpus cancer is increasing, indicating diverse etiology of gastric carcinogenesis depending on the subsites. Identifying the most common sites of occurrence, may help to improve the efficiency of screening for gastric cancer.
Introduction
The incidence of gastric cancer has been steadily declining worldwide, mostly due to the decreasing global trend in the Helicobacter pylori infection rate. However, gastric cancer remains the second leading cause of death from cancer worldwide as well as in Japan (Lau et al. 2006; Dassen et al. 2010; Inoue 2017), so investigations into the etiology of gastric cancer are still noteworthy.
Some compositional changes in the anatomical site of gastric cancer have been observed in the US and European countries. Gastric cancers are divided into two subtypes depending on the anatomical location: cardiac gastric cancer (CGC) and non-cardiac gastric cancer (NCGC). An increased incidence of CGC relative to NCGC has been reported since the early 1970s, although the trend has plateaued in more recent surveys (Blot et al. 1991; Botterweck et al. 2000; Wu et al. 2009). In addition, parallel with the increase in the incidence of CGC, the incidence of corpus cancer has also increased since the 1980s in the US and European countries (Anderson et al. 2010; Camargo et al. 2011; Holster et al. 2014).
Eastern Asia, including Japan, is known to be an area with a particularly high incidence of and mortality due to gastric cancer (Inoue 2017). However, only a few studies have investigated the chronological shift in the subsites of gastric cancer in Asian countries. Of note, the trend in the prevalence of CGC has never been studied using a population-based registration database in Japan (Hatta et al. 2017), mainly because, until quite recently, the location of gastric cancer was diagnosed based on the Japanese Classification of Gastric Carcinoma, in which the cancer location is usually described anatomically in three parts as the upper third (cardia plus fundus), middle third, or lower third, making it difficult to distinguish the “cardia” from the upper third of the stomach (Liu et al. 2004; Inoue et al. 2009; Honda et al. 2017).
Akita Prefecture is located in the northern region of Honshu, the main island of Japan, and has a population of approximately 1 million. The prefecture has had one of the highest gastric cancer-related mortality rates in Japan for the past several years. We recently reported on the recent trends in esophageal cancer using our hospital-based registration system for cancer cases in Akita Prefecture, which was started in 2007 (Koizumi et al. 2018).
In the present study, using a hospital-based cancer registration system in which gastric cancer was diagnosed according to the international standard (ICD-O-3) from the outset (WHO, World Health Organization 1993), we investigated the recent trend (2007-2015) in the compositional change of gastric cancer subsites with a particular focus on the histologic subtypes and gender.
Patients and Methods
In this analysis, we employed the database from the collaborative Akita Prefecture hospital-based registration system of cancers, in which the main hospitals in the prefecture participate. During the patient registration period, all patients histologically diagnosed with gastric cancer were registered in the system regardless of what subsequent therapies were administered. The system was started in 5 hospitals in 2007. Since then, the number of participating hospitals has gradually increased, and 11 hospitals have consistently participated since 2011. In Akita Prefecture, the facilities for the treatment of cancers are concentrated in major hospitals, and these 11 hospitals cover more than 90% of total patients with cancer in Akita Prefecture. Thus, the system provides near population-based data in this region (Koizumi et al. 2018). Using this registration system, we examined the latest trends in the occurrence of gastric cancer in 2007-2015 in Akita Prefecture from the perspective of gastric cancer subsites and histology.
The subsites of gastric cancer registered in our system throughout the study period were coded according to the International Classification of Diseases for Oncology (ICD-03), in which the tumor location was divided into cardia (C16.0), fundus (upper third) (C16.1), corpus (middle third) (C16.2), antrum and pylorus (lower third) (C16.3 and C16.4), overlapping contiguous subsite (C16.8), and unspecified subsite (C16.9) (WHO 1993). The subsite of gastric cancer was defined as a predominantly affected area for a large gastric cancer extending over two areas. Gastric cancers were histologically classified into two subtypes: intestinal type and diffuse type, based on the criteria proposed by Lauren (1965).
Statistical analyses
The nine-year registration period was divided in chronological order into the three 3-year periods: period A (2007-2009), period B (2010-2012), and period C (2013-2015). The characteristics were compared among the three chronological periods. Data were expressed as the mean (standard deviation) for continuous variables and number (percentage) for categorical variables. Comparisons were made using the unpaired t-test for continuous variables and Chi-square test for categorical variables. Changes in the chronological trend of cancer subsites were analyzed by Cochran Armitage trend test. All analyses were performed using JMP Pro 13 (SAS Institute Inc. Cary, USA) and a p-value < 0.05 was considered statistically significant. This analysis was approved by the Akita University School of Medicine Ethics Committee (1237).
Results
A total of 10,804 cases with gastric cancer was registered in the 9-year study period of 2007-2015. The mean age of the cases was 71.7 (10.8) years, and 7,394 (68.4%) were men. Regarding the subsite of gastric cancer, the corpus accounted for the majority of cases (5,048 [46.7%]), followed by the antropylorus (3,867; 35.8%), cardia (1,121; 10.4%), and fornix (137; 1.3%), leaving 640 cases (5.9%) with an unknown location. The histological subtypes of cancer were defined in 9,181 (85.0%), and 6,336 (69.0%) and 2,845 cases (31.0%) were intestinal type and diffuse type, respectively (Table 1). The characteristic features are shown according to the cancer subsite. The men/women ratio was the highest in the cardia and decreased as the location became more distal: 3.2 for cardia, 2.8 for fornix, 2.2 for corpus, and 1.9 for antropylorus. The intestinal type was more prevalent in the antrum than at other sites (Table 1).
The number of registered cases increased over time, from 2,760 cases in period A (2007-2009), 3,927 in period B (2010-2012), and to 4,117 in period C (2013-2015), mainly due to the increasing number of participating hospitals (Table 2). Indeed, as described below, according to the database from the 5 hospitals participating in the registry from the beginning of the study in 2007, the number of gastric cancer cases was relatively stable at around 2,000 cases in each chronological period.
The men/women ratio was similar among the three chronological groups. The mean age of patients has significantly increased over time as in a report from the Japanese Cancer Registry (Inoue 2017). The proportion of CGC significantly declined during the study period, from 12.1% (333/2,760) in period A to 10.5% (411/3,927) in period B and 9.2% in period C (377/4,117) (P < 0.01). Similarly, the proportion of antropylorus cancer significantly declined chronologically from 37.6% (1,039/2,760) in period A to 36.5% (1,416/3,927) in period B and 34.3% (1,412/4,117) in period C (P < 0.05). In contrast, the proportion of corpus cancer steadily and significantly increased during the study period, from 41.3% (1,140/2,760) in period A to 46.7% (1,833/3,927) in period B and 50.2% (2,069/4,117) in period C (P < 0.01). In addition, fornix cancer accounted for only 1%-2% of total gastric cancer throughout the study period (Table 2 and Fig. 1A). These chronological changes in the subsites of gastric cancer were more prominently observed at early stage (stage T1 or T2) compared with advanced stage (stage T3 or T4) (Table 3). Regarding the histological subtypes, no clear trend was noted during the study period, with 65%-70% of cases being intestinal type and 30%-35% of diffuse type among those with a defined histology.
The results of a subgroup analysis based on the database from the five originally participating hospitals are shown in Table 4, allowing the direct comparison of the absolute number of cases during the study period. The trends in the number of cases at each subsite among the five hospitals were largely similar to the changes in the proportions among the overall participating hospitals.
Chronological changes in the subsite and histology in the overall participating hospitals were separately shown for men and women (Table 5 and Fig. 1B, C), and a somewhat distinct trend regarding the cancer subsite was noted between genders. The decreases in CGC as well as the increase in corpus cancer were more prominently observed in men compared with women (P < 0.01 in men vs. P < 0.05 in women for both cancers, respectively). While the proportion of antropylorus cancer significantly declined in men (P < 0.01), there was no such trend in women. (Table 5 and Fig. 1C). No chronological trend was noted regarding the proportion of histological subtype in men or women (Table 5).
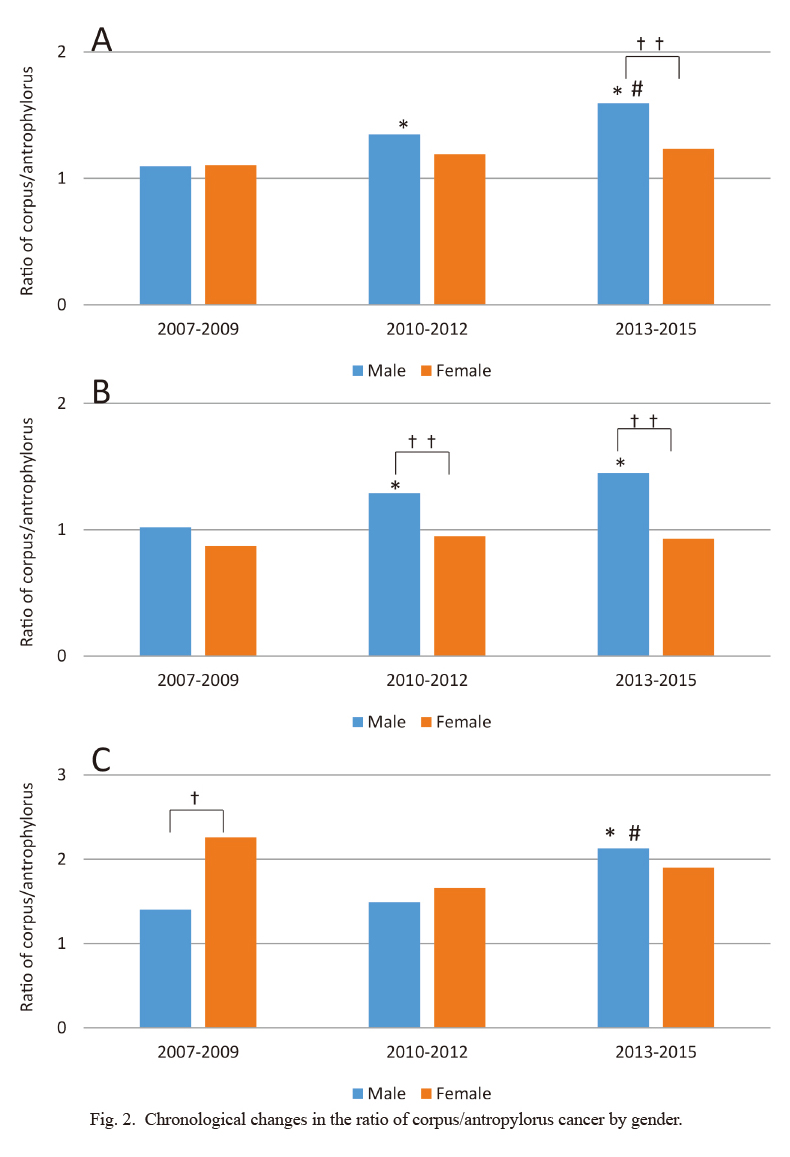
Distinct chronological trends in the subsite of gastric cancer between genders were further illustrated by assessing the ratio of corpus/antropylorus in each period (Fig. 2A). The corpus/antropylorus ratio in men was 1.10 in period A and increased to 1.35 in period B (P < 0.01) and 1.59 in period C (P < 0.01). In contrast, the corpus/antropylorus ratio in women did not significantly change during the study period (1.11, 1.19, and 1.23 in periods A, B, and C, respectively). Consequently, while the corpus/antropylorus ratio was similar between the genders in period A (1.10 for men and 1.11 for women), a difference in the ratio became obvious in period C (1.59 for men and 1.23 for women, P < 0.01). These results indicate that the increasing trend in the prevalence of corpus cancer as well as the decreasing trend in that of antropylorus cancer was a phenomenon largely confined to men.
The distinct chronological trends in the prevalence of corpus and antropylorus gastric cancer between genders were also true in both histological subtypes. Significant increases in the proportion of corpus cancer were observed in both histological subtypes exclusively in men (Table 6). For intestinal-type, while the corpus/antropylorus ratio significantly increased in men (1.02, 1.29, and 1.45 in periods A, B, and C, respectively, P < 0.01: period A vs. B and B vs. C), there was no apparent sequential trend in women (0.87, 0.95. and 0.93 in periods A, B, and C, respectively). Similarly, for diffuse-type, the ratio of corpus/antropylorus showed a significant increase during the study period in men (1.40, 1.49, and 2.13 in periods A, B, and C, respectively, P < 0.01: period A vs. C and B vs. C) (Fig. 2B), but there was no sequentially apparent trend in the ratio in women, although the ratio showed a high value from the beginning in women (2.26, 1.66, and 1.90 in periods A, B, and C, respectively) (Fig. 2C).

Discussion
In the present study, using the latest hospital-based cancer registration system during a nine-year period (2007-2015) in Akita Prefecture in Japan, we found that the proportion of CGC among total gastric cancer slightly but significantly declined. In addition, we found that the proportion of corpus gastric cancer significantly increased while that of antropylorus cancer declined, and this trend was observed largely in men regardless of the histologic subtype of cancer.
There is substantial geographical variation in the proportion of CGC among total gastric cancer (Ferro et al. 2014; Colquhoun et al. 2015). NCGCs constitute the vast majority of total gastric cancer, leaving only a small portion (about 10%) of CGC in Eastern Asia. In contrast, in European counties and the US, the incidence of CGC is comparable to that of NCGC, and CGC accounts for about half of total gastric cancer (Ferro et al. 2014; Colquhoun et al. 2015). Geographic differences in the H. pylori infection rate in the general population of each country are at least partly responsible for the difference in the proportion of CGC, as H. pylori infection is more closely associated with the development of NCGC than that of CGC (Parsonnet et al. 1991). In turn, compositional changes in CGC are expected in Asian countries where the H. pylori infection rate is steadily declining, albeit lagging behind Western countries. However, only a few studies in Asian countries have examined this issue, all of which have been retrospective single-center studies showing conflicting results (Bor et al. 2007; Kusano et al. 2008; Zhou et al. 2008; Hasegawa et al. 2009).
In this study, utilizing a hospital-based cancer registration system, we successfully demonstrated the latest trends in CGC in Japan for the first time, showing that the proportion of CGC was not increased but instead slightly but significantly decreased in Japan. The decreasing trend in CGC observed in this study contrasts with the results from Western countries (Blot et al. 1991; Botterweck et al. 2000; Wu et al. 2009) and might not reconcile with our recent report, which showed an increasing trend in esophageal adenocarcinoma using the same database (Koizumi et al. 2018), as both cancers are recognized to share the same etiologic factor (gastro-esophageal reflux disease [GERD]). However, it is also recognized that CGC consists of two different pathways to carcinogenesis: a GERD-related pathway similar to esophageal adenocarcinoma, and a non-GERD-related pathway involving H. pylori infection.
CGC can be induced by H. pylori infection-related inflammation and atrophy, as can NCGC (Derakhshan et al. 2008; Horii et al. 2011). Indeed, the H. pylori-related pathway is the predominant mechanism of CGC carcinogenesis in Japan and Korea, as previous studies have indicated that H. pylori-related corporal inflammation or atrophy is observed in 55%-95% of CGC patients in these countries (Egi et al. 2007; Kamada et al. 2012; Kim et al. 2012; Yamada et al. 2014), which is in contrast to the situation in Western countries (Cavaleiro-Pinto et al. 2011). Thus, since most CGC has a different etiologic background from esophageal adenocarcinoma in Japan, it is unsurprising that the changing trend in CGC does not parallel that of esophageal adenocarcinoma.
The present study showed that CGC accounts for only a small portion of total gastric cancers in Japan. However, we must be alert for potential increases in the trend of CGC in the future in Japan, as the prevalence of GERD is increasing in Asia in general as well as in Japan specifically (Wong and Kinoshita 2006; Fujiwara and Arakawa 2009). Indeed, the population-based registry data from the US indicated that there was a decrease in the incidence of CGC until the late 1960s, then followed by a steady increase since the 1970s (Abrams et al. 2013).
A number of studies from not only Western countries but also Japan have described increasing trends in gastric corpus cancer along with a declining trend in antropylorus cancer (Kampschoer et al. 1989; Maehara et al. 2000; Liu et al. 2004; Camargo et al. 2011; Holster et al. 2014; Nicolas et al. 2016; Honda et al. 2017). Consistent with this global trend, we observed a steady increase in corpus cancer relative to antropylorus cancer in the nine-year period of 2007-2015. Furthermore, our study clearly demonstrated that the increasing trend in corpus cancer relative to antropylorus cancer was observed largely in men. This phenomenon may be supported by a recent study in Japan, in which male gender was independently associated with an increasing trend in gastric corpus cancer in a multivariate analysis (Honda et al. 2017).
Decreasing trend of H. pylori infection rate may be responsible for the increasing trend in corpus cancer relative to antropylorus cancer in Japan, since the infection preferentially affects the carcinogenic potential in the antropylorus over the corpus (Martín-de-Argila et al. 1997). Furthermore, H. pylori infection causes a more marked inflammatory reaction in the gastric mucosa of men than in that of women, leading to a male predominance in the prevalence of gastric precancerous lesions (Iijima et al. 2004a; de Vries et al. 2008; Sakitani et al. 2011). Further, the advanced stage of gastritis in men could be a risk factor for GC even after H. pylori eradication due to limited reversibility of the precancerous lesions (Iijima et al. 2004b). Thus, we speculate that reductions in the H. pylori infection may lead to more prominent compositional changes in the gastric cancer subsite in men than in women. Further, a recent study indicated chronological reduction of histological gastritis in the H. pylori-positive subjects (Kamada et al. 2015), which may be associated with the increasing trend in corpus cancer.
Interestingly, a recent study from Taiwan showed that not only H. pylori-negative subjects without gastric atrophy (true H. pylori-negative) but also H. pylori-negative subjects with gastric atrophy and a history of infection were more likely to have gastric cancer in the proximal location than H. pylori-positive subjects (Tsai et al. 2017), which is consistent with our previous observation (Iijima et al. 2012). Thus, the recent widespread use of eradication therapy in Japan is also responsible for the compositional changes favorable to corpus cancer. Otherwise, potential of the involvement of Epstein-Barr virus infection (Murphy et al. 2009), the increasing prevalence of obesity (Kim et al. 2015), and wide spread use of acid-suppressive drugs such as proton pump inhibitors (Wennerstrom et al. 2017) may also have contributed to the increase in corpus cancer relative to antropylorus cancer.
Regardless of the mechanism, the increasing trend in the proportion of corpus cancer relative to antropylorus ones is of clinical relevance, as some studies have found that gastric corpus cancers show poorer prognosis after treatment than antropylorus ones (Maehara et al. 2000; Piessen et al. 2009; Petrelli et al. 2017). Furthermore, we need to be alert for the potential increase in the absolute incidence of corpus cancer in the future in Japan, as such a phenomenon has already been observed in the US and the Netherlands (Anderson et al. 2010; Camargo et al. 2011; Holster et al. 2014).
One strength of the study is that the risk of selection bias was reduced by using a near population-based database from hospital registration system. However, using registration databases might have been a limitation of this study, potentially inducing classification bias for the diagnosis of the subsites of gastric cancer, although all studies using registration databases are inevitably subject to such bias. Another limitation associated with this study is the fact that insufficient information is available regarding the trends in the H. pylori infection rate in the studied area. However, the infection rate has been observed to be steadily declining all over Japan, not only in urban areas, but also in suburban areas (Tamura et al. 2012; Shiota et al. 2013). In fact, the infection rate has steadily declined in the Tohoku district in Japan, to which Akita prefecture belongs (Shimoyama et al. 2012; Iijima et al. 2015).
In conclusion, this study demonstrated that, although the overall incidence of gastric cancer is expected to decrease in Japan with the decrease in the H. pylori infection rate (Inoue 2017), compositional changes in the gastric cancer subsite are occurring in Japan. While the proportion of cardia and antropylorus cancer is declining, that of corpus cancer is increasing, and this change has been observed to occur mainly in men. Identifying the most common sites of occurrence, may help to improve the efficiency of screening for gastric cancer using either X-ray barium or endoscopic examinations.
Conflict of Interest
The authors declare no conflict of interest.
References
-
Abrams,
J.A.,
Gonsalves,
L. &
Neugut,
A.I.
(2013) Diverging trends in the incidence of reflux-related and Helicobacter pylori-related gastric cardia cancer. J. Clin. Gastroenterol., 47, 322-327.
-
Anderson,
W.F.,
Camargo,
M.C.,
Fraumeni,
J.F. Jr.,
Correa,
P.,
Rosenberg,
P.S. &
Rabkin,
C.S.
(2010) Age-specific trends in incidence of noncardia gastric cancer in US adults. JAMA, 303, 1723-1728.
-
Blot,
W.J.,
Devesa,
S.S.,
Kneller,
R.W. &
Fraumeni,
J.F. Jr.
(1991) Rising incidence of adenocarcinoma of the esophagus and gastric cardia. JAMA, 265, 1287-1289.
-
Bor,
S.,
Vardar,
R.,
Ormeci,
N.,
Memik,
F.,
Suleymanlar,
I.,
Oguz,
D.,
Colakoglu,
S.,
Yucesoy,
M.,
Turkdogan,
K.,
Gurel,
S.,
Dogan,
I.,
Yildirim,
B.,
Goral,
V.,
Dokmeci,
G.,
Okcu,
N.,
et al. (2007) Prevalence patterns of gastric cancers in Turkey: model of a developing country with high occurrence of Helicobacter pylori. J. Gastroenterol. Hepatol., 22, 2242-2245.
-
Botterweck,
A.A.,
Schouten,
L.J.,
Volovics,
A.,
Dorant,
E. &
van Den Brandt,
P.A.
(2000) Trends in incidence of adenocarcinoma of the oesophagus and gastric cardia in ten European countries. Int. J. Epidemiol., 29, 645-654.
-
Camargo,
M.C.,
Anderson,
W.F.,
King,
J.B.,
Correa,
P.,
Thomas,
C.C.,
Rosenberg,
P.S.,
Eheman,
C.R. &
Rabkin,
C.S.
(2011) Divergent trends for gastric cancer incidence by anatomical subsite in US adults. Gut, 60, 1644-1649.
-
Cavaleiro-Pinto,
M.,
Peleteiro,
B.,
Lunet,
N. &
Barros,
H.
(2011) Helicobacter pylori infection and gastric cardia cancer: systematic review and meta-analysis. Cancer Causes Control, 22, 375-387.
-
Colquhoun,
A.,
Arnold,
M.,
Ferlay,
J.,
Goodman,
K.J.,
Forman,
D. &
Soerjomataram,
I.
(2015) Global patterns of cardia and non-cardia gastric cancer incidence in 2012. Gut, 64, 1881-1888.
-
Dassen,
A.E.,
Lemmens,
V.E.,
van de Poll-Franse,
L.V.,
Creemers,
G.J.,
Brenninkmeijer,
S.J.,
Lips,
D.J.,
Vd Wurff,
A.A.,
Bosscha,
K. &
Coebergh,
J.W.
(2010) Trends in incidence, treatment and survival of gastric adenocarcinoma between 1990 and 2007: a population-based study in the Netherlands. Eur. J. Cancer, 46, 1101-1110.
-
de Vries,
A.C.,
van Grieken,
N.C.,
Looman,
C.W.,
Casparie,
M.K.,
de Vries,
E.,
Meijer,
G.A. &
Kuipers,
E.J.
(2008) Gastric cancer risk in patients with premalignant gastric lesions: a nationwide cohort study in the Netherlands. Gastroenterology, 134, 945-952.
-
Derakhshan,
M.H.,
Malekzadeh,
R.,
Watabe,
H.,
Yazdanbod,
A.,
Fyfe,
V.,
Kazemi,
A.,
Rakhshani,
N.,
Didevar,
R.,
Sotoudeh,
M.,
Zolfeghari,
A.A. &
McColl,
K.E.
(2008) Combination of gastric atrophy, reflux symptoms and histological subtype indicates two distinct aetiologies of gastric cardia cancer. Gut, 57, 298-305.
-
Egi,
Y.,
Ito,
M.,
Tanaka,
S.,
Imagawa,
S.,
Takata,
S.,
Yoshihara,
M.,
Haruma,
K. &
Chayama,
K.
(2007) Role of Helicobacter pylori infection and chronic inflammation in gastric cancer in the cardia. Jpn. J. Clin. Oncol., 37, 365-369.
-
Ferro,
A.,
Peleteiro,
B.,
Malvezzi,
M.,
Bosetti,
C.,
Bertuccio,
P.,
Levi,
F.,
Negri,
E.,
La Vecchia,
C. &
Lunet,
N.
(2014) Worldwide trends in gastric cancer mortality (1980-2011), with predictions to 2015, and incidence by subtype. Eur. J. Cancer, 50, 1330-1344.
-
Fujiwara,
Y. &
Arakawa,
T.
(2009) Epidemiology and clinical characteristics of GERD in the Japanese population. J. Gastroenterol., 44, 518-534.
-
Hasegawa,
S.,
Yoshikawa,
T.,
Cho,
H.,
Tsuburaya,
A. &
Kobayashi,
O.
(2009) Is adenocarcinoma of the esophagogastric junction different between Japan and western countries? The incidence and clinicopathological features at a Japanese high-volume cancer center. World J. Surg., 33, 95-103.
-
Hatta,
W.,
Tong,
D.,
Lee,
Y.Y.,
Ichihara,
S.,
Uedo,
N. &
Gotoda,
T.
(2017) Different time trend and management of esophagogastric junction adenocarcinoma in three Asian countries. Dig. Endosc., 29 Suppl 2, 18-25.
-
Holster,
I.L.,
Aarts,
M.J.,
Tjwa,
E.T.,
Lemmens,
V.E. &
Kuipers,
E.J.
(2014) Trend breaks in incidence of non-cardia gastric cancer in the Netherlands. Cancer Epidemiol., 38, 9-15.
-
Honda,
M.,
Wong,
S.L.,
Healy,
M.A.,
Nakajima,
T.,
Watanabe,
M.,
Fukuma,
S.,
Fukuhara,
S. &
Ayanian,
J.Z.
(2017) Long-term trends in primary sites of gastric adenocarcinoma in Japan and the United States. J. Cancer, 8, 1935-1942.
-
Horii,
T.,
Koike,
T.,
Abe,
Y.,
Kikuchi,
R.,
Unakami,
H.,
Iijima,
K.,
Imatani,
A.,
Ohara,
S. &
Shimosegawa,
T.
(2011) Two distinct types of cancer of different origin may be mixed in gastroesophageal junction adenocarcinomas in Japan: evidence from direct evaluation of gastric acid secretion. Scand. J. Gastroenterol., 46, 710-719.
-
Iijima,
K.,
Abe,
Y.,
Koike,
T.,
Uno,
K.,
Endo,
H.,
Hatta,
W.,
Asano,
N.,
Asanuma,
K.,
Imatani,
A. &
Shimosegawa,
T.
(2012) Gastric cancers emerging after H. pylori eradication arise exclusively from non-acid-secreting areas. Tohoku J. Exp. Med., 226, 45-53.
-
Iijima,
K.,
Koike,
T.,
Abe,
Y.,
Ohara,
S.,
Nakaya,
N. &
Shimosegawa,
T.
(2015) Time series analysis of gastric acid secretion over a 20-year period in normal Japanese men. J. Gastroenterol., 50, 853-861.
-
Iijima,
K.,
Ohara,
S.,
Koike,
T.,
Sekine,
H. &
Shimosegawa,
T.
(2004a) Gastric acid secretion of normal Japanese subjects in relation to Helicobacter pylori infection, aging, and gender. Scand. J. Gastroenterol., 39, 709-716.
-
Iijima,
K.,
Sekine,
H.,
Koike,
T.,
Imatani,
A.,
Ohara,
S. &
Shimosegawa,
T.
(2004b) Long-term effect of Helicobacter pylori eradication on the reversibility of acid secretion in profound hypochlorhydria. Aliment. Pharmacol. Ther., 19, 1181-1188.
-
Inoue,
M.
(2017) Changing epidemiology of Helicobacter pylori in Japan. Gastric Cancer, 20, 3-7.
-
Inoue,
M.,
Sasazuki,
S.,
Wakai,
K.,
Suzuki,
T.,
Matsuo,
K.,
Shimazu,
T.,
Tsuji,
I.,
Tanaka,
K.,
Mizoue,
T.,
Nagata,
C.,
Tamakoshi,
A.,
Sawada,
N. &
Tsugane,
S.;
Research Group for the Development and Evaluation of Cancer Prevention Strategies in Japan
(2009) Green tea consumption and gastric cancer in Japanese: a pooled analysis of six cohort studies. Gut, 58, 1323-1332.
-
Kamada,
T.,
Haruma,
K.,
Ito,
M.,
Inoue,
K.,
Manabe,
N.,
Matsumoto,
H.,
Kusunoki,
H.,
Hata,
J.,
Yoshihara,
M.,
Sumii,
K.,
Akiyama,
T.,
Tanaka,
S.,
Shiotani,
A. &
Graham,
D.Y.
(2015) Time trends in Helicobacter pylori infection and atrophic gastritis over 40 years in Japan. Helicobacter, 20, 192-198.
-
Kamada,
T.,
Kurose,
H.,
Yamanaka,
Y.,
Manabe,
N.,
Kusunoki,
H.,
Shiotani,
A.,
Inoue,
K.,
Hata,
J.,
Matsumoto,
H.,
Akiyama,
T.,
Hirai,
T.,
Sadahira,
Y. &
Haruma,
K.
(2012) Relationship between gastroesophageal junction adenocarcinoma and Helicobacter pylori infection in Japan. Digestion, 85, 256-260.
-
Kampschoer,
G.H.,
Nakajima,
T. &
van de Velde,
C.J.
(1989) Changing patterns in gastric adenocarcinoma. Br. J. Surg., 76, 914-916.
-
Kim,
H.J.,
Kim,
N.,
Kim,
H.Y.,
Lee,
H.S.,
Yoon,
H.,
Shin,
C.M.,
Park,
Y.S.,
Park,
D.J.,
Kim,
H.H.,
Lee,
K.H.,
Kim,
Y.H.,
Kim,
H.M. &
Lee,
D.H.
(2015) Relationship between body mass index and the risk of early gastric cancer and dysplasia regardless of Helicobacter pylori infection. Gastric Cancer, 18, 762-773.
-
Kim,
J.Y.,
Lee,
H.S.,
Kim,
N.,
Shin,
C.M.,
Lee,
S.H.,
Park,
Y.S.,
Hwang,
J.H.,
Kim,
J.W.,
Jeong,
S.H.,
Lee,
D.H.,
Park,
D.J.,
Kim,
H.H. &
Jung,
H.C.
(2012) Prevalence and clinicopathologic characteristics of gastric cardia cancer in South Korea. Helicobacter, 17, 358-368.
-
Koizumi,
S.,
Motoyama,
S. &
Iijima,
K.
(2018) Is the incidence of esophageal adenocarcinoma increasing in Japan? Trends from the data of a hospital-based registration system in Akita Prefecture, Japan. J. Gastroenterol., 53, 827-833.
-
Kusano,
C.,
Gotoda,
T.,
Khor,
C.J.,
Katai,
H.,
Kato,
H.,
Taniguchi,
H. &
Shimoda,
T.
(2008) Changing trends in the proportion of adenocarcinoma of the esophagogastric junction in a large tertiary referral center in Japan. J. Gastroenterol. Hepatol., 23, 1662-1665.
-
Lau,
M.,
Le,
A. &
El-Serag,
H.B.
(2006) Noncardia gastric adenocarcinoma remains an important and deadly cancer in the United States: secular trends in incidence and survival. Am. J. Gastroenterol., 101, 2485-2492.
-
Lauren,
P.
(1965) The two hiotological main types of gastric carcinoma: diffuse and so-called intestinal type carcinoma. An attempt at a histo-clinical classification. Acta Pathol. Microbiol. Scand., 64, 31-49.
-
Liu,
Y.,
Kaneko,
S. &
Sobue,
T.
(2004) Trends in reported incidences of gastric cancer by tumour location, from 1975 to 1989 in Japan. Int. J. Epidemiol., 33, 808-815.
-
Maehara,
Y.,
Kakeji,
Y.,
Oda,
S.,
Takahashi,
I.,
Akazawa,
K. &
Sugimachi,
K.
(2000) Time trends of surgical treatment and the prognosis for Japanese patients with gastric cancer. Br. J. Cancer, 83, 986-991.
-
Martín-de-Argila,
C.,
Boixedam,
D.,
Redondom,
C.,
Redondom,
C.,
Alvarez,
I.,
Gisbert,
J.P.,
García Plaza,
A. &
Cantón,
R.
(1997) Relation between histologic subtypes and location of gastric cancer and Helicobacter pylori. Scand. J. Gastroenterol., 32, 303-307.
-
Murphy,
G.,
Pfeiffer,
R.,
Camargo,
M.C. &
Rabkin,
C.S.
(2009) Meta-analysis shows that prevalence of Epstein-Barr virus-positive gastric cancer differs based on sex and anatomic location. Gastroenterology, 137, 824-833.
-
Nicolas,
C.,
Sylvain,
M.,
Come,
L.,
Jean,
F.,
Anne-Marie,
B. &
Valerie,
J.
(2016) Trends in gastric cancer incidence: a period and birth cohort analysis in a well-defined French population. Gastric Cancer, 19, 508-514.
-
Parsonnet,
J.,
Friedman,
G.D.,
Vandersteen,
D.P.,
Chang,
Y.,
Vogelman,
J.H.,
Orentreich,
N. &
Sibley,
R.K.
(1991) Helicobacter pylori infection and the risk of gastric carcinoma. N. Engl. J. Med., 325, 1127-1131.
-
Petrelli,
F.,
Ghidini,
M.,
Barni,
S.,
Steccanella,
F.,
Sgroi,
G.,
Passalacqua,
R. &
Tomasello,
G.
(2017) Prognostic role of primary tumor location in non-metastatic gastric cancer: a systematic review and meta-analysis of 50 studies. Ann. Surg. Oncol., 24, 2655-2668.
-
Piessen,
G.,
Messager,
M.,
Leteurtre,
E.,
Jean-Pierre,
T. &
Mariette,
C.
(2009) Signet ring cell histology is an independent predictor of poor prognosis in gastric adenocarcinoma regardless of tumoral clinical presentation. Ann. Surg., 250, 878-887.
-
Sakitani,
K.,
Hirata,
Y.,
Watabe,
H.,
Yamada,
A.,
Sugimoto,
T.,
Yamaji,
Y.,
Yoshida,
H.,
Maeda,
S.,
Omata,
M. &
Koike,
K.
(2011) Gastric cancer risk according to the distribution of intestinal metaplasia and neutrophil infiltration. J. Gastroenterol. Hepatol., 26, 1570-1575.
-
Shimoyama,
T.,
Aoki,
M.,
Sasaki,
Y.,
Matsuzaka,
M.,
Nakaji,
S. &
Fukuda,
S.
(2012) ABC screening for gastric cancer is not applicable in a Japanese population with high prevalence of atrophic gastritis. Gastric Cancer, 15, 331-334.
-
Shiota,
S.,
Murakawi,
K.,
Suzuki,
R.,
Fujioka,
T. &
Yamaoka,
Y.
(2013) Helicobacter pylori infection in Japan. Expert Rev. Gastroenterol. Hepatol., 7, 35-40.
-
Tamura,
T.,
Morita,
E.,
Kondo,
T.,
Ueyama,
J.,
Tanaka,
T.,
Kida,
Y.,
Hori,
Y.,
Inoue,
S.,
Tomita,
K.,
Okada,
R.,
Kawai,
S.,
Hishida,
A.,
Naito,
M.,
Wakai,
K. &
Hamajima,
N.
(2012) Prevalence of Helicobacter pylori infection measured with urinary antibody in an urban area of Japan, 2008-2010. Nagoya J. Med. Sci., 74, 63-70.
-
Tsai,
K.F.,
Liou,
J.M.,
Chen,
M.J.,
Chen,
C.C.,
Kuo,
S.H.,
Lai,
I.R.,
Yeh,
K.H.,
Lin,
M.T.,
Wang,
H.P.,
Cheng,
A.L.,
Lin,
J.T.,
Shun,
C.T. &
Wu,
M.S.;
Taiwan Gastrointestinal Disease and Helicobacter Consortium
(2017) Distinct Clinicopathological Features and Prognosis of Helicobacter pylori Negative Gastric Cancer. PLoS One, 12, e0170942.
-
Wennerstrom,
E.C.M.,
Simonsen,
J.,
Camargo,
M.C. &
Rabkin,
C.S.
(2017) Acid-suppressing therapies and subsite-specific risk of stomach cancer. Br. J. Cancer, 116, 1234-1238.
-
World Health Organization (WHO)
(1993) International Classification of Disease for Oncology, 3rd revision, Geneve.
-
Wong,
B.C. &
Kinoshita,
Y.
(2006) Systematic review on epidemiology of gastroesophageal reflux disease in Asia. Clin. Gastroenterol. Hepatol., 4, 398-407.
-
Wu,
H.,
Rusiecki,
J.A.,
Zhu,
K.,
Potter,
J. &
Devesa,
S.S.
(2009) Stomach carcinoma incidence patterns in the United States by histologic type and anatomic site. Cancer Epidemiol. Biomarkers Prev., 18, 1945-1952.
-
Yamada,
M.,
Kushima,
R.,
Oda,
I.,
Mojtahed,
K.,
Nonaka,
S.,
Suzuki,
H.,
Yoshinaga,
S.,
Matsubara,
A.,
Taniguchi,
H.,
Sekine,
S.,
Saito,
Y. &
Shimoda,
T.
(2014) Different histological status of gastritis in superficial adenocarcinoma of the esophagogastric junction. Jpn. J. Clin. Oncol., 44, 65-71.
-
Zhou,
Y.,
Zhang,
Z.,
Zhang,
Z.,
Wu,
J.,
Ren,
D.,
Yan,
X.,
Wang,
Q.,
Wang,
Y.,
Wang,
H.,
Zhang,
J.,
Zhu,
X.,
Yang,
Y.,
Luo,
C.,
Guo,
X.,
Tang,
C.,
et al. (2008) A rising trend of gastric cardia cancer in Gansu Province of China. Cancer Lett., 269, 18-25.